










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.2 Piracicaba Abr./Jun. 2012
ORIGINAL ARTICLE
Perception of orthodontists regarding the management of root resorption – clinical and legal aspects
Luíza Valéria de Abreu MaiaI; Renata de Castro MartinsII; Mariana Mourão de Azevedo Flores PereiraIII; Maurício de Almeida CardosoIV; Leopoldino Capelozza FilhoIV; Luiz Renato ParanhosIV
IDDS, Department of Community Dentistry, School of Dentistry, Federal University of Minas Gerais (UFMG), Brazil
IIDDS, MSc, PhD, Department of Community Dentistry, School of Dentistry, Federal University of Minas Gerais (UFMG), Brazil
IIIDDS, MSc, Professor, Brazilian Dental Association - BDA/MG, Belo Horizonte, Brazil
IVDDS, MSc, PhD, Professor, Department Oral Biology, School of Dentistry, Sagrado Coração University (USC), Brazil
ABSTRACT
AIM: To evaluate the management adopted by orthodontists regarding root resorption caused by orthodontic treatment, relating it to their time of experience and the applicable legal norms.
METHODS: the study population consisted of 56 orthodontists from the city of Belo Horizonte (Minas Gerais State), and the tool to collect the data was a questionnaire with open and closed questions. Data were subjected to descriptive analysis. The association between the variables was analyzed by the chi-square test with significance level of 5%.
RESULTS: 57.6% of professionals temporarily interrupt the treatment; in the prevention and/or control, most professionals (80.4%) perform initial and periodical radiographs (every six months). Among the professionals with less than 5 years of experience as a specialist, 88.9% usually make periodic radiographic control; 100% affirmed to file the documents. No significant difference was found between dentists with different times of experience regarding the practice of archiving the documents (p = 0.271). Among those with 5-15 years of experience, 77.4% perform periodic radiographic control and 45.2% had already detected root resorption. Among those with more than 15 years of experience, 71.4% usually perform the periodic radiographic control, and 85.7% had already faced some case of root resorption in the clinical practice.
CONCLUSIONS: Although most orthodontists adopt a correct management facing the occurrence, prevention and control of root resorption associated with orthodontic treatment, the majority are unaware about existing legislation in our country.
Keywords: root resorption, perception, legal norms.
Introduction
External root resorption associated with orthodontic treatment is recognized as a clinical problem and has been a factor of controversy and concern due to the imminent risk for apical root rounding, which occurs in practically all patients under orthodontic treatment in different magnitudes. According to Petrelli1, root resorption may occur in any orthodontic treatment with any professional. Depending on the associated predisposing and etiologic factors, a resorption may occur with loss of more than one half of root length, being one of the mostundesirable side effect of orthodontic treatment. This attracts considerable interest from orthodontists, especially because of the legal aspects related to indemnities2.
The etiology of external root resorption is not yet completely understood3. It has great importance when is consequence and/or complication of certain clinical situations, such as induced tooth movement, and when related to legal implications because it is a borderline phenomenon between cost/benefit and iatrogenesis, particularly in orthodontic practice4.
The complexity of orthodontic diagnosis and treatment requires legal and ethical attitudes by the specialists from the very first contact with the patient. With the creation of the Code of Consumer Protection5, the lawsuits have increased significantly in several sectors of consumption, which brought direct consequences for Orthodontics. Therefore, the need to keep patients' documentation as complete as possible is unquestionable.
Before the beginning of the treatment, all patients (or parents/guardians) should be clearly informed that there is a real possibility of one or more teeth suffer root resorption as a consequence of orthodontic treatment6, and sign an informed consent form explaining all associated risks and factors affecting root resorption evolutionarily7-8.
The Brazilian Civil Procedure Code9 argues in Chapter VI – Evidences that the record is a document of probative force to defend the Dentist, as presented in the Art. 332: "All legal means, as well as the morally legitimate, though not specified in this Code, are able to prove the veracity of facts which substantiate the action or defense", being necessary and very important to keep a complete and organized documentation that contains the largest number of diagnostic elements and clinical procedures performed7,10-13.
Radiographic examination is the most important tool for diagnosis before starting the orthodontic treatment, and periodical radiographs also should be taken during the treatment for monitoring the occurrence of root resorption. This preventive measure has a low financial and biological cost, with a great benefit14. When the resorption is found at the beginning or during the orthodontic treatment, the best practice is to inform the patient, reevaluate the mechanics, control periodically, and warn about a possible extension in treatment time11.
In this way, this study investigated the perception of orthodontists regarding the practices adopted with respect to the prevention and/or control of the occurrence of root resorption caused by orthodontic treatment, relating it to the time of experience as specialists and to the applicable Brazilian laws.
Material and methods
This study was approved by the Ethics Committee of FOP/UNICAMP, preserving the patients and researchers of any legal and ethical drawbacks. A questionnaire with open and closed questions was sent to 150 dentists, specialists in Orthodontics, from the city of Belo Horizonte (Minas Gerais State), with a return ratio of 37.33% (n= 56). It was assured confidentiality of the information and the exclusive use of the data for research purposes. The questionnaire was sent to the participants by reply-paid mail. After receipt of the filled questionnaires, the data were compiled and distributed in percentage by means of graphs and tables that showed the results descriptively. The association between the variables was checked by chi-square test at 5% significance level.
The questionnaire was divided into two sections; the first with identification, and the second with questions about the formation, professional documentation, and the practice adopted facing the occurrence of root resorption. In the first section addressed the gender and characteristics relative to the time of experience in orthodontics. In the second section, it was questioned whether they: ask for initial and final patient documentation; perform regular radiographic control and how often this is performed; use an informed consent form before starting the treatment; know the physiological mechanisms of root resorption; had already encountered root resorption of more than a half of root length (if yes, how they managed the case); and usually file the documentation of the patients and for how long.
Results
The tabulation of personal data obtained by the questionnaires characterized the profile of the professionals composing the sample: 56 orthodontists regularly registered in the CRO-MG, predominantly male (60.7%), with different times of experience as a specialist [18 (32%) had less than 5 years, 31 (55.3%) had from 5 to 15 years, and only 7 (12.5%) had over 15 years of experience].
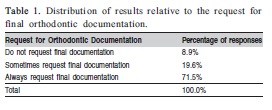
Concerning the request for initial documentation, 100% of the interviewed professionals affirmed to request the documentation before starting an orthodontic treatment. Table 1 shows the result for the request for final documentation.
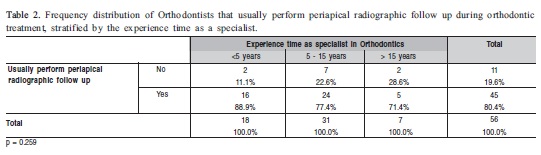
In relation to the regular periapical radiographic follow up during the orthodontic treatment, 80.4% of professionals perform this control, and 19.6% do not always do it. Table 2 presents the relationship between periodic radiographic follow up and time of experience as specialist in Orthodontics.
Among the professionals that usually perform periapical radiographic follow up, the majority (61%) makes it every six months.
Regarding the informed consent form, most interviewees (77%) have included this document, or similar, warning about the imminent risks for root resorption.
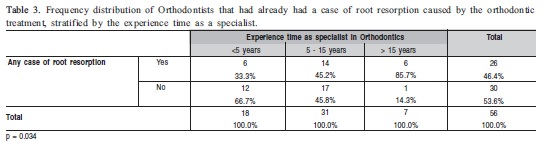
All interviewed orthodontists affirmed to know the physiological mechanisms of root resorption, and 46.4% of them reported that had already encountered a resorption case of more than a half of root length during professional exercise.
A significant association was found between the time since graduation as a specialist and the occurrence of a case of root resorption (Table 3).
Of the professionals that had already encountered a root resorption, 57.6% responded that they interrupted the treatment for a while; 19.6% continued the treatment – with lighter forces – and none of them reported to have continued normally the treatment without interrupting.
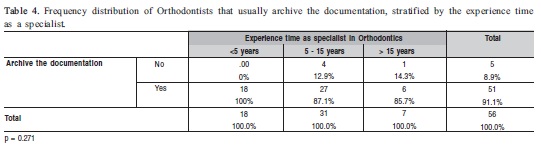
With regard to archiving practices, 91% informed that they usually archive the documentation. No significant association was found between the time since graduation as a specialist and the adoption of a routine of archiving the documentation (Table 4).
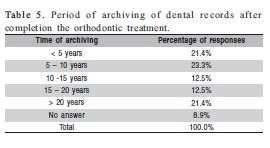
Considering the period of archiving the orthodontic documentation, there was a remarkable variation in the responses, as listed in Table 5.
Discussion
The present study investigated the perception of orthodontists regarding the ideal practice facing root resorption due to orthodontic treatment. Most studies have shown that the professionals know how to prevent the occurrence of root resorption during orthodontic treatment and how control this event when it appears8,15-17. However,some professionals are still unaware of the legal provisions relating to dental practice existing in our country.
In relation to request of initial documentation, all the professionals recognize its importance because 100% affirmed to do it. In contrast, about the final documentation, 8.9% of orthodontists responded that they do not request it, and 19.6% of them request it only sometimes. These results differ from findings of a previous study17 in which 5.7% of professionals affirmed to request the documentation after completion of treatment, and only 14.2% did not request. The request for final documentation minimizes the chances of legal problems, since it has great relevance in the follow up of orthodontic completion and post-treatment period, providing a favorable legal support15.
High-risk patients should be identified through periapical radiographs of all teeth before starting the orthodontic treatment, which are one of the most effective manners for preventing problems associated with root resorption. Radiographic control throughout the treatment is also highly recommended. Additionally, the diagnosis of oral and dental problems is part of the duty of every dentist4,18.
In view of this, we questioned about the regular periapical radiographic control during orthodontic treatment to monitor the occurrence of root resorption. By analyzing the relationship between the accomplishment of a periodic control and the time of experience in Orthodontic practice, the percentages were well distributed among the categories of the experience time (88.9% - 0-5 years; 77.4% - 5-15 years, and 71.4% - >15 years), with no correlation between these factors. Thus, the routine of performing periapical radiographic control is independent of the experience time as an orthodontist. Six months after starting the treatment is the time recommended to reevaluate radiographically the occurrence of root resorption, which may lead to temporary suspension of the treatment, thus reducing the resorption rate at the end of the orthodontic treatment4.
A preformed proof is all documentation produced by the professional, i.e., elaborated along the clinical practice for all phases of the performance as a dentist11-12,15. If produced on timely basis, the dental records may be presented by the professional to prove the existence of a fact. However, it is not enough only to have documentation; it has to have quality to safeguard the professional, containing all necessary documents that make up the patient chart7-8.
The Consent Form is an agreement between the professional and patient about a possible and licit object (orthodontic treatment), showing the conditions and limitations of the professional along with the understanding and acceptance from the patient7-8. This document should be prepared in simple language, explaining everything about the service, its indications and limitations, risks and benefits of the treatment, all the treatment options possible within the technical and biological limits, and information about the post-treatment care7-8. Most interviewees (77%) reported to include this document in the patient chart, alerting about the possible risk of root resorption as a consequence of the orthodontic treatment.
It is known that root resorption during the orthodontic treatment cannot be avoided. Nevertheless, preventive measures can avoid, in most cases, important damage to the affected tooth. Therefore, the non-adoption of these measures may characterize professional negligence19.
In the present study, all the interviewees responded to know the physiological mechanisms of root resorption; and 46.4% reported that had already faced a case of root resorption of more than a half of root length in their clinical practice. Among those with over 15 years as a specialist, 85.7% had already encountered this problem in their orthodontic clinic. The proportions of cases of root resorption increased with the increase of the experience time as an orthodontist (33.3% and 45.2%, respectively 0-5 and 5-15 years as specialist). This higher frequency of occurrence among the most experienced professionals is probably due to the performance of a larger number of services, and thus they had been more frequently exposed to the risk of this type of occurrence.
Among the professionals that had already dealt with a case of resorption of more than a half of root length in their clinical practice, 56.7% responded that they interrupted the treatment for a certain time. This procedure reduces significantly tooth shortening at the end of orthodontic treatment4; if root resorption is detected by means of intermediate radiographs, the patient is informed, as a change, interruption or termination of the treatment may be necessary.
Most professionals are not aware of the limitation of time for legal demands in relation to dental treatment. This ignorance leads to an unsafe clinical practice. The participants of the present study were not aware of the exact time that the patient has to complain to Justice in relation to performed treatment.
In the present study, 91% of the interviewees affirmed to file the orthodontic documentation of their patients. Likewise, in similar study16 with 56 dentists 98% of the sample affirmed to keep the documentation on file after completion of the treatment, and only 2% give the documentation to patients without keeping copies on file. In relation to the association between experience time and archiving of dental records, 100% of professionals with less than 5 years of experience as specialist usually archive the documentation; among those with between 5 and 15 years, 87.1% keep documentation of file, and 85.7% of professionals with over 15 years of experience affirmed to do this.
Regarding the archiving time, an expressive variation of responses was found in the present study (Table 5), whereas another study8 showed that most professionals (58.9%) filed the records after completion of treatment throughout the life. Barroso et al.17 revealed that 8.3% of professionals filed the documentation for 5 years; 3.8% for 10 years; 12.4% for 15 years; 25.5% for 20 years, and most of them (49.8%) for over 20 years. This difference in the archiving time exposed and characterized the contradictions regarding this theme, emphasizing the need for better professional orientation in relation to the Brazilian legal system. Moreover, in the Brazilian law, there is not such a term "archiving time", but a limitation time, which is frequently misunderstood.
Still on the documentation archiving, the Code of Dental Ethics20 recommends that it is the duty of the dentist to prepare and keep current the records of the patients, maintaining them on own file. The Civil Code21 establishes in three years the limitation time for civil compensation claim, while the Consumer Defense Code5 establishes this limitation in five years from the date of the discovery of the fact. Nevertheless, the professionals that responded that file the documentation for more than 20 years have corroborated the recommendation of Silva22 that states: "…the clinical records must be kept at least for twenty years…".
The occurrence of external root resorption cannot be avoided, representing a biological cost inherent to any orthodontic movement, with a variable magnitude for each individual19. This statement is consensual for to the orthodontist, but several clinicians that not work in the orthodontics area may consider this scar as an iatrogeny caused by orthodontic treatment and lead the patient to question the resorption consequent of orthodontic movement.
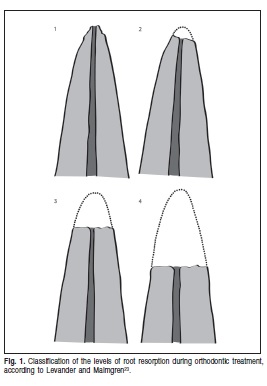
Levander and Malmgren23, in 1988, suggested a classification of the levels of root resorption during the orthodontic treatment: 1 = minimal resorption (irregular apical contour); 2 = moderate (d" 2 mm); 3 = severe resorption (> 2 mm < 1/3 root); 4 = extreme resorption (> 1/3 root), as illustrated in Figure 1.
The same knowledge allows the orthodontist to have a set of attitudes that permit the early identification of individuals and teeth predisposed to resorption before the treatment, reorientation of orthodontic procedures (once identified the process), post-treatment care of patients that suffered root resorption. This set of actions allows avoiding, in most cases, significant damages to the involved tooth or teeth.
Given the increased number of legal cases against the professionals, more experienced and newly graduated dentists should increasingly think about a professional development, particularly in Deontology to increase their knowledge of legal and ethical aspects that govern the exercise of dentistry. If not properly trained on relevant ethical and legal aspects concerning the professionals, dentists become vulnerable to litigation24.
It may be concluded that all professionals interviewed in this study request the documentation before starting an orthodontic treatment – a basic condition for professional practice. Most of these professionals perform periodic periapical radiographic control during the orthodontic treatment, but the differences in orthodontic management showed the need for dissemination of a protocol of actions among the professionals when dealing with root resorption. Most orthodontists affirm to prepare an informed consent form, indicating concern and zeal for the profession. The range of responses in relation to the archiving period of orthodontic documentation revealed the lack of knowledge about the legal provisions existing in our country, such as the Civil Code and the Consumer Defense Code.
References
1. Petrelli NE. Aspectos éticos e legais em Ortodontia. Rev Dent Press Ortod Ortop Facial. 1998; 3: 6-10. [ Links ]
2. Kaley J, Philips C. Factors related to root resorption in edgewise practice. Angle Orthod. 1991; 61: 125-32. [ Links ]
3. Capps L. Reabsorção radicular periapical e o tratamento ortodôntico. In: Rielson JAC, Gonçalves EAN. Ortodontia e ortopedia funcional dos maxilares. São Paulo: Artes Médicas; 2002. p.179-84. [ Links ]
4. Consolaro A. Reabsorções dentárias nas especialidades clínicas. Maringá: Dental Press; 2002. [ Links ]
5. Brasil. Lei no 8.078/90. Código de defesa do consumidor. Diário Oficial da União. 11 mar. 1991. [ Links ]
6. Rupp R. Root resorption related to orthodontics and other factors: a review of the literature. J Gen Orthod. 1995; 6: 25-9. [ Links ]
7. Paranhos LR, Guedes TMP, Jóias RP, Torres FC, Scanavini MA. Orientações legais aos ortodontistas: elaboração de contrato de prestação de serviços odontológicos e consentimento esclarecido - parte 2. Ortodontia SPO. 2009; 42: 237-43. [ Links ]
8. Paranhos LR, Salazar M, Torres FC, Pereira AC, Silva RF, Ramos AL. Avaliação do perfil dos profissionais da área de Ortodontia quanto às condutas legais. Dent Press J Orthod. 2011; 16: 127-34. [ Links ]
9. Brasil. Lei nº 5.869, de 11 de Janeiro de 1973. Institui o Código de Processo Civil; 1973. [ Links ]
10. Rosa FB. Dentista x Indivíduo ortodôntico: levantamento de problemas jurídicos nas últimas três décadas. J Bras Ortod Ortop Facial. 1997; 2: 14-27. [ Links ]
11. Silva M. Compêndio de Odontologia Legal. Rio de Janeiro: Editora Médica e Científica Ltda; 1997. [ Links ]
12. Calvielli ITP. Responsabilidade profissional do cirurgião-dentista. In: Silva M. Compêndio de Odontologia Legal. Rio de Janeiro: Editora Médica e Científica Ltda; 1997. p.399-411. [ Links ]
13. Silva RF, Chaves P, Paranhos LR, Lenza MA, Daruge Júnior E. Utilização de documentação ortodôntica na identificação humana. Dent Press J Orthod. 2011; 16: 52-7. [ Links ]
14. Brezniak N, Wasserstein A. Root resorption orthodontic treatment: Part I. Literature review. Am J Orthod Dentofac Orthop. 1993; 103: 62-6. [ Links ]
15. Fernandes F, Cardozo HF. Responsabilidade civil do cirurgião-dentista: o pós-tratamento ortodôntico. Rev ABO Nac. 2004; 12: 298-305. [ Links ]
16. Garbin CAS, Garbin AJI, Lelis RT. Verificação das atitudes de cirurgiõesdentistas quanto à documentação de seus pacientes. Rev Assoc Paul Cir Dent. 2006; 60: 442-5. [ Links ]
17. Barroso MG, Vedovello Filho M, Vedovello SAS, Valdrighi HC, Kuramae M, Vaz V. Responsabilidade civil do ortodontista após a terapia. RGO. 2008; 56: 67-73. [ Links ]
18. Consolaro A. Radiografias periapicais prévias ao tratamento ortodôntico. Rev Dent Press Ortod Ortop Facial. 2007; 12: 14-6. [ Links ]
19. Capelozza Filho L, Silva Filho OG. Reabsorção radicular na clínica ortodôntica: atitudes para uma conduta preventiva. Rev Dent Press Ortod Ortop Facial. 1998; 3: 104-26. [ Links ]
20. Conselho Federal de Odontologia (Brasil). Código de Ético Odontológico [cited 2007 May 7]. Rio de Janeiro. Available from: http://cfo.org.br/wpcontent/uploads/2009/09/codigo_etica.pdf. [ Links ]
21. Brasil. Novo Código Civil. Lei no 10.406/2002. Diário Oficial da União. 10 Jan 2002. [ Links ]
22. Silva M. A ética e a legislação odontológica aplicadas ao especialista em Ortodontia. In: interlandi S. Ortodontia - bases para a iniciação; 1994. Cap. 30. [ Links ]
23. Levander E, Malmgren O. Evaluation of the risks of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988; 10: 30-8. [ Links ]
24. Pereira MMAF, Silva RF, Maia LVA, Silva RHA, Daruge-Junior E, Paranhos LR. Perception of dental surgeons on the ethical and legal aspects of exercising their profession as personal and corporate entities. Braz J Oral Sci. 2011; 10: 246-9. [ Links ]
 Correspondence:
Correspondence:
Luiz Renato Paranhos
Rua Padre Roque, 958, Centro - CEP: 13800-033
Mogi Mirim - SP - Brasil
E-mail: paranhos@ortodontista.com.br
Received for publication: January 19, 2012
Accepted: April 18, 2012
