










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.2 Piracicaba Abr./Jun. 2012
ORIGINAL ARTICLE
Laser fluorescence on dental caries detection under epidemiological setting
Renato Pereira da SilvaI; Andréa Vieira AssafII; Marina Vannucci Mena RomeiroIII; Aline Sampieri Tonello BennazziIV; Gustavo Antônio Martins BrandãoV; Antonio Carlos PereiraVI
IDDS, MSc, PhD, Collaborator Professor, Department of Community Dentistry, Piracicaba Dental School, University of Campinas, Brazil
IIDDS, MSc, PhD, Professor, Department of Community Services, Fluminense Federal University, Brazil
IIIDDS, Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil
IVDDS, MSc, PhD, Substitute Professor, Department of Public Health, Federal University of Maranhão, Brazil
VDDS, MSc, PhD, Professor, Department of Orthodontics, Federal University of Pará, Brazil
VIDDS, MSc, PhD, Professor, Department of Community Dentistry, Piracicaba Dental School, University of Campinas, Brazil
ABSTRACT
AIM: To evaluate reproducibility of visual exam under artificial lighting (VI) and DIAGNOdent™ (DD) exams, their validity and their association (VI+DD) in examining occlusal dental surfaces under epidemiological setting.
METHODS: One hundred and sixty five 12-year-old schoolchildren from public schools from Piracicaba, SP, Brazil, were examined under epidemiological setting using different diagnostic criteria (D1, D1+D3 and D3). Kappa statistics was adopted for reproducibility study, while sensibility, specificity and accuracy were adopted for validity study.
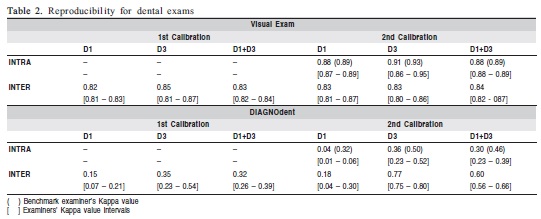
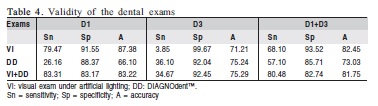
RESULTS: The intra/interexaminer Kappa for VI and DD exams at D1, D3 and D1+D3 criteria were 0.88/0.82 and 0.04/0.18, 0.91/0.85 and 0.36/0.35, 0.88/0.83 and 0.30/0.32, respectively. The VI was the most accurate exam at D1 (A=87.38%) and D1+D3 (A=82.45%) criteria, while VI+DD was the most accurate exam at D3 criterion (A=75.29%).
CONCLUSIONS: Initial caries lesions can be satisfactorily detected by VI exam, while DD exam improved the VI exam sensitivity at D1 and D3 diagnostic criteria under epidemiological setting.
Keywords: dental caries, epidemiology, dental health surveys, diagnosis; lasers.
Introduction
Dental caries is currently seen as the reflex of signs of a past or ongoing disease, resulting from the dynamic balance between de-/re-mineralization of hard dental tissues, being reversible provided it is detected early. Dental caries is a process beginning with subclinical manifestations of enamel demineralization at atomic level, culminating in spontaneous cavitation of dental surface. The closest dentists can come to measuring the carious process itself is by the clinical detection of evidence of past occurrence of this process on the dental surfaces1.
One of the challenges of modern dentistry is the early diagnosis of dental caries in occlusal tooth surfaces, particularly in children and young adults. Dentists are faced with a new epidemiological profile of this disease, characterized by a considerable portion of the world's child population being free of dental caries, with less prevalence of cavited carious lesions and greater prevalence of initial carious lesions in dental enamel, an increasing prevalence of ‘hidden caries' lesionsin dentin, and polarization of dental caries through underprivileged socioeconomic groups2-5.
New methodologies and diagnostic adjunct technologies have been suggested to improve the precision of the diagnosis of initial carious lesions5-8. Laser fluorescence measurement of the hard dental tissues has shown to be quite promising for this purpose9-10. The aim of this study was to evaluate the reproducibility and validity of dental occlusal caries exams under epidemiological setting in a 12-year-old schoolchildren group.
Material and methods
This study was approved by the Ethics Committee of Piracicaba Dental School/UNICAMP (protocol #082/2006), and conducted in accordance with resolutions 196/96 from the National Health Council of the Brazilian Ministry of Health, and 179/93 of Dental Professional Code of Ethics from Brazilian Dental Council. The study was conducted under a cross-sectional design in two stages. Participation was voluntary and written informed consent was obtained from all children's parents/caregivers.
Stage 1
The reproducibility of the visual exam under artificial lighting (VI) and the laser fluorescence exam performed with DIAGNOdent™ 2095 (KaVo, Biberach, Germany) (DD) on posterior tooth occlusal surfaces, under epidemiological conditions, was verified. One benchmark examiner and 3 experienced examiners participated. The examiners were submitted to nine 4-hour training/calibration sessions conducted by the benchmark examiner.
The sample included thirteen 12-year-old randomly selected children enrolled in a public school of Piracicaba, SP, Brazil, presenting low to high prevalence of dental caries, who had not participated in the examiners' previous clinical training. Children with fixed orthodontic appliances, severe fluorosis and enamel hypoplasia or serious systemic disease were replaced by children free of such conditions. This number of participants and the interval between the calibration sessions was based on Assaf et al. (2006)5.
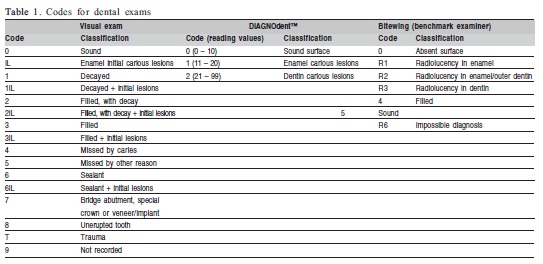
VI was performed with a flat buccal mirror, CPI probe (debris removal) and artificial lighting. All children performed supervised toothbrushing for 2 min (Bass modified with fluoridated toothpaste) before the dental examination. Each dental surface was dried for 5 s5 with a compressed air jet from a portable dental unit (Proquest Delivery System, model 4010; Compressor Technologies Ltd, Englewood, NJ, USA) before the exams. At D1 diagnostic criterion, the tooth condition was codified on ‘with initial lesions on enamel' and ‘without such condition'. At D1+D3 diagnostic criterion carious lesions (‘cavited or not' and ‘none') in enamel and/ or dentin were registered. At D3 diagnostic criterion, only dental caries in dentin or none, according to conventional World Health Organization (WHO) diagnostic criterion11 and suspected ‘hidden caries' lesions were registered. The criteria and codes adopted as D1+D3 and D3 criteria were based on Assaf et al. (2006)5 ( Table 1).
The DD exam was accomplished in accordance with manufacturer's recommendations. However the scale for interpreting and classifying its readings were defined by Zanin et al. (2005)12 ( Table 1).
The interexaminer agreement was obtained at first calibration session. For intraexaminer agreement, a second calibration session was performed after a 10-day interval to avoid bias memorization5. The weighted Kappa statistics was adopted. The data obtained were not dichotomized.
Stage 2
The sample for this stage included 165 randomly selected 12-year-old schoolchildren with the same clinical characteristics of the Stage 1. A total of 2,187 occlusal surfaces were examined. The examiner who had the highest intraexaminer Kappa values in Stage 1 was selected to conduct the exams. The validity of VI, DD and VI+DD exams was evaluated. The data were dichotomized in ‘with' and‘without caries'. The SAS System for Windows™ 9.1 (SAS Institute Inc., Cary, NC, USA) was used at both stages.
At D1 diagnostic criterion, the validation standard was the VI exam performed by benchmark examiner, while for D1+D3 diagnostic criterion, it was VI exam combined with bitewing radiography exam (VI+BW) performed by benchmark examiner. The VI+BW exam enables a more refined detection and evaluation of occlusal carious lesion depth, especially when the carious lesion is confined to dentin13. Although the value of bitewing radiograph has been questioned in epidemiological surveys14, it has been proven important in studies in which histological validation or tooth drilling is unfeasible and unethical13, especially when suspicious carious lesions are confined in enamel.
The sample DMF-T index was 1.00 (SD=1.65) according to WHO diagnostic criterion11. When enamel initial carious lesions were detected, the DMF-T index was 5.74 (SD=4.29). The difference among the DMF-T index obtained by dental exams under all diagnostic criteria was evaluated by ANOVA and Tukey's test. Significance level was set at 5%.
Results
The reproducibility for VI and DD exams is presented in Table 2. The intraexaminer agreement was ‘almost perfect' for the VI exam at all diagnostic criteria. However, the intraexaminer agreement for the DD exam was ‘slight' at D1 criterion and ‘fair' for the others criteria. The intraexaminer agreement was ‘fair' at D1 and ‘moderate' at D3 and D1+D3 criteria for the benchmark examiner performing DD exam ( Table 2). The interexaminer agreement was ‘almost perfect' for VI exam at all diagnostic criteria. For the DD exam, the interexaminer agreement was ‘slight' at D1 and ‘fair' at theothers criteria ( Table 2).
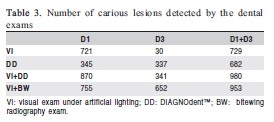
The number of carious lesions detected by VI, DD, VI+DD examinations, and by the benchmark examiner (VI+BW exam) is expressed in Table 3. The VI+DD exam detected the largest number of occlusal caries for all diagnostic criteria. A trend to overestimate caries detection was observed for VI+DD exam under D1 and D1+D3 criteria in relation to benchmark examiner ( Table 3).
The validity of the VI, DD and VI+DD examinations is presented in Table 4. At D1 criterion, the highest sensitivity was found by VI+DD exam. At D3 criterion, the highest sensitivity was found by DD exam; the highest accuracy was found for DD and VI+DD exams at this diagnostic criterion. At D1+D3 criterion, the highest value for sensitivity was found for the VI+DD exam, however the best accuracy was observed for VI exam ( Table 4).
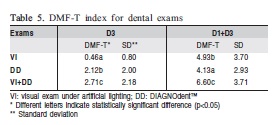
Differences among the DMF-T indexes obtained by VI, DD and VI+DD exams, at D3 and D1+D3 criteria were revealed by the Tukey's test ( Table 5).
Discussion
In view of the current dental caries development profile, seeking new methodologies and diagnostic methods that can identify its earliest stages is the intention of dentists in order to accomplish more conservative and effective treatment plans. Likewise, researchers can use different study designs and conduct studies that can prove or refute their hypotheses6-8,15-18. The D1+D3 criterion is more refined than the conventional WHO diagnostic criteria and has shown to be successful in this task2,5. In the present study, the D1+D3 criterion was responsible for a 574% increase in the DMF-T index at D3 criterion for the sample on Stage 2. Although the diagnostic complexity increases with D1+D3 in relation to D3, an increase on the accuracy of VI and VI+DD exams was verified. A further step searching for a more accurate dental caries diagnostic is the addition of diagnostic adjuncts to the traditional visual clinical exam.
The present study evaluated the reproducibility and validity of caries detection by laser fluorescence according to the D1, D3 and D1+D3 diagnostic criteria, under epidemiological setting. This adjunct technology is based on the principle that demineralized dental surfaces colonized by bacteria and exposed to their metabolites exhibit an increased fluorescence in comparison with sound enamel when excited by a diode laser beam (655 nm) emitted by DIAGNOdent™. Because of its high sensitivity, but low specificity, the combination of DIAGNOdent™ with traditional diagnostic methods, such visual exam, is justified10,19. However a great deal of the studies evaluating this technology is performed under laboratorial and/or clinical conditions, not under epidemiological conditions. This way, the preliminary comparisons made in this study, as well its design, require caution in both interpretation and generalization.
The intraexaminer reproducibility of DD examination concerning all diagnostic criteria was lower than in in vitro studies16 and in vivo clinical trials12,17. This can reflect the difficulty to keep an adequate oral hygiene level in epidemiological conditions and that the presence of plaque on dental occlusal surfaces worsens DIAGNOdent™ accuracy20-21. Although DIAGNOdent's™ manufacturer recommends previous professional prophylaxis, the previous supervised toothbrushing adopted in this study can be implemented with similar success20. After that, vigorous oral rinse was performed to remove any toothpaste residues, which could interfere on DIAGNOdent™ readings20-21. Drying of dental surface to be examined was also performed as recommended5,22. The Kappa values of the second calibration session for interexaminer agreement were higher than those of the first session, suggesting that the oral hygiene level improved during this period. The reproducibility of DD exam contraindicates its use on epidemiological surveys. The reproducibility was more influenced by the examination setting than the examiners' ability to operate the DIAGNOdent™ device.
An accuracy of at least 80% was obtained by VI and VI+DD exams at D1 and D1+D3 criteria. The lower values of sensitivity and accuracy for dental examinations at D3 criterion are due to the validation method adopted (VI+BW exam), which is more sensitive than the dental examinations adopted, detecting dentin carious lesions under sound enamel, which are not detectable by the visual exam alone. So, the sensitivity was extremely low for VI examination at D3 criterion. The assertive that DD exam should be used as an adjunct diagnostic tool6,8,10,18 is corroborated by the sensitivity values for VI+DD exam under D1 and D1+D3 criteria. However the accuracy values of VI+DD exam were slightly inferior to the accuracy of VI exam at D1 and D3 criteria. Although an increasing VI exam sensitivity can be seen, the good results of the DD exam found in clinical setting17 were not found in the present study.
As in a previous study by Pereira et al.9, data available from multiple diagnostic methods did not improve the accuracy of examiners, but it influenced the number of surfaces indicated for operative treatment. For D1 and D1+D3 criteria, the combination of DD with VI decreased its accuracy. However, the number of surfaces indicated to treat was overestimated with VI+DD exam in relation to benchmark examiner. The DD exam increased the accuracy of VI for D3 criteria. Discrepant amounts of caries detected between dental exams and benchmark examiner for D3 criterion was due to validation method. For D3 criterion, VI+BW exam allowed detecting more dental caries than the other diagnostic methods.
The financial costs of the inclusion of the bitewing radiograph and DIAGNOdent™ examinations in dental caries surveys are limitations to the use of these adjuncts on such surveys. However, when the public health services support financially those epidemiological surveys such limitations can be solved. In epidemiological dental caries surveys, the bitewing radiograph must be used for suspicious cases only due to the ethical concerns.
Another limitation of this study was the validation process. Facing to the actual prevalence of initial carious lesions in enamel, treatable by preventive proceedings, other ways to validate diagnostic methods, that are not histological (extracting teeth) or biopsy (drilling suspicious surfaces) are necessary. The VI+BW exam adopted in this study, although it is far from the ideal method, was one of them. More and more, detection of initial carious lesions is necessary for planning actions in oral public health services3. A meticulous visual examination using D1 criterion was sufficient for this purpose, corroborating with Heinrich-Weltzien et al.17. For D3 and D1+D3 criteria, the DIAGNOdent™ showed its potential to supplement the VI exam on epidemiological surveys18,23. However, caution and additional in vivo studies, under epidemiological settings, are needed to corroborate or refute those results.
The results of the present study reveal that a meticulous visual exam is sufficient to detect initial carious lesions in enamel using D1 diagnostic criterion. It was also observed that the combination of laser fluorescence and visual exam improved its sensitivity according to D1 and D3 diagnostic criteria under epidemiological setting.
Acknowledgements
The authors would like to thanks the volunteers for their collaboration, the PROEX/CAPES-UNICAMP for the first author scholarship and the FAPESP for the financial support (grants #06/58881-9).
References
1. Featherstone JDB. The continuum of dental caries – evidence for a dynamic disease process. J Dent Res. 2004; 83 (Spec Iss C): C39-42.
2. Ricketts D, Kidd E, Weerheijm Ê, Soet H. Hidden caries: What is it? Does it exist? Does it matter? Int Dent Educ. 1997; 47: 259-65. [ Links ]
3. Vehkalahti M, Tarkkonen L, Varsio S, Heikkilä P. Decrease in and polarization of dental caries occurrence among child and youth populations, 1976-1993. Caries Res. 1997; 31: 161-5. [ Links ]
4. Kassawara ABC, Assaf AV, Meneghim MC, Pereira AC, Topping G, Levin K, et al. Comparison of epidemiological evaluations under different caries diagnostic thresholds. Oral Health Prev Dent. 2007; 5: 137-44. [ Links ]
5. Assaf AV, Meneghim MC, Zanin L, Cortelazzi KL, Pereira AC, Ambrosano GMB. Effect of different diagnostic thresholds on dental caries calibration. J Public Health Dent. 2006; 66: 17-22. [ Links ]
6. da Silva RP, Assaf AV, Pereira SM, Mialhe FL, Ambrosano GM, Meneghim Mde C, et al. Validity of caries-detection methods under epidemiological setting. Am J Dent. 2011; 24: 363-6. [ Links ]
7. da Silva RP, Assaf AV, Pereira SM, Ambrosano GM, Mialhe FL, Pereira AC. Reproducibility of adjunct techniques for diagnosis of dental caries in an epidemiological situation. Oral Health Prev Dent. 2011; 9: 251-9. [ Links ]
8. Duruturk L, Ciftçi A, Baharoglu S, Oztuna D. Clinical evaluation of DIAGNOdent in detection of occlusal caries in newly erupted noncavitated first permanent molars in caries-active children. Oper Dent. 2011; 36: 348-55. [ Links ]
9. Pereira AC, Eggertsson H, Martinez-Mier EA, Mialhe FL, Eckert GJ, Zero DT. Validity of caries detection on occlusal surfaces and treatment decisions based on results from multiple caries-detection methods. Eur J Oral Sci. 2009; 117: 51-7. [ Links ]
10. Bader JD, Shugars DA. A systematic review of the performance of a laser fluorescence device for detecting caries. J Am Dent Assoc. 2004; 135: 1413-26. [ Links ]
11. World Health Organization. Oral health surveys, basic methods. 4th ed. Geneve: WHO; 1997. [ Links ]
12. Zanin L, Meneghim MC, Assaf AV, Pardi V, Pereira AC, Mialhe FL. Depth of occlusal caries assessed clinically by fluorescence laser, conventional and digital radiographic methods. Braz J Oral Sci. 2005; 4: 735-40. [ Links ]
13. Wenzel A. Bitewing and digital bitewing radiography for detection of caries lesions. J Dent Res. 2004; 83 (Spec Iss C): C72-5. [ Links ]
14. Bloemendal E, de Vet HCW, Bouter LM. The value of bitewing radiographs in epidemiological caries research: a systematic review of the literature. J Dent. 2004; 32: 255-64. [ Links ]
15. Chesters RK, Ellwood RP, Biesbrock AR, Smith SR. Potential modern alternative designs for caries clinical trials (CCTs) and how these can be validated against the conventional model. J Dent Res. 2004; 83 (Spec Iss C): C122-4. [ Links ]
16. Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG. Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res. 2006; 40: 194-201. [ Links ]
17. Heinrich-Weltzien R, Weerheijm KL, Kühnisch J, Oehme T, Stösser L. Clinical evaluation of visual, radiographic, and laser fluorescence methods for detection of occlusal caries. ASCD J Dent Child. 2002; 69: 127-32. [ Links ]
18. Rando-Meirelles MP, de Sousa Mda L. Using laser fluorescence (DIAGNOdent) in surveys for the detection of noncavitated occlusal dentine caries. Community Dent Health. 2011; 28: 17-21. [ Links ]
19. Matos R, Novaes TF, Braga MM, Siqueira WL, Duarte DA, Mendes FM. Clinical performance of two fluorescence-based methods in detecting occlusal caries lesions in primary teeth. Caries Res. 2011;45: 294-302. [ Links ]
20. Lussi A, Reich E. The influence of toothpastes and prophylaxis pastes on fluorescence measurements for caries detection in vitro. Eur J Oral Sci. 2005; 113: 141-4. [ Links ]
21. Diniz MB, Sciasci P, Rodrigues JA, Lussi A, Cordeiro RC. Influence of different professional prophylactic methods on fluorescence measurements for detection of occlusal caries. Caries Res. 2011;45: 264-8. [ Links ]
22. Pinelli C, Loffredo Lde C, Serra MC. Effect of drying on the reproducibility of DIAGNOdent to detect caries-like lesions. Braz Dent J. 2010; 21: 405-10. [ Links ]
23. Rodrigues JA, Hug I, Neuhaus KW, Lussi A. Light-emitting diode and laser fluorescence-based devices in detecting occlusal caries. J Biomed Opt. 2011; 16: 107003. [ Links ]
 Correspondence:
Correspondence:
Antonio Carlos Pereira
Faculdade de Odontologia de Piracicaba, UNICAMP
Av Limeira, 901, Areião - CEP: 13414-903
Piracicaba, SP, Brasil
E-mail: apereira@fop.unicamp.br
Received for publication: April 12, 2012
Accepted: May 04, 2012
