










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.3 Piracicaba Jul./Set. 2012
ORIGINAL ARTICLE
Influence of wrong determination of occlusal plane in maxillary advancement: a model surgery study
Maximiana Cristina de Souza MaliskaI; Robson GarciaII; Roger Willian Fernandes MoreiraIII
IDDS, Master student, Oral and Maxillofacial Surgery Division, Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil
IIDDS, MS, PhD, Collaborative Researcher, Oral and Maxillofacial Surgery Division, Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil
IIIDDS, MS, PhD, Associate professor, Oral and Maxillofacial Surgery Division, Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil
ABSTRACT
AIM: This study investigated whether an occlusal plane error of acquisition can influence on the treatment planning of maxillary advancement in double-jaw surgeries.
METHODS: Advancement of 8 and 4 mm were studied in different groups. For each group, 20 maxillary models were mounted by a 13-degree platform with superior articulator arm (control group) and other 20 models mounted with 7 degrees (study group). Intermediate splint was obtained by cast surgery performed in the control group. All the 40 maxillary models were remounted with this intermediate splint. Measurements in vertical and anteroposterior planes were accomplished pre- and postoperatively by digital caliper rule and Erickson's platform.
RESULTS: Statistical analysis showed significant results in two planes. The alteration of occlusal plane from 13 degrees to 7 degrees modified the final result in vertical measurements: right molar from group of 4 mm advancement (p<0.0001) and left molar from two groups of advancement (p<0.0001); in anteroposterior measurements: maxillary incisor from 4 mm of advancement (p<0.005) and 8 mm of advancement (p<0.0001).
CONCLUSIONS: Notwithstanding the importance of statistical findings, the result probably did not show clinical relevance in orthognathic surgery. Clinical studies addressing these concerns must be supplied in scientific literature.
Keywords: occlusal plane, bimaxillary surgery, face bow, model surgery.
Introduction
Correction of dentoskeletal deformities of the jaws, where double-jaw surgery is necessary to establish optimal functional and esthetic relationships, requires accurate diagnoses and proper treatment planning. Planning for orthognathic surgery involves integrating diagnostic information from patient examination, cephalometric radiograph, and dental models. The Frankfort horizontal plane is a common reference plane accepted to link all this information and it is universally represented by the upper arm of the articulator1. It is imperative that the angle between the occlusal plane and the Frankfort horizontal plane in the patient be the same as the angle between the occlusal plane of the maxillary model to the upper arm of the articulator2.
An important step to achieve excellence in orthognathic surgery concerns model surgery, which can provide a more accurate assessment of the surgical movements, as it allows assessment in all three dimensions3. Face bow is the device that can transfer maxillary position in relation to Frankfort plane from the patient to thesemi-adjustable articulator. Unfortunately, this face bow registration method often creates inaccuracies in the mounted maxillary model position.
Many authors1,4-5 studied different face bows recordings to investigate the inaccuracies presented in the maxillary mounted model in the articulator. Ellis et al. 2 developed a simple technique of checking the angle between the occlusal plane and Frankfort horizontal. With the use of a compass, recordings in the maxillary mounted model were transferred to cephalometric tracings. A line was drawn tangent to the compass recordings, and the angle between this line and the Frankfort line was measured.
An important average value of 7 degrees of inaccuracy was established with respect to the angulation of the occlusal plane. However, traditional face bow mounting of dental models remains with different and difficult inaccuracies to be corrected6.
The three-dimensional position of patient's external meatuses or condyles may be asymmetric from side to side; a shift could happen when tightening the bolts or screws of the face bow components, which show the sensibility of the device; some anatomic aberrations or absent structures may be present and are not reproducible on the articulator6.
In regard of face bow recording inaccuracies, the purpose of this study was to analyze the influence of a 6-degree hypothetical error of occlusal plane registration in model surgery with maxillary advancement of 4 and 8 mm.
Material and methods
Maxillary and mandibular plaster models were obtained from a dental manikin with corrected dental alignment. Twenty models for each group, control and study, were necessary for this study. The models had a specific number to permit the use of the same model for maxillary advancement of 4 and 8 mm. The same articulator adjusted with the recommended arbitrary average values of 15° and 30°, respectively for Bennett angle and eminence angle, was used for mounting all samples.
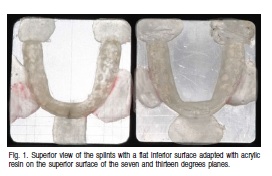
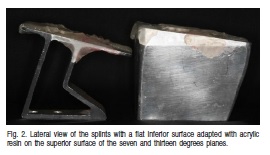
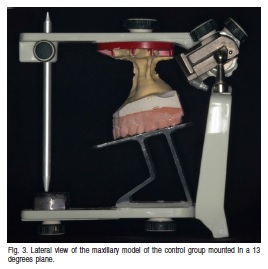
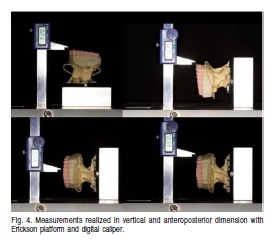
Maxillary models of the control and study groups were firstly mounted in 13- and 7-degree planes retrospecti-vely from two splints with a flat inferior surface adapted on the superior surface of the planes to give a standardized position of the models (Figures 1-3). This standardization was checked by measurements made in specific vertical and anteroposterior points: the tip of the upper incisor and the mesiobuccal cusps of the left and right first molars in the vertical plane, and the most convex point of the upper incisor in the anteroposterior plane (Figure 4). Measurements were performed with Erickson's platform and digital caliper similar to the Ellis technique described5. Models that could not achieve an error margin of 0.05 mm in the average of measurements of all mounting models were remounted.
A malocclusion splint was obtained by an anteroposterior discrepancy simulation of about 4 mm of mandibular prognathism. The normal (control group) and altered (study group) maxillary plane angulation data was transferred to mandibular models: two mandibular models were mounted by the adapted malocclusion splint and according to each maxillary model angulation of 13 and 7 degrees.
Maxillary advancement of 4 and 8 mm were performed during model surgery from two extra models mounted in a 13-degree plane (control group) according to standardized procedures. A mandible with 13 degrees of mandibular occlusal angle and operated models as cited above was used to the confection of the intermediate splints (Figure 5).

All the samples of the control and study groups, totalizing 40 maxillary models, were remounted according to intermediate splint from maxillary advancement of 4 mm. It is important to highlight that it was used the mandible of 13-degree mandibular plane angle to set the control group and the mandible of 7-degree mandibular plane angle to set the study group. The same measurements performed in vertical and anteroposterior plane for standardization was applied and registered as post-operatory values. Forty maxillary models for advancement group of 8 mm were remounted, and measurements were registered in the same manner. Data was submitted to Double F test for homogeneity of variances, and to Shapiro-Wilk test for normality of variances followed by Student's t-test. The level ofsignificance adopted in the study was 0.05, and calculations were accomplished by the SAS system (SAS Institute Inc. The SAS System, release 9.2 – TS Level 2MO. SAS Institute Inc., Cary, NC, USA).
Results
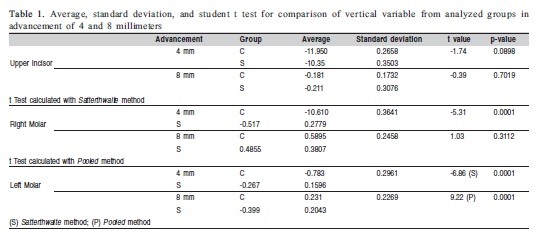
Vertical variable did not show statistical significance between control and study groups in the tip of upper incisor from advancement of 4 and 8 mm and mesiobuccal cusp of the right first molar from maxillary advancement of 8 mm. However, there were subsidies to affirm that the mean difference of the measures were different between control and study groups in mesiobuccal cusps of the right molar from maxillary advancement of 4 mm (p<0.0001) and the left molar from 4 and 8 mm (p<0.0001) of advancement, as seen in Table 1.
In the clinical practice, the flattening of 6 degrees of occlusal plane angle could downward the first molars cusps of 0.55 mm in right molar with advancement of 4 mm compared with upward movement showed with angulation of 13 degrees observed in all control groups from vertical variable. The left molar demonstrated a similar course: a downward movement of 0.52 and 0.62 mm in retrospectively 4 and 8 mm of advancement.
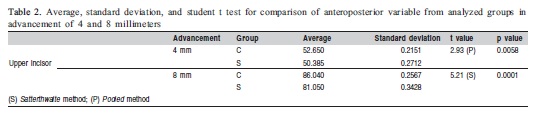
Anteroposterior variable showed statistically significant difference between control and study groups in both 4 and 8 mm advancements (p<0.005; p<0.0001), as seen in Table 2.
Study groups in both maxillary advancements did not follow the predicted advancement in control groups. The study group advanced 0.23 mm less than the control group in 4 mm analysis and 0.5 mm less than control group in 8 mm analysis.
Discussion
Several studies have been designed to compare the occlusal plane angulation obtained in the articulator with the occlusal plane in the patient. Results showed great variation about type or brand of the articulator and the face bow used. The differences in methodologies applied increase the variability of the results, even though all studies demonstrated different angulations between patient and position of transferred maxilla in the articulator.
O'Malley and Milosevic5 found 1.9 degrees of difference between the occlusal plane of patients and Whipmix articulator, 5.2 degrees of difference for Denar articulator, and 6.5 for Dentatus articulator. Gateno et al.1 showed statistically difference to SAM's face bow: 7.8 degrees and 4.4 degrees to Erickon's face bow.
This study demonstrated statistically significant values for both planes studied: vertical and anteroposterior in all measures analyzed, except for the right molar in 8 mm advancement, considering a hypothetic error of 6 degrees of occlusal plane transference. The choice of 6 degrees of inaccuracy is perfectly acceptable for analysis of the influence in planning the orthognathic movements, as seen in previous studies, cited above.
A variation of vertical movement was expected in this upper incisor variable because the condyle axis determines the aperture amplitude in articulator, notwithstanding the results were not statistically significant. During splint fabrication, special attention was dedicate to the incisor position, so their unaltered position can be explained by the axis formed by the tip of crowns in maxillary incisor that transfer the amplitude movement for this incisor axis, thus determining a variation in first molar's vertical position as demonstrated in this study.
The movement that first molars in study group did not exert to accompany the vertical movement in control group, or a flattening of occlusal plane, can be considered a counterclockwise rotation of occlusal plane. According to Wolford et al.7, some important anatomic alterations were found in this type of movement such as anterior projection of chin, increase of maxillary incisor inclination and decrease of mandibular incisor inclination, increase in the posterior facial height, and flattening of mandibular occlusal plane.
Esthetic relationships of the jaws with other facial structures in counterclockwise rotation are also determined by the center of rotation adopted for the movement. This study adopted the center of rotation at the maxillary incisor edge, so the perinasal area, subnasale area, and the nasal tip could move posteriorly and the chin could come forward. On the other hand, if rotation is around point A or higher, then the perinasal area and the nose could be less affected, but the maxillary incisor edges could come forward, thus increasing the anteroposterior support to the upper lip8.
No study has yet demonstrated a relationship between the decrease of vertical height in first molars in a counterclockwise rotation and the influence in some soft tissue point. Coleta et al.9 showed results with different values of hard and soft tissue after a counterclockwise movement adjunct with TMJ reconstruction in vertical and horizontal planes, unfortunately, not applicable in this study.
Doubts about the clinical influence of 0.5 mm of vertical height decrease in 6 degrees of flattening occlusal plane founded in this study still persist. Probably, this value, which is even statistically significant, could not represent the real problems in clinical esthetic planning and the results in orthognathic surgery.
Maxillary advancement induces some important changes in soft tissue, mainly, in the nasal area and upper lip. Rotation and translation from the subnasale point are typical movements that the upper lip exerts when maxillary advancement is performed, followed by the advancement of the tip of the upper incisor in a soft-hard tissue proportion of 0.4:1 and 0.9:110-11.
Jensen et al.12 found 78% of soft-hard tissue alteration measured in the most projected point in the upper lip (labrale superius) in a 1.9 mm advancement from the tip of maxillary incisor. In addition to this tendency, Stella et al.13 observed that postoperative upper lip had a pattern more than 25% thinner than pre-operative upper lip in maxillary advancements13.
Anteroposterior upper incisor lack of projection induces errors of prediction. Soft tissue never followed totally hard tissue in maxillary advancement, even with different points of reference and methods of investigation. If transference of occlusal plane has inaccuracies, probably the amount of advancement planned will not be the expected. The same doubt still remains about clinical influence of little lack of movements predicted in the orthognathic surgery results.
Developments in different three-dimensional technologies, such as multiplanar computed tomography and magnetic resonance imaging scanning and three-dimensional photography modalities, permit fusion of images that can provide an accurate and realistic prediction of model treatment planning in orthognathic surgery14. Digital model surgery and the obtainment of prototyped wafers for orthognathic surgery became an accurate and effortless alternative to model surgery. However, these new technologies are not yet achievable for oral and maxillofacial surgeons from some developing countries. In these cases, manual model surgery still remains the only alternative to achieve excellent results in orthognathic surgery15.
The authors believe that sensible errors from acquisition of occlusal plane with face bow and semi-adjustable articulator technique will not produce serious problems with facial esthetic and functional outcomes in bimaxillary surgery that requires pure advancement of maxilla. A limitation of this study is that only one movement was analyzed: maxillary advancement. Perhaps, with the exception of non-asymmetric cases, or in patients with jaw aberrations, a Camper table could be used as alternative mounting of maxillary model in the articulator. Analysis of other orthognathic movements and clinical studies will be necessary to make it clearer and feasible the use of Camper table as an alternative technique.
References
1. Gateno J, Forrest KK,Camp B. A comparison of 3 methods of face-bow transfer recording: implications for orthognathic surgery. 2001; 59: 635-40.
2. Ellis E III. Accuracy of model surgery: evaluation of an old technique and introduction of a new one. J Oral Maxillofac Surg. 1990; 48: 1161-7. [ Links ]
3. Ellis E III, Tharanon W, Gambrell K. Accuracy of face-bow transfer: effect on surgical prediction and postsurgical result. J Oral Maxillofac Surg. 1992; 50: 562-7. [ Links ]
4. Bamber MA, Firouzai R, Harris M, Linney A. A comparative study of two arbitrary face-bow transfer systems for orthognathic surgery planning. 1996; 25: 339-43.
5. O'Malley AM, Milosevic A. Comparison of three facebow/semi-adjustable articulator systems for planning orthognathic surgery. Br J Oral Maxillofac Surg. 2000; 38: 185-90. [ Links ]
6. Wolford LM, Galiano A. A simple and accurate method for mounting models in orthognathic surgery. J Oral Maxillofac Surg. 2007; 65: 1406-9. [ Links ]
7. Wolford LM, Chemello PD, Hilliard F. Occlusal plane alteration in orthognathic surgery – part I: Effects on function and esthetics. Am J Orthod Dentofac Orthop. 1994; 106: 304-16.
8. Reyneke JP, Evans WG. Surgical manipulation of the occlusal plane. Int J Adult Orthod Orthognath Surg. 1990; 5: 99. [ Links ]
9. Coleta KED, Wolford LM, Gonçalves JR, dos Santos Pinto A, Cassano DS, Gonçalves DAG. Maxillo-mandibular counterclockwise rotation and mandibular advancement with TMJ concepts total joint prostheses –part IV –Soft tissue response. Int J Oral Maxillofac Surg. 2009; 38: 637-46.
10. Carlotti AE, Aschaffenburg PH, Schendel SA. Facial changes associated with surgical advancement of the lip and maxilla. J Oral Maxillofac Surg. 1986; 44: 593-6. [ Links ]
11. Dann JJ, Fonseca RJ, Bell WH. Soft tissue changes associated with total maxillary advancement: a preliminary study. J Oral Surg. 1976; 34: 19-23. [ Links ]
12. Jensen AC, Sinclair PM, Wolford LM. Soft tissue changes associated with double jaw surgery. Am J Orthod Dentofacial Orthop. 1992; 101: 266-75. [ Links ]
13. Stella JP, Streater MR, Epker BN, Sinn DP. Predictability of upper lip soft tissue changes with maxillary advancement. J Oral Maxillofac Surg. 1989; 47: 697-703. [ Links ]
14. Plooij JM, Maal TJ, Haers P, Borstlap WA, Kuijpers-Jaqtman AM, Bergé SJ. Digital three-dimensional image fusion processes for planning and evaluating orthodontics and orthognathic surgery. A systematic review. Int J Oral Maxillofac Surg. 2011; 40: 341-52. [ Links ]
15. McCormick SU, Drew SJ. Virtual model surgery for efficient planning and surgical performance. J Oral Maxillofac Surg. 2011; 69:638-44. [ Links ]
 Correspondence:
Correspondence:
Maximiana Cristina de Souza Maliska
Departamento de Cirurgia Buco-Maxilo-Facial
Faculdade de Odontologia de Piracicaba,
Caixa Postal 52, Universidade Estadual de Campinas
CEP: 13414-903, Piracicaba, SP, Brasil
E-mail: maximaliska@yahoo.com.br
Received for publication: February 23, 2012
Accepted: May 17, 2012
