










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.3 Piracicaba Jul./Set. 2012
ORIGINAL ARTICLE
Topographic relationship of impacted third molars and mandibular canal: correlation of panoramic radiograph signs and CBCT images
Eduardo Luiz DelamareI; Gabriela Salatino LiedkeII; Mariana Boessio VizzottoIII; Heraldo Luis Dias da SilveiraIV; Tais Weber Furlanetto de AzambujaIV; Heloisa Emilia Dias da SilveiraV
IBDS, MSc; Private practice; Porto Alegre, RS, Brazil
IIBDS, MSc; PhD Student; Department of Surgery and Orthopedics, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
IIIBDS, MSc, PhD; Department of Surgery and Orthopedics, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
IVBDS, MSc, PhD; Associate Professor; Department of Surgery and Orthopedics, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
VBDS, MSc, PhD; Professor and Department Head; Department of Surgery and Orthopedics, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
ABSTRACT
AIM: This study evaluated the proximity and relation of impacted lower third molars and mandibular canal on panoramic radiography.
METHODS: Radiographic signals associated with proximity of structures and Pell & Gregory and Winter classifications of 78 impacted teeth were analyzed and compared with CBCT images (gold standard). The associations between the findings were tested with Pearson's chi-square.
RESULTS: Direct contact between structures was observed in 85% of cases of radiolucent band over roots.
CONCLUSIONS: Radiolucent band over roots is the image more associated with direct contact between structures and the one that indicates lingual positioning of the canal more consistently. Some categories of Pell & Gregory and Winter classifications suggested signs of the topographic location of the mandibular canal.
Keywords: radiography, tomography, third molar.
Introduction
Surgical removal of impacted lower third molars is common procedure in clinical dental practice and might be associated with post-operative complications related to inferior alveolar nerve (IAN) injuries, and the risk of complications is sensibly increased whenever direct contact between the nerve and the impacted molar root is observed1-3. Therefore, a precise topographic evaluation of the mandibular canal and the surrounding molars is deemed essential during preoperatory planning1,3-4.
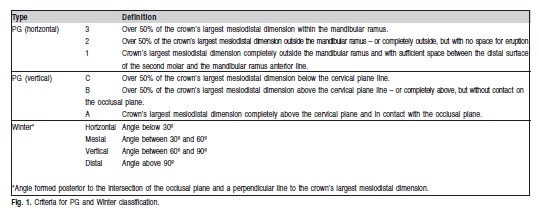
The panoramic radiograph is routinely used as an auxiliary examination for treatment planning of lower third molar removal, due to its wide availability, low cost and relatively low exposure dose5. For this kind of investigation, four signals have been more consistently associated with direct contact between mandibular canal and molar roots: interruption of the radiopaque line of the canal wall; radiolucent band over roots; deflection of the canal around the apices; and narrowing of the roots6-12. Another traditionally accepted option for estimations of difficulty and risk during lower third molar removal is the evaluation of the impacted tooth according to the classification of Pell & Gregory (PG) and Winter13. PG classification distributes impacted molars in three categories according to their vertical positioning (related to the occlusal and cervical plane of adjacent molars) and three horizontal categories (related to the mandibular ascending ramus). Winter classification is divided in four categories based on tilting of the impacted molar in relation to its longitudinal axis.
Whenever these classifications and signals point towards categories correlated with higher difficulty levels, as well as with proximity between structures observed in panoramic radiographs, it should be noticed that the buccolingual aspect cannot be visualized. Indeed, a further assessment regarding surgical removal of impacted lower third molars observed by Ghaeminia et al.14 is that lingual positioning of the mandibular canal is significantly linked with injuries to the IAN.
Due to the recent development and spread of cone beam computed tomography (CBCT), three-dimensional images are becoming more easily available in dentistry, allowing extra investigation of the mandibular canal and surrounding molars. Tantanapornkul et al.7 concluded that CBCT was significantly superior to panoramic images in predicting neurovascular bundle exposure during extraction of impacted mandibular third molar. Although CBCT allows such evaluation, panoramic radiography is still often the first imaging method requested to the investigation of third molars5. Moreover, ALARA Principle should be a concern among professionals, seeking to extract maximum information from an imaging study, avoiding further exposure15.
Thus, this study aimed to evaluate more deeply the association between impacted lower third molars and mandibular canal based on radiographic signals suggesting proximity of structures and the PG and Winter classifications, using CBCT images as references, to increase the information that might be gather from panoramic radiographs.
Material and methods
All patients who attended to Oral Surgery Department for third molar removal during one year and had at least one impacted molar and one of the radiographic signals associated with proximity of structures – interruption of the radiopaque line of the canal wall; radiolucent band over roots; deflection of the canal around the apices; and narrowing of the roots - were asked a tomographic examination. For all those cases in which the impacted molar exhibited two radiographic findings or more, the most striking feature has been selected. A total of 78 impacted teeth (from 41 patients - 17 women; 24 men) comprised the sample. All of them read and signed informed consent forms and this study has been approved by the Institution Ethical and Research Boards.
Tomographic images were obtained with an i-CAT tomography scanner (Imaging Sciences International, Hatfield, PA, USA), and a 0.25 mm voxel has been used. The conventional panoramic radiographs were digitized with a transparency flatbed scanner (UMAX 2400S) and resolution of 300 dpi.
All randomly coded images were analyzed with a 19" LCD screen by three calibrated examiners from the Oral Radiology department (Kappa scores over 0.7 for intra and inter-observer reproducibility). Image J version 1.42 (National Institutes of Health, Bethesda, MD, USA) software has been used to perform PG and Winter classifications in the panoramic views (Figure 1). I-CAT Vision v.7.2.4. Implant Screen function has been chosen to carry out the tomographic examination. Identification of contact between structures was classified in: 1 – Present; 2 – Absent; and the topographic positioning of the mandibular canal as seen in the buccolingual aspect was divided in: 1 – Inferior; 2 – Lingual; 3 – Inter-radicular; 4 – Buccal.
Data was processed and analyzed with the Statistical Package for Social Sciences, version 15.0 (SPSS Inc., Chicago, IL, USA). The association between the radiographic signals and the classifications of PG and Winter with the tomographic images have been tested with Pearson's chi-square test.

Results
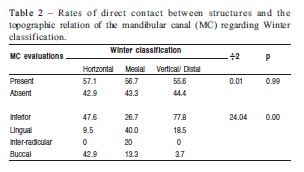
Analyses of Table 1 shows that direct contact between structures could be observed in 85% of cases of radiolucent band over roots (p<0.05); on the other hand, deflection of the canal demonstrated the smallest amount association with contact of molars and mandibular canal (30%). The connection between the radiographic signals and the topographic relation of the mandibular canal (visualized on CBCT images) reveals that the lingual positioning of the canal has proven to be more closely associated with radiolucent band over roots.
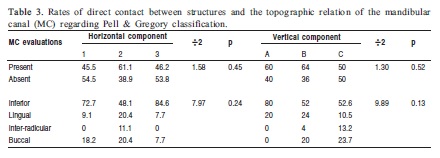
Tables 2 and 3 present associations between Winter and PG Classifications and the mandibular canal (visualized on CBCT images). It was observed that molars mesial impacted are consistently linked with lingual position of the canal. Moreover, despite most PG categories were closely associated with inferior position of the canal, the lingual position was more observed with A, B and 2 components.
Table 3 explores the association between PG classification and the mandibular canal (visualized on CBCT images). Although no statistically significant data can be drawn, the observation of frequencies reveals that lingual position is more linked to type A and B. Besides, when the horizontal component is evaluated, it can be reported that the lingual position of the mandibular canal is more linked to type 2.
Discussion
Several factors might be associated with higher risk of injury to the IAN and increased difficulty during impacted third molar removal, and those can be divided in clinical and radiographic. Within clinical factors, gender and body mass index appear to be consistently correlated16. Radiographic factors include panoramic signals like interruption of the radiopaque line of the canal wall, radiolucent band over roots, deflection of the canal around the apices and narrowing of the roots6-12, and positioning according to PG and Winter classifications13.
Previous studies observed relationship between radiographic signals indicating proximity of structures and the mandibular canal: radiolucent band over roots and interruption of the radiopaque line of the canal wall were stronger associated with direct contact between the tooth roots and the mandibular canal17-19. The present study showed a statistically significant relation among three types of radiographic finding –interruption of the radiopaque line of the canal wall, narrowing of roots and radiolucent band over roots - and the presence of contact with the mandibular canal. Furthermore, some studies have evaluated the association between the lingual positioning of the mandibular canal and its relation to accidental exposure of the neurovascular bundle7,14. The results from this study detected that the lingual positioning of the canal is closely associated with radiolucent band over roots.
This study has also aimed as well to evaluate PG and Winter classifications and the topographic relationship of the mandibular canal as seen in CBCT images. Analysis of data relative to Winter classification indicates that mesial positioning is associated with lingual positioning of the mandibular canal. Regarding PG components, although no statistically significant associations could be established, Table 3 reveals a higher frequency with direct contact between mandibular canal and positioning of mandibular canal in the lingual aspect for categories A, B and 2. Almendro-Marqués et al.13 have warned for a higher probability of complications correlated with categories B2 and C2. Therefore, whenever in face to mesially positioned impacted molars, it is advisable for clinicians to also look for the coexistence of signals associated with a higher probability of lingual positioning of the IAN (such as radiolucent band over roots), since the association of this topographic relation and exposure of the neurovascular bundle has been observed7,14.
Some authors have stated that panoramic radiographs cannot be considered an ideal tool in terms of prediction of accidents related to IAN20, and the requesting of CBCT is supported in the presence of radiographic signals associated with proximity of structures7,17,21-23. However, facing that panoramic radiograph is the most frequently used image for the diagnosis and treatment recommendations for third molar surgery5, the information available with this technique is essential for dimensioning the need for further investigation. Furthermore, CBCT should be use consciously among professionals, especially because of the radiation dose received by patients. Even if the radiation dose from CBCT is significantly less than the conventional CT, it is several to many times higher than panoramic imaging24, and, therefore, their use has to be fully justify over conventional techniques before they are carried out25-26.
The present study evaluated the signals and classifications usually used to determine the injury risk to the IAN by impacted lower third molars surgery using different diagnostic images methods. The results showed a tendency of critical positions and closeness between mandibular canal and third molars at the panoramic radiography based on its topographic position as seemed in CBCT images. Hence, the knowledge about the relationship between radiographic signals and the PG and Winter classifications might improve the panoramic radiographic diagnosis, contributing to the clinical decision as well as to the teaching and learning process; moreover, the lower radiation dose received will benefit the patient.
Regarding radiographic signals indicating proximity between impacted lower third molars and mandibular canal in panoramic radiographs, radiolucent band over roots is the image more closely associated with direct contact between structures and the one that indicates lingual positioning of the canal more consistently. Some categories of PG and Winter classifications suggested signs of the topographic location of the mandibular canal encouraging further assessments exploring these aspects.
References
1. Cade TA. Paresthesia of the inferior alveolar nerve following the extraction of the mandibular third molars: a literature review of its causes, treatment, and prognosis. Mil Med. 1992; 157: 389-92. [ Links ]
2. Miloro M, DaBell J. Radiographic proximity of the mandibular third molar to the inferior alveolar canal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100: 545-9. [ Links ]
3. Savi A, Manfredi M, Pizzi S, Vescovi P, Ferrari S. Inferior alveolar nerve injury related to surgery for an erupted third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103: e7-9. [ Links ]
4. Klinge B, Petersson A, Maly P. Location of the mandibular canal: comparison of macroscopic findings, conventional radiography, and computed tomography. Int J Oral Maxillofac Implants. 1989; 4: 327-32. [ Links ]
5. Marciani RD. Third molar removal: an overview of indications, imaging, evaluation, and assessment of risk. Oral Maxillofac Surg Clin North Am. 2007; 19: 1-13. [ Links ]
6. Monaco G, Montevecchi M, Bonetti GA, Gatto MR, Checchi L. Reliability of panoramic radiography in evaluating the topographic relationship between the mandibular canal and impacted third molars. J Am Dent Assoc. 2004; 135: 312-8. [ Links ]
7. Tantanapornkul W, Okouchi K, Fujiwara Y, Yamashiro M, Maruoka Y, Ohbayashi N et al. A comparative study of cone-beam computed tomography and conventional panoramic radiography in assessing the topographic relationship between the mandibular canal and impacted third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103: 253-9. [ Links ]
8. Blaeser BF, August MA, Donoff RB, Kaban LB, Dodson TB. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J Oral Maxillofac Surg. 2003; 61: 417-21. [ Links ]
9. Rood JP, Shehab BA. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg. 1990; 28: 20-5. [ Links ]
10. Sedaghatfar M, August MA, Dodson TB. Panoramic radiographic findings as predictors of inferior alveolar nerve exposure following third molar extraction. J Oral Maxillofac Surg. 2005; 63: 3-7. [ Links ]
11. de Melo Albert DG, Gomes AC, do Egito Vasconcelos BC, de Oliveira e Silva ED, Holanda GZ. Comparison of orthopantomographs and conventional tomography images for assessing the relationship between impacted lower third molars and the mandibular canal. J Oral Maxillofac Surg. 2006; 64: 1030-7. [ Links ]
12. Gallesio C, Berrone M, Ruga E, Boffano P. Surgical extraction of impacted inferior third molars at risk for inferior alveolar nerve injury. J Craniofac Surg. 2010; 21: 2003-7. [ Links ]
13. Almendros-Marques N, Berini-Aytes L, Gay-Escoda C. Influence of lower third molar position on the incidence of preoperative complications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102: 725-32. [ Links ]
14. Ghaeminia H, Meijer GJ, Soehardi A, Borstlap WA, Mulder J, Berge SJ. Position of the impacted third molar in relation to the mandibular canal. Diagnostic accuracy of cone beam computed tomography compared with panoramic radiography. Int J Oral Maxillofac Surg. 2009; 38: 964-71. [ Links ]
15. Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100: 395-7. [ Links ]
16. Gbotolorun OM, Arotiba GT, Ladeinde AL. Assessment of factors associated with surgical difficulty in impacted mandibular third molar extraction. J Oral Maxillofac Surg. 2007; 65: 1977-83. [ Links ]
17. Sampaio NF, de Camargo ST, Maria de Almeida S, Haiter-Neto F, Queiroz FD, Norberto BF. Correlation of panoramic radiography and cone beam computed tomography findings in the assessment of the relationship between impacted mandibular third molars and the mandibular canal. Dentomaxillofac Radiol. 2012; 41: 553-7. [ Links ]
18. Nakamori K, Fujiwara K, Miyazaki A, Tomihara K, Tsuji M, Nakai M et al. Clinical assessment of the relationship between the third molar and the inferior alveolar canal using panoramic images and computed tomography. J Oral Maxillofac Surg. 2008; 66: 2308-13. [ Links ]
19. Nakagawa Y, Ishii H, Nomura Y, Watanabe NY, Hoshiba D, Kobayashi K et al. Third molar position: reliability of panoramic radiography. J Oral Maxillofac Surg. 2007; 65: 1303-8. [ Links ]
20. Gomes AC, Vasconcelos BC, Silva ED, Caldas Ade Jr F, Pita Neto IC. Sensitivity and specificity of pantomography to predict inferior alveolar nerve damage during extraction of impacted lower third molars. J Oral Maxillofac Surg. 2008; 66: 256-9. [ Links ]
21. Flygare L, Ohman A. Preoperative imaging procedures for lower wisdom teeth removal. Clin Oral Investig. 2008; 12: 291-302. [ Links ]
22. Neugebauer J, Shirani R, Mischkowski RA, Ritter L, Scheer M, Keeve E et al. Comparison of cone-beam volumetric imaging and combined plain radiographs for localization of the mandibular canal before removal of impacted lower third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105: 633-43. [ Links ]
23. Susarla SM, Dodson TB. Preoperative computed tomography imaging in the management of impacted mandibular third molars. J Oral Maxillofac Surg. 2007; 65: 83-8. [ Links ]
24. Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol. 2006; 35: 219-26. [ Links ]
25. Roberts JA, Drage NA, Davies J, Thomas DW. Effective dose from cone beam CT examinations in dentistry. Br J Radiol. 2009; 82: 35-40. [ Links ]
26. Scarfe WC. "All that glitters is not gold": standards for cone-beam computerized tomographic imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 111: 402-8. [ Links ]
 Correspondence:
Correspondence:
Mariana Boessio Vizzotto,
Department of Surgery and Orthopedics –
Ground Floor, Faculty of Dentistry
Rua Ramiro Barcelos, 2492 – CEP: 90035-003 -
Porto Alegre, RS - Brasil
E-mail: mari_vizzotto@yahoo.com.br
Received for publication: May 21, 2012
Accepted: September 18, 2012
