










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.4 Piracicaba Out./Dez. 2012
ORIGINAL ARTICLE
Clinical status of permanent first molars in children aged seven to ten years in a Brazilian rural community
Lara Jansiski MottaI; Joyce Garcia dos SantosII; Thays Almeida AlfayaIII; Carolina Cardoso GuedesIV; Camila Haddad Leal de GodoyV; Sandra Kalil BussadoriVI
IPhD, Professor of Pediatric Dentistry, Department of Rehabilitation Sciences Graduation Program, Nove de Julho University (UNINOVE), São Paulo, SP, Brazil
IIDDS, Private Practice, Department of Rehabilitation Sciences Post Graduation Program, Nove de Julho University (UNINOVE), São Paulo, SP, Brazil
IIIDDS, Student of Dental Clinic Graduation Program, Fluminense Federal University (UFF), Niterói, RJ, Brazil
IVMS, Professor of Pediatric Dentistry, Braz Cubas University, São Paulo, SP, Brazil
VDDS, Student of Rehabilitation Sciences Graduation Program, Nove de Julho University (UNINOVE), São Paulo, SP, Brazil
VIPhD, Professor of Rehabilitation Sciences Post Graduation Program, Nove de Julho University (UNINOVE) , São Paulo, SP, Brazil
ABSTRACT
AIM: To evaluate the clinical status of permanent first molars and associations with dental caries, gingival bleeding, dental fluorosis and malocclusion.
METHODS: An observational study was carried out in a rural community denominated Morro do Saboó in the city of São Roque, state of São Paulo, Brazil. A total of 194 children aged seven to ten years were examined for dental caries using the index proposed by the World Health Organization. Other conditions were determined using the Gingival Alterations Index, Dean's Index and Dental Aesthetic Index. The chi-squared test was used for the statistical analysis of the data.
RESULTS: A total of 85.5% of the sample exhibited gingival bleeding and 69.9% exhibited malocclusion. A total of 53.6% had a clinical aspect of normality with regard to dental fluorosis. There was a predominance of sound teeth in the upper arch and teeth with carious lesions in the lower arch. No significant differences were found between sexes regarding gingival bleeding, dental fluorosis or malocclusion. Significant associations were found between tooth status and oral alterations (gingival bleeding, malocclusion and fluorosis) in teeth 16, 26 and 46 and between tooth status and gingival bleeding in tooth 36 (p<0.001).
CONCLUSIONS: Caries activity in the permanent first molars was mainly associated with dental fluorosis and malocclusion. Strategies aimed at health promotion should be adopted on a large scale to minimize the prevalence of oral diseases.
Keywords: dental caries, molar, fluorosis, dental, gingivitis, malocclusion.
Introduction
Oral health status is mainly analyzed by the occurrence of dental caries and periodontal disease. Dental caries is estimated to affect 60 to 90% of children in industrialized countries and constitutes the most prevalent oral condition in Asia and Latin America1. The establishment of the "Brazil Smiling Program" in 2003 led to the expansion of public dental services in Brazil. This greater access to oral health care (including prevention actions and specialized treatment) hascontributed to an increase in the number of children who are free of caries (44%)2.
Permanent first molars play a fundamental role in the maintenance of the masticatory function. The development of carious lesions is common during the eruption of the first molars due characteristics that are favorable to the buildup of bacterial plaque3, such as pits and fissures4. In the absence of preventive measures, these teeth may experience all the repercussions stemming from the development of caries5-6.
Gingivitis is the most common form of periodontal disease in children and adolescents1 and is related to the presence of gingival bleeding. The early onset of aggressive periodontal disease affects approximately 2% of young patients and can lead to tooth loss1. The increase in the prevalence of gingivitis from childhood to puberty may be attributed to the number of sites at risk, with the buildup of bacterial plaque and inflammatory changes related to the process of exfoliation and eruption as well as hormonal factors related to age7.
While dental caries and periodontal disease are the most common oral manifestations1, other factors should also be taken into consideration in the analysis of oral health status. Dental fluorosis is a formation disorder in which the developing enamel is hypomineralized due to a change in the secretion of ameloblasts caused by an excess of fluoride ions8. Malocclusion is a growth and development disorder that affects the occlusion (bite) of the teeth9 and can have a considerable impact on affected individuals, causing discomfort as well as functional and social limitations10. These conditions can have both functional and esthetic repercussions, with an impact on quality of life11-12, and should therefore be identified so that proper intervention steps can be taken.
The aim of the present study was to evaluate the clinical status of permanent first molars and associations with dental caries, gingival bleeding, dental fluorosis and malocclusion.
Material and methods
An observational study was carried out involving the analysis of permanent first molars with regard to the presence of dental caries and other oral problems, such as gingival bleeding, dental fluorosis and malocclusion, in 194 children aged seven to ten years at a school located in a rural community denominated Morro do Saboó in the city of São Roque, state of São Paulo, Brazil, during a collective action. The study received approval from the Human Research Ethics Committee of the Universidade Federal de São Paulo, Brazil, under project number 1374/07. Parents/guardians of the participants signed a statement of informed consent allowing their children to participate in the study.
The evaluations were performed by a single, calibrated operator, using a mouth mirror and periodontal probe under natural light with the child seated and the examiner standing. The findings of the exam were recorded on an individual clinical chart for each child.
Assessment of dental caries
The assessment of dental caries was performed on the permanent first molars (teeth 16, 26, 36 and 46). The following codes and criteria were used for the classification of the teeth: (0) sound; (1) with carious lesion; (2) restoration with carious lesion; (3) restoration without carious lesion; (4) loss due to caries; (5) loss for other reasons (6); presence of occlusal sealant; (7) bridge support or crown; (8) non-erupted; (9) excluded tooth (applied to any tooth that could not be examined); (T) trauma/fracture. This assessment was based on the criteria proposed by the World Health Organization13 and employed in Brazilian Oral Health surveys14.
Assessment of gingival bleeding
Gingival bleeding was determined with the use of a periodontal probe, which was lightly inserted in the entrance of the gingival sulcus and run along its length – Gingival Alterations Index15.
Assessment of Dental fluorosis
Dental fluorosis was determined based on Dean's index and coded as follows: (0) normal; (1) questionable; (2) very mild; (3) mild; (4) moderate; and (5) severe13.
Assessment of malocclusion
Malocclusion was determined based on the abnormal positioning of the teeth using the index proposed by Cons et al. (1989) denominated the Dental Aesthetic Index (DAI)16. The following criteria were used for the classification of normal occlusion: class I relationship of permanent first molars; canines in normal relationship (upper canine in the space between the lower canine and lower first premolar or primary first molar); absence of anterior or posterior crossbite; vertical overjet not surpassing 3 mm; horizontal overjet not surpassing 2 mm; presence or absence of inter-incisor diastema and primate spaces; absence of crowding; absence of tooth anomalies in shape and number; and absence of tooth rotation.
Statistical analysis
Data analysis was performed using the SPSS 17 program (IBM Corp., Chicago, IL, USA). For such, the chi-squared test was employed, with the level of significance set to 5% (p < 0.05).
Results
The sample was made up of 194 children aged seven to ten years; 51.03% (n = 99) of the children were female. Table 1 displays the distribution of the children with regard to gingival bleeding, malocclusion and fluorosis according to sex. No significant difference between sexes was found regarding these oral conditions. A total of 84.5% of the participants (n = 164) exhibited gingival bleeding and 69.9% exhibited malocclusion (n = 135). With regard to fluorosis, 53.6% (n = 104) had a clinical aspect of normality, 32% (n = 62) were classified with questionable fluorosis, 10.3% (n = 20) were classified with questionable very mild fluorosis and 4.1% (n = 8) were classified with questionable mild fluorosis.
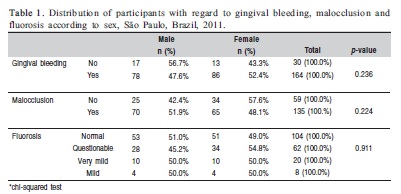
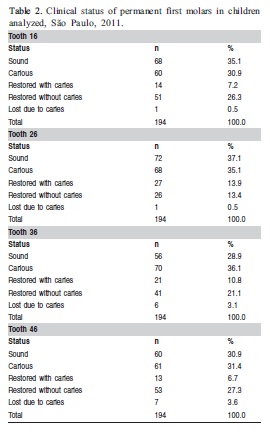
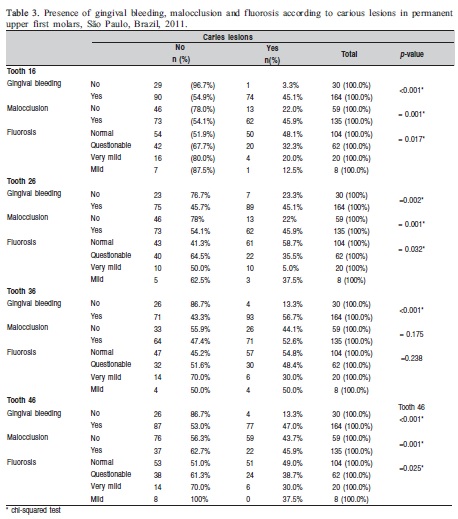
Table 2 displays the results of the classification of dental caries status of the permanent first molars. There was a predominance of sound teeth in the upper arch and teeth with carious lesions in the lower arch. Tooth loss was recorded in both the upper and lower arches. Significant associations were found between caries activity and oral alterations (gingival bleeding, malocclusion and fluorosis) in teeth 16, 26 and 46 and between caries activity and gingival bleeding in tooth 36 (Table 3) (p < 0.001).
Discussion
The present results demonstrate no statistically significant associations between sex and gingival bleeding, malocclusion or fluorosis. However, tooth status was associated with all these conditions in teeth 16, 26 and 46 and with gingival bleeding in tooth 36. There was a predominance of sound teeth in the upper arch and carious teeth in the lower arch.
Data from the National Brazilian Oral Health survey demonstrate an increase in the number of children who are free of caries2. However, variables related to social context remain predictors of caries, which underscores the need for integrated health actions, as occurs with other childhood diseases17. The present study revealed a large number of carious lesions in the sample analyzed, which may be attributed to the rural region in which the school is located, which has no access to public health care or fluoridated water.
A previous study involving children and adults in a rural community in the state of Minas Gerais, Brazil states that deficient oral health is to be expected in this population given the fact that preventive and curative care hinges on access to dental treatment18. Another study carried out in a different region of the same state reports a greater prevalence of dental caries and lesser access to dental services as well as evidence of greater social deprivation among rural schoolchildren in comparison to their urban counterparts19. The findings described in a study carried out by de Abreu et al. (2004) suggest that underprivileged populations as well as families with a slightly higher income and greater schooling are more prone to adopt behavior that leads to dental caries20. However, a study conducted abroad states that children who participate in preventive oral health programs made available at school have less caries experience21.
The molars play a fundamental role in the maintenance of the stomatognathic system16. The first molars are the first permanent teeth to erupt and, due to their anatomy, which includes pits and fissures, these teeth have increased odds of developing carious lesions4. In the present study, the lower molars had a greater frequency of caries, whereas the upper molars were, for the most part, sound. The permanent molars are the teeth most affected by caries22. While the location of the tooth (lower or upper) has no influence on the risk to dental caries, a number of factors may be related to the development of this disease in general, such as dietary habits23, caries experience in the deciduous tooth24 and parents/guardians' schooling25.
Tooth loss was found in the sample in both the upper and lower arches. According to Gonzalez and Manrrique (2001), the loss of permanent first molars can lead to a reduction in local function, the continuous eruption of the antagonist teeth and tooth deviations26. Considering the consequences of the absence of such teeth to the stomatognathic system, oral health promotion programs and campaigns aimed at the prevention of oral health problems should be established for the population as a whole and schoolchildren in particular. When performed early, interventions tend to minimize the impact of treatment and costs27.
No significant association was found between dental fluorosis and sex. However, the prevalence of fluorosis was relatively low, which may have been due the fact that the participants lived in a rural environment, where some communities without access to a fluoridated water supply make use of artesian wells, mines, rivers, ponds, etc. Fluorosis has been related to a reduction in caries28-29. However, a significant association was found between these conditionsin three of the four teeth evaluated in the present study. Changes in diet have been suggested as an explanation for the increase in the prevalence of caries in groups that also have contact with fluoride ions30. Therefore, a greater frequency of visits to the dentist and supervision with regard to sugar intake and brushing should be warrant21.
A statistically significant association was found between gingival bleeding and caries activity. A previous study reports that the prevalence of gum disease is high among individuals aged seven to 14 years and is directly related to deficient oral hygiene31. In a systematic review of studies addressing periodontal disease, Gjermo et al. (2000) report that gingivitis is the most common periodontal condition among children and adolescents, especially among males and individuals belonging to lower socioeconomic strata32. The findings of the present study are in agreement with these statements, except with regard to sex, for which no significant association was found.
The prevalence of malocclusion in the present study was high, likely due to the absence of public promotion measures regarding this aspect of oral health. According to Dimberg et al. (2011), the early treatment of malocclusion may be unnecessary if spontaneous correction occurs during the transition from the primary to the mixed dentition33. However, the present study involved the mixed dentition and the findings demonstrate treatment needs in this subgroup of the population. Thus, basic epidemiological surveys are fundamental to the assessment of the current situation regarding malocclusion and the drafting of treatment plans for groups at risk.
Prevention programs should be directed at the population in both rural and urban environments. The findings of a longitudinal study demonstrate that children without caries in the primary dentition tend to remain caries free during the mixed dentition phase34. Strategies aimed at health promotion should be adopted on a large scale to minimize the prevalence of oral diseases. Moreover, for cases in which such conditions have already developed, early detection and treatment can ensure a future generation of healthy adults from the dental standpoint.
References
1. WHO. World Health Organization. What is the burden of oral disease? [Cited 2012 Mar 7Available from: http://www.who.int/oral_health/disease_burden/global/en/. [ Links ]
2. Brasil. Ministério da Saúde. Brasil Sorridente: A saúde bucal levada a sério. [Cited 2012 Mar 28] Available from: http: //dab.saude.gov.br/cnsb/sbbrasil/arquivos/apresentacao_abbrasil_2010.pdf. [ Links ]
3. Carvalho JC, Ekstrand KR, Thylstrup A. Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J Dent Res. 1989; 68: 773-9. [ Links ]
4. Pine CM, Pitts NB, Nugent ZJ. British Association for the Study of Community Dentistry (BASCD) guidance on sampling for surveys of child dental health. A BASCD coordinated dental epidemiology programme quality standard. Community Dent Health. 1997; 14(Suppl 1): 10-7. [ Links ]
5. Feldens CA, Kramer PF, Abreu ME, Rosso ED, Ferreira SH, Feldens EG. Association between caries experience in deciduos molars and first molar permanents. Pesq Bras Odontoped Clin Integ. 2005; 5: 157-63. [ Links ]
6. Quaglio JM, Sousa MB, Ardenghi TM, Mendes FM, Imparato JC, Pinheiro SL. Association between clinical parameters and the presence of active caries lesions in first permanent molars. Braz Oral Res. 2006; 20: 358-63. [ Links ]
7. Jenkins WM, Papapanou PN. Epidemiology of periodontal disease in children and adolescents. Periodontol 2000. 2001; 26: 16-32. [ Links ]
8. Fejerskov O, Manji F, Baelum V. The nature and mechanisms of dental fluorosis in man. J Dent Res. 1990; 69(Spec N.): 692-700; discussion 21. [ Links ]
9. de Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004; 31: 20-7; discussion 15. [ Links ]
10. Anosike AN, Sanu OO, da Costa OO. Malocclusion and its impact on quality of life of school children in Nigeria. West Afr J Med. 2010; 29: 417-24. [ Links ]
11. Chankanka O, Levy SM, Warren JJ, Chalmers JM. A literature review of aesthetic perceptions of dental fluorosis and relationships with psychosocial aspects/oral health-related quality of life. Community Dent Oral Epidemiol. 2010; 38: 97-109. [ Links ]
12. Marques LS, Ramos-Jorge ML, Paiva SM, Pordeus IA. Malocclusion: esthetic impact and quality of life among Brazilian schoolchildren. Am J Orthod Dentofacial Orthop. 2006; 129: 424-7. [ Links ]
13. WHO. World Health Organization. Oral health surveys: basic methods. 4 ed. Geneva: ORH/EPID; 1997. [ Links ]
14. Brasil. SB Pesquisa nacional de saúde bucal. Projeto técnico. Secretaria Políticas de Saúde, Departamento de Atenção Básica, Área Técnica de Saúde Bucal. – Brasília: Ministério da Saúde; 2010.
15. Brasil. Projeto SB 2000: condições de saúde bucal da população brasileira no ano 2000: manual do examinador / Secretaria Políticas de Saúde, Departamento de Atenção Básica, Área Técnica de Saúde Bucal. – Brasília: Ministério da Saúde; 2001.
16. Cons NC, Jenny J, Kohout FJ, Songpaisan Y, Jotikastira D. Utility of the dental aesthetic index in industrialized and developing countries. J Public Health Dent. 1989; 49: 163-6. [ Links ]
17. Melo MM, Souza WV, Lima ML, Braga C. Factors associated with dental caries in preschoolers in Recife, Pernambuco State, Brazil. Cad Saude Publica. 2011; 27: 471-85. [ Links ]
18. Pallos D, Loberto JCS, Cortelli JR, Cortelli SC, Souza DM, Ricardo LH. Periodontal disease in a rural community in Minas Gerais, Brazil. Braz J Oral Sci. 2005; 4: 659-63. [ Links ]
19. Mello TR, Antunes JL. Prevalence of dental caries in schoolchildren in the rural area of Itapetininga, Sao Paulo State, Brazil. Cad Saude Publica. 2004; 20: 829-35. [ Links ]
20. de Abreu MH, Pordeus IA, Modena CM. Dental caries in schoolchildren from rural communities in Itauna (MG), Brazil. Rev Panam Salud Publica. 2004; 16: 334-44. [ Links ]
21. Amalia R, Schaub RM, Widyanti N, Stewart R, Groothoff JW. The role of school-based dental programme on dental caries experience in Yogyakarta Province, Indonesia. Int J Paediatr Dent. 2012; 22:203-10. [ Links ]
22. Marthaler TM. Changes in Dental Caries 1953–2003. Caries Res. 2004; 38: 173-81.
23. Ohlund I, Holgerson PL, Backman B, Lind T, Hernell O, Johansson I. Diet intake and caries prevalence in four-year-old children living in a lowprevalence country. Caries Res. 2007; 41: 26-33. [ Links ]
24. Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J Dent Res. 2002; 81: 561-6. [ Links ]
25. Ismail AI, Sohn W. The impact of universal access to dental care on disparities in caries experience in children. J Am Dent Assoc. 2001; 132: 295-303. [ Links ]
26. Gonzalez J, Manrrique R. Proyecto Anaco-U.C.V. estudio epidemiológico sobre la pérdida prematura del primer molar permanente en niños con edades comprendidas entre 6 y 10 años. Acta odontol venez. 2001; 39: 42-6. [ Links ]
27. Singh M, Saini A, Saimbi CS, Bajpai AK. Prevalence of dental diseases in 5- to 14-year-old school children in rural areas of the Barabanki district, Uttar Pradesh, India. Indian J Dent Res. 2011; 22: 396-9. [ Links ]
28. Mascarenhas AK. Risk factors for dental fluorosis: a review of the recent literature. Pediatr Dent. 2000; 22: 269-77. [ Links ]
29. McDonagh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, et al. Systematic review of water fluoridation. BMJ. 2000; 321: 855-9. [ Links ]
30. Sampaio FC, Hossain AN, von der Fehr FR, Arneberg P. Dental caries and sugar intake of children from rural areas with different water fluoride levels in Paraiba, Brazil. Community Dent Oral Epidemiol. 2000; 28: 307-13. [ Links ]
31. Chambrone L, Macedo SB, Ramalho FC, Trevizani Filho E, Chambrone LA. [Prevalence and severity of gingivitis among scholars (7-14 years): local conditions associated to bleeding on probing]. Cien Saude Colet. 2010; 15: 337-43. [ Links ]
32. Gjermo P, Rösing CK, Susin C. Periodontal diseases in Central and South America. Periodontol. 2000; 29: 70-8. [ Links ]
33. Dimberg L, Lennartsson B, Soderfeldt B, Bondemark L. Malocclusions in children at 3 and 7 years of age: a longitudinal study. Eur J Orthod. 2011; Oct 31. [Epub ahead of print] [ Links ].
34. Greenwell AL, Johnsen D, DiSantis TA, Gerstenmaier J, Limbert N. Longitudinal evaluation of caries patterns form the primary to the mixed dentition. Pediatr Dent. 1990; 12: 278-82. [ Links ]
 Correspondence:
Correspondence:
Thays Almeida Alfaya
Rua Doutor Calandrine 235 A, CEP: 24755-160,
São Gonçalo, RJ, Brasil
E-mail: thalfaya@gmail.com
Received for publication: August 05, 2012
Accepted: December 11, 2012
