










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.4 Piracicaba Out./Dez. 2012
ORIGINAL ARTICLE
Mapping of proximal enamel thickness in permanent teeth
Flávio Vellini-FerreiraI; Flávio Augusto Cotrim-FerreiraII; José Alaor RibeiroIII; Cívea Inês Ferreira-SantosII
IDDS, MSc, PhD, Professor and Chairman, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), São Paulo, SP, Brazil
IIDDS, MSc, PhD, Associate Professor, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), São Paulo, SP, Brazil
IIIDDS, MSc in Orthodontics, Department of Pediatric Dentistry and Orthodontics, University of São Paulo City (UNICID), São Paulo, SP, Brazil
ABSTRACT
AIM: Knowledge of enamel thickness is relevant to perform stripping during orthodontic treatment. Thus, proximal enamel measurements of human permanent teeth were compared in this study.
METHODS: The measurements were previously obtained on cut sections of mandibular central (n = 30) and lateral (n = 30) incisors, canines (n = 20), first (n = 40) and second (n = 40) premolars; maxillary central (n = 20) and lateral (n = 20) incisors, canines (n = 20), first (n = 40) and second (n = 42) premolars. Comparisons between thicknesses by arch side and proximal surface were carried out using Student's t-tests (α = 0.05). Teeth were compared according to the mesial and distal thicknesses by ANOVA and Tukey's test.
RESULTS: No significant differences were found between right and left teeth. For the mesial surface, the mandibular second premolar presented the highest mean value (1.376 mm ± 0.198; p<0.001). The mandibular central incisor had the smallest thickness in relation to the other teeth (0.675 mm ± 0.144), although not significant compared with the mandibular lateral incisor and canine (0.734-0.781 mm). The mandibular second premolar also presented the higher distal thickness in relation to the others (1.450 mm± 0.172), although not significant compared with the maxillary first premolar (1.322 mm ± 0.195). Mandibular incisors had the lowest means for distal thickness (0.872-0.879 mm), although not statistically different compared with maxillary incisors and mandibular canine (1.002-1.015 mm). Distal thickness was greater than mesial (p<0.001).
CONCLUSIONS: Interproximal stripping should be less marked in incisors and mesial surfaces.
Keywords: dental enamel, dentition, permanent, orthodontics, corrective.
Introduction
Several treatment options for mild to moderate tooth crowding are available in Orthodontics and, after diagnosis and clinical planning, one suitable alternative is the indication of interproximal stripping in permanent teeth1-9. Stripping has long been indicated in cases of tooth-size discrepancy to avoid extractions, reshape tooth morphology and create contact surfaces, which would improve posttreatment stability4,6-7,10. Some authors even advocate enamel removal and dentin exposure in selected patients7. However, it is generally recommended that only half of the proximal enamel layer should be removed, yet without registration of quantitative data related to enamel thickness11-13.
In spite of the well-documented applicability of interproximal stripping1-18, professionals who are willing to practice this option should be aware of the enamel thickness estimates for the most frequently eligible teeth. There are many studieswith distinct methodological approaches and for determined teeth3,5,8-9,19-21. An experimental study in 1973 succeeded in mapping the enamel and dentin thicknesses of different tooth groups by microscopy19. However, since then, there is lack of complete studies on this subject. Thus, the aim of the present study was to comparatively assess proximal enamel thicknesses of human incisors, canines and premolars.
Material and methods
Before the beginning of the study, the research protocol was approved by an Ethical Institutional Review Board under the protocol #13525722, in compliance with the Helsinki Declaration.
Data collection
Mapping of enamel thickness was based on analysis of primary data obtained from experimental studies conducted on sound human teeth from tooth banks8-9. The teeth previously analyzed were as follows: Mandibular right central incisor (n = 15), Mandibular left central incisor (n = 15), Mandibular right lateral incisor (n = 15), Mandibular left lateral incisor (n = 15), Mandibular right canine (n = 10), Mandibular left canine (n = 10), Mandibular right first premolar (n = 20), Mandibular left first premolar (n = 20), Mandibular right second premolar (n = 20), Mandibular left second premolar (n = 20), Maxillary right central incisor (n = 10), Maxillary left central incisor (n = 10), Maxillary right lateral incisor (n = 10), Maxillary left lateral incisor (n = 10), Maxillary right canine (n = 10), Maxillary left canine (n = 10), Maxillary right first premolar (n = 20), Maxillary left first premolar (n = 20), Maxillary right second premolar (n = 22) and Maxillary left second premolar (n = 20).
Previous experimental procedures
To estimate the proximal enamel thickness, the teeth were placed in plastic flasks using utility wax and then embedded in orthophthalic resin (ARAZYN 1.0; Redelease®, São Paulo, SP, Brazil). The specimens were removed from the flasks and two points were marked in the resin surface (one incisal/occlusal and another apical), which served as reference to trace the long axis of the block. Subsequently, the specimens were positioned in a low-speed saw Lab Cut 1010 (Extec® Corp., Enfield, NH, USA), so as the tooth long axis and contact surfaces coincided with the cutting plane of the diamond disc (Diamond Wafering - 12205 4" x 0.012 x 0.5; Extec® Corp.), with the incisal or occlusal aspect turned toward the operator8-9. With the aid of the micrometer in the saw, preestablished cuts were made for achievement of central sections with thickness ranging from 0.7 mm to 1 mm, of proximal contact aspects. The specimens were trimmed under water cooling to avoid fractures and loss of enamel components.
After obtaining the central section of the specimens, a trained operator performed the measurements of enamel thickness on the proximal surfaces using a perfilometer Profile Projector® PJ 300 (Mitutoyo®, Kawasaki, Japan) with thousandth precision. Tooth sections were manipulated to allow standardization of measurements by alignment of Cartesian axes (X and Y) of the perfilometer with the tooth long axis. The Y axis was mesially displaced up to the most external enamel point, determining the "point A". The perfilometer's caliper was then zeroed and parallelly displaced up to the most external dentin point, achieving the "point B". In this way, the mesial enamel thickness was read and expressed in thousandths of millimeters. For achieving of measurements on the distal aspect, the Y axis was displaced to the most external dentin point, achieving the "point C". Then, it was parallelly displaced to the most external enamel point on the distal surface, named "point D", estimating the enamel thickness on this surface.
Statistical analyses
Means and standard deviations of proximal enamel thickness measured on the perfilometer were calculated. Data on the enamel thicknesses on proximal surfaces of right and left teeth were compared by the unpaired student's t-test. The mesial and distal thickness measurements were compared by analysis of variance (ANOVA) considering the tooth, side of dental arch and proximal surface as main factors and the double interactions between them. Since significant interaction was observed between tooth and thickness (p = 0.030), mesial and distal measurements were compared for each type of tooth by the paired Student's t-test. Subsequently, the enamel thickness on mesial and distal surfaces of human incisors, canines and premolars were compared by the ANOVA and Tukey's test. The analyses were performed at a significance level of 5%, using the statistical software MINITAB® 14 (Minitab Inc., State College, PA, USA).
Results
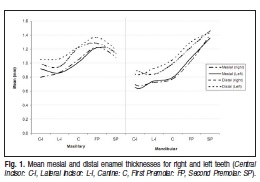
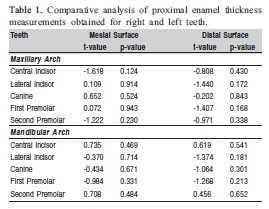
Mean enamel thicknesses on mesial and distal surfaces of right and left teeth are shown in Figure 1. Data of right and left teeth presented similar distribution. No statistically significant differences were found between right and left teeth (Table 1). Therefore, the analyses progressed considering the mean enamel thicknesses of right and left teeth, for both mesial and distal surfaces.
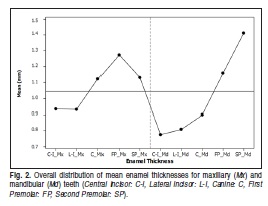
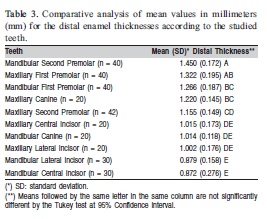
Figure 2 presents the mapping of proximal enamelthickness regardless of the mesial or distal surface. There was an increasing order for enamel thicknesses on the mesial and distal surfaces (Tables 2 and 3).
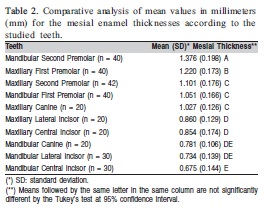
For the mesial surface, the mandibular second premolar presented the greatest mean thickness compared with all other teeth (p<0.05). Conversely, the mandibular central incisor exhibited the smaller thickness in relation to the other teeth. However, there were no statistically significant differences between the mean mesial thickness of the mandibular central incisor, lateral incisor and canine (Table 2). The mandibular second premolar also exhibited greater mean distal enamel thickness. Nevertheless, no significant difference was found in comparison to the maxillary first premolar (Table 3). The mandibular incisors presented the smallest means of distal enamel thickness, yet not statistically different from the maxillary incisors and mandibular canine (Table 3).
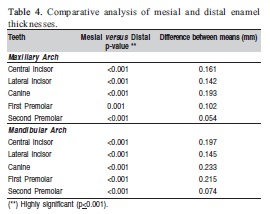
The average mesial enamel thickness was significantly smaller than distal (Table 4). For most teeth, the difference between distal and mesial thicknesses was nearly 0.1 mm, with the smaller difference between means for the maxillary and mandibular second premolars. However, for the mandibular canine and first premolar the difference is up to 0.2 mm (Table 4).
Discussion
A space gain of at least 7 mm in the dental arch may be expected by interproximal stripping1,14,16. Even though the extent of stripping is related to the severity of tooth-size discrepancy10-12, planning of this procedure should consider that each tooth has different enamel thicknesses on the proximal surfaces5,8,12,19. The results of the present study corroborate the variation in proximal enamel thickness of different human teeth. It should be emphasized that tooth banks do not provide information on the age range, gender or race of donors. However, the validity of outcomes may be demonstrated by the absence of statistically significant differences between mean enamel thicknesses for right and left teeth (Table 1), thus evidencing the symmetry of characteristics analyzed. Similarly, this kind of symmetry was observed in a clinical study that recorded radiographic measurements of enamel thickness of mandibular incisors3.
The enamel thickness is not significantly different between males and females, even though male teeth are largerdue to the dentin layer21-23. Based on computer-assisted measurements of proximal enamel thickness of central and lateral incisors, obtained on periapical radiographs of 80 patients, no gender dimorphism was observed3. Some authors24-25 have been concerned about the racial influence on tooth dimensions. A study revealed that mandibular central and lateral incisors are not significantly different between Caucasoid and African individuals. However, the other teeth were greater in Africans compared with Caucasians, both for males and females25. The admixture is a marked trait in the Brazilian population, which impairs the identification of possible effects of factors related to race on the odontogenesis5.
Considering the data in Tables 2 and 3, as well as the schematic presentation in Figure 2, the mandibular second premolar had the greatest average proximal enamel thicknesses (mesial: 1.376 mm ± 0.198, distal: 1.450 mm ± 0.172). However, the smallest mean values of proximal enamel thickness were observed for the mandibular incisors. According to the results of this histological study, there were no significant differences between the mean enamel thicknesses of mandibular incisors, for both mesial and distal surfaces. Nevertheless, a radiographic study reported that the mandibular lateral incisors had significantly thicker enamel in both proximal surfaces compared with the mandibular central incisors3. Presumably, this difference may be attributed to the employment of distinct measuring methods.
It is recommended that the amount of enamel to be removed during interproximal stripping should vary from 0.4-0.5 mm per proximal surface17. The findings of this study, based on measurements obtained using a highly accurate instrument (0.001 mm), suggest that orthodontists should be careful when interpreting that kind of clinical advice. Even though the mandibular incisors present the highest frequency of crowding, they also had the smallest values of proximal enamel thickness (Tables 2 and 3, Figure 2). Therefore, removal of 0.5 mm from the mesial surface of a mandibular central incisor may be excessive in some cases. It would be advisable to follow the guidelines for stripping and though limit the interproximal reduction to 50% of the enamel thickness5,11-14.
Taking into to account the means shown in Tables 2 and 3, it was possible to suggest a chart with reference numbers that might be used as parameters for professionals during enamel stripping on mesial and distal surfaces. Chart 1 presents the sum of mesial and distal thicknesses for maxillary and mandibular anterior and posterior teeth (in this case, only premolars). These data may yield an indirect reference of the amount of enamel to be removed and hence the maximum achievable space. However, the values in Chart 1 should be interpreted with some caution, as they represent only numerical data and should not be used without analyzing the malocclusion, the patient, and each tooth individually. For instance, in a pre-selected patient with Class I malocclusion, showing mild anterior crowding in the mandibular arch and having harmonious profile, the orthodontist could easily obtain a 4.0-mm-wide space by removing half the mesial and distal enamel of the anterior teeth.

The enamel layer was significantly thicker on the distal surfaces of all teeth (Table 4). This is in agreement with two radiographic studies on the enamel thickness of mandibular3 and maxillary21 incisors. The present findings also agree with another Brazilian study that registered the dimensions of maxillary first premolars by computer-assisted analysis of histological sections5. In radiographic studies, the authors observed that enamel was significantly thicker on the distal surfaces of mandibular and maxillary central and lateral incisors, with a mean difference of 0.1 mm3,21. The differences between means shown in Table 4 are in agreement with previous studies3,21. Therefore, it may be suggested that stripping should be less marked on mesial surfaces and in some teeth, such as the mandibular incisors.
Interproximal stripping has not been related to an increase in the incidence of proximal caries lesions or periodontal disease2,7,13,15,18. However, not all teeth are eligible for interproximal stripping. Mandibular incisors with parallel proximal surfaces should not be submitted to this procedure7. To avoid any damage to the adjacent tissues, orthodontists should estimate the amount of enamel removal in accurate radiographs, since the proximal enamel thickness may vary between and within individuals3. The use of fan-beam20 and cone-beam8 computed tomography has also been suggested for assessing proximal enamel thickness, whenever these imaging modalities are needed. Moreover, after interproximal stripping, it is useful to insert accurate thickness devicesbetween teeth to record the magnitude of spaces and enamel reduction5,8,15.
The described mapping indicated that mandibular second premolars presented the greatest mean mesial thickness. Mandibular central incisors had the smallest thickness in relation to the other teeth, though without significant differences compared with the mandibular lateral incisors and canines. Mandibular second premolars also showed the greater distal thickness, albeit without statistically significant difference from maxillary first premolars. Mandibular incisors had the smallest average distal thickness, but without significant differences compared with the maxillary incisors and mandibular canines. Distal enamel was significantly thicker than mesial.
References
1. Stroud JL, English J, Buschang PH. Enamel thickness of the posterior dentition: its implications for nonextraction treatment. Angle Orthod. 1998; 68: 141-6. [ Links ]
2. Zachrisson BU, Nyoygaard L, Mobarak K. Dental health assessed more than 10 years after interproximal enamel reduction of mandibular anterior teeth. Am J Orthod Dentofacial Orthop. 2007; 131: 162-9. [ Links ]
3. Hall NE, Lindauer SJ, Tüfekçi E, Shroff B. Predictors of variation in mandibular incisor enamel thickness. J Am Dent Assoc. 2007; 138: 809-15. [ Links ]
4. Germeç D, Taner TU. Effects of extraction and nonextraction therapy with air-rotor stripping on facial esthetics in postadolescent borderline patients. Am J Orthod Dentofacial Orthop. 2008; 133: 539-49. [ Links ]
5. Macha AC, Vellini-Ferreira F, Scavone-Junior H, Ferreira RI. Mesiodistal width and proximal enamel thickness of maxillary first bicuspids. Braz Oral Res. 2010; 24: 58-63. [ Links ]
6. Germec-Cakan D, Taner TU, Akan S. Arch-width and perimeter changes in patients with borderline Class I malocclusion treated with extractions or without extractions with air-rotor stripping. Am J Orthod Dentofacial Orthop. 2010; 137: 734.e1-7. [ Links ]
7. Zachrisson BU, Minster L, Ogaard B, Birkhed D. Dental health assessed after interproximal enamel reduction: caries risk in posterior teeth. Am J Orthod Dentofacial Orthop. 2011; 139: 90-8. [ Links ]
8. Fernandes SA, Vellini-Ferreira F, Scavone-Junior H, Ferreira RI. Crown dimensions and proximal enamel thickness of mandibular second bicuspids. Braz Oral Res. 2011; 25: 324-30. [ Links ]
9. Munhoz LO, Vellini-Ferreira F, Cotrim-Ferreira FA, Ferreira RI. Evaluation of proximal enamel thickness and crown measurements in maxillary first premolars. Braz J Oral Sci. 2012; 11: 30-5. [ Links ]
10. Peck H, Peck S. An index for assessing tooth shape deviations as applied to the mandibular incisors. Am J Orthod. 1972; 61: 384-401. [ Links ]
11. Tuverson DL. Anterior interocclusal relations. Parts I and II. Am J Orthod. 1980; 78: 361-93. [ Links ]
12. Demange C, François B. Measuring and charting interproximal enamel removal. J Clin Orthod. 1990; 24: 408-12. [ Links ]
13. Jarjoura K, Gagnon G, Nieberg L. Caries risk after interproximal enamel reduction. Am J Orthod Dentofacial Orthop. 2006; 130: 26-30. [ Links ]
14. Sheridan JJ. Air rotor stripping. J Clin Orthod. 1985; 19: 43-59. [ Links ]
15. Crain G, Sheridan JJ. Susceptibility to caries and periodontal disease after posterior air-rotor stripping. J Clin Orthod. 1990; 24: 84-5. [ Links ]
16. Rossouw PE, Tortorella A. Enamel reduction procedures in orthodontic treatment. J Can Dent Assoc. 2003; 69: 378-83. [ Links ]
17. Chudasama D, Sheridan JJ. Guidelines for contemporary air-rotor stripping. J Clin Orthod. 2007; 41: 315-20. [ Links ]
18. Grippaudo C, Cancellieri D, Grecolini ME, Deli R. Comparison between different interdental stripping methods and evaluation of abrasive strips: SEM analysis. Prog Orthod. 2010; 11: 127-37. [ Links ]
19. Shillingburg HT Jr, Grace CS. Thickness of enamel and dentin. J South Calif Dent Assoc. 1973; 41: 33-52. [ Links ]
20. Spoor CF, Zonneveld FW, Macho GA. Linear measurements of cortical bone and dental enamel by computed tomography: applications and problems. Am J Phys Anthropol. 1993; 91: 469-84. [ Links ]
21. Harris AF, Hicks JD. A radiographic assessment of enamel thickness in human maxillary incisors. Arch Oral Biol. 1998; 43: 825-31. [ Links ]
22. Alvesalo L, Tammisalo E, Townsend G. Upper central incisor and canine tooth crown size in 47,XXY males. J Dent Res. 1991; 70: 1057-60. [ Links ]
23. Stroud JL, Buschang PH, Goaz PW. Sexual dimorphism in mesiodistal dentin and enamel thickness. Dentomaxillofac Radiol. 1994; 23: 169-71. [ Links ]
24. Bishara SE, Jakobsen JR, Abdallah EM, Fernandez Garcia A. Comparisons of mesiodistal and buccolingual crown dimensions of the permanent teeth in three populations from Egypt, Mexico, and the United States. Am J Orthod Dentofacial Orthop. 1989; 96: 416-22. [ Links ]
25. Merz ML, Isaacson RJ, Germane N, Rubenstein LK. Tooth diameters and arch perimeters in a black and a white population. Am J Orthod Dentofacial Orthop. 1991; 100: 53-8. [ Links ]
 Correspondence:
Correspondence:
Rívea Inês Ferreira-Santos
Universidade Cidade de São Paulo (UNICID)
Pós-Graduação (Mestrado em Ortodontia)
Rua Cesário Galeno, 448 – Bloco A,
CEP: 03071-000, Tatuapé, São Paulo, SP, Brasil
E-mail: riveaines@yahoo.com
Received for publication: October 11, 2012
Accepted: December 11, 2012
