










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.11 no.4 Piracicaba Out./Dez. 2012
ORIGINAL ARTICLE
Factors involved in dentistry absenteeism since the foundation of the Labor Court from 1986 to 2008
Elaine Justino SantosI; Dagmar de Paula QueluzII
IDDS, Graduate student, Piracicaba Dental School, UNICAMP - University of Campinas, Piracicaba, SP, Brazil
IIDDS, MSPH, PhD, Professor, Department of Community Dentistry, Piracicaba Dental School, UNICAMP - University of Campinas, Piracicaba, SP, Brazil
ABSTRACT
AIM: To identify the most important factors involved in dentistry absenteeism since the foundation of the Labor Court in Campinas, SP, Brazil, until December 2008; to verify if there was a decrease in dentistry absenteeism after the introduction of the dental service in the headquarters of the Court; to verify if dentistry absenteeism is greater in the others cities of the region compared with the city of Campinas.
METHODS: The information was collected from the dental statements of the archives of the Health Department of the Labor Court. Collected information included: International Classification of Diseases (ICD-10), gender, age, function, origin of the statements, period of the absenteeism and year when the absence occurred.
RESULTS: 3,084 health files from server group (2,741) and judges (343) were reviewed. The results indicated: higher prevalence of female gender, higher frequency in the age group from 30 to 40 years old and the smallest frequency in the age group upper from 60 years old. It was found an average sick-leave period of 1.93 days. According to the International Classification of Diseases (ICD)-10, the most prevalent dental problems found in this study were: K01 (25.78%), K04 (10.57%) and K05 (6.37%).
CONCLUSIONS: The results of this study pointed to lower rates of absenteeism than the results found in the literature. The introduction of the dental service did not have influence on the rates of absenteeism of the area; however it influenced the absenteeism rates in the city of Campinas (headquarters of the Court).
Keywords: dental absenteeism, worker health, occupational health.
Introduction
The Occupational Health is a technical area of Public Health that seeks to intervene in the relationship between the production system and health, to promote work that dignifies instead of denigrating the man. Its mission is to assist in structuring a society that promotes health through workspaces.
Regarding the consequences of working conditions for the oral structures, it is known that, given the location and functions of the worker, they are vulnerable to the action of toxic agents in the environment and can lead to alterations. Thus, the field of oral health worker, whose principles are close to the worker's health, focuses on the relationship between oral health and work, trying to promote, preserve and restore the oral health of populations included in the various work processes, thus contributing to their quality of life1,2. Inside of health worker, health promotion in companies is an aspect that has been great emphasis in recent years3.
The dental care (curative procedures mostly) has brought considerable benefits to the employee, but there is still the need of surveillance activities of the risks present in the workplace and on occupational diseases with oral manifestations. The public and private sectors have sought to provide dental care to workers in order to reduce absenteeism on grounds through dental procedures is mainly curative services on their own or through agreements contracted to provide this service. Although the rate of absenteeism for dental reasons is not as relevant4in relation to absenteeism for medical reasons, the most worrying fact is that presenteeism exists for dental reasons, it is difficult to measure and can cause accidents related causes dental and decrease in profitability of companies.
Presenteeism is an even worse organizational problem because the worker is physically present at work, but he/she is not producing due to multiple variables and factors such as: dissatisfaction, pessimism, discouragement and high stress level, making it harder to identify the problem, and causing harm to the industry and to other workers who are often contaminated by this apathy and lack of productivity.
Various epidemiological studies have demonstrated that the prevalence of absenteeism resulting from dental reasons varies from 10 to 35%, and the average number of lost working hours varies from 1.24 to 6.20 working hours/workers/years5-11. Ferreira4 (1995) reported that tooth decay and other oral complications are responsible for 20% of the service and lack of production by the fall, and generate other types of organic complications such as generalized infections. Recently, evidence has been found linking periodontal disease in pregnant women and the birth of babies with low birth weight and the relationship between diabetes mellitus and periodontal disease has been extensively studied. This is because microorganisms enter the bloodstream can cause serious health problems. Therefore, a proper care of oral hygiene can reduce the risk of atherosclerosis, a major cause of heart disease and other complications as mentioned above.
Sickness absenteeism reflects workers' health status, besides being an economic and social problem is an increase in spending on social security12-13 through insurance paid to temporary incapacity caused by illness or accident at work. Besides, aspects directly related to health, diverse factors determine work absences, such as the organizational culture, lack of employee appreciation strategies, burnout and stress, unfavorable psychosocial environment, dissatisfaction with work, workers' socioeconomic status, lack of control over work and low social support at work12,14-17.
Employee absence takes a heavy toll on worker productivity2,18-25. Research in the United States charged that change in sleep patterns and mood affects productivity at work, which may lead to an increase in chronic diseases and absenteeism26. Getting to a single cause for the absenteeism is problematic because there is a complexity of causes, which is evident in the literature, is that the organization in the workplace can lead to the stressor as a major cause of high rates of absenteeism. The prevalence of mental disorders peaks during working age, which makes them a major cause of sickness absence27-30. Employed people with mental disorders lost three times more work days in a 12-month period compared with people without mental disorders28.
The study of dental absenteeism in Brazil is difficult, as there is not sufficient documentary material, nor statistical data representative at the municipal, state and federal able to draw a profile of lost days at work and its impact on both economic and degree of satisfaction worker31. Programs addressing the oral health of workers should be stimulated and developed based on epidemiologic knowledge, in order to promote disease reduction and improve quality of life among workers.
The objective of the present study was to identify the most important factors involved in dentistry absenteeism since the foundation of the Labor Court in Campinas, SP, Brazil until December 2008; to verify if there was a decrease in dentistry absenteeism after the introduction the dentistry service in the headquarters of the Court; to verify if at the others cities of the region area the dentistry absenteeism has larger frequency than in Campinas city.
Material and methods
Study Area
The study was conducted in Labor Court. With the internalization of development initiated in 1960s, and resurfaced in the 1970s with special relevance to the state of São Paulo, there was an increase in labor actions and the need to break the hitherto single Labor Court with jurisdiction over the entire state São Paulo. Thus, on July 14, 1986 His Excellency President José Sarney signed into law creating the Regional Labor Court of the 15th Region with headquarters in Campinas32.
When it was installed on December 5, 1986, there were only 38 joint conciliations and trial under the jurisdiction of this Court, in 2008 the 15th region reaches 599 counties, making up 95% of the territory of the state, covering a population of approximately 20 million people, one of the largest among the 24 regions in which is divided the Labor Court of the country. 153 Labor Courts are installed.
With 22 years of existence, the Regional Labor Court of the 15th Region holds the rank of 2nd largest regional labor nationwide procedural motion in 2008. Officials of the Labor Court, as well as all federal employees, were named servers from the Law No. 8112 of 11 December 199033 establishing the Legal Regime of Public Civil Union of Municipalities and Public Foundations Feds. The filling of positions is done by public tender with statutory employment scheme. The staff in 2008 consists of 343 judges and 2741 servers (analysts and technical college).
The dental service was created in 1991 with the goal to offer a comprehensive health care to the server because the medical and psychological existed. In 2008 the health department includes medical, dental, psychological, physiotherapy and social work in 15th Region. The dental care provided by quality always excelled, but within an assistencialist philosophy. Preventive care has always been practiced individually, not with collective measures. In 2008,the dental service had six dentists (five clinicians and one endodontist) and five dental auxiliary. Procedures performed include prevention, dentistry, periodontics, endodontics, prosthodontics, surgery, laser therapy, among others.
Study Design
This study is a cross-sectional, descriptive and quantitative, addressing absenteeism and prevalence of factors of absenteeism in the Regional Labor Court of the 15th Region between December 1986 and December 2008, including servers group (analysts and technical college) and judges.
Data Collection
The study population consisted of all dental certificates, duly approved the medical records of servers and judges, issued from December 1986 through December 2008 (22 years). Medical records are filed with the Health Department of the Regional Labor Court of the 15th Region located in Campinas - SP. There was no identification of individuals in the medical records. Only servers and judges active frame participated in this study.
The collection date used following the variables:
* With respect to the worker: function, gender, age
* With regard to absenteeism:
- Origin of certificate: own or accompaniment
- Duration of absenteeism (lost days)
- Causes of absenteeism (ICD-10)
- Date (month, year) of absenteeism
- Type of certificate: external or internal
- City of origin certificate
Data on sick leaves were collected from medical records of servers and judges filed with the secretary of health. These data were recorded in Excel spreadsheets and incorporated into sociodemographic information obtained with frame personnel, to perform the statistical analyzes.
*With regard to International Classification of Diseases – 10th Revision ( ICD-10)
The causes of absenteeism were grouped by ICD-10 (International Classification of Diseases), and we used the Chapter XI of the ICD-1034-35 that groups all diseases of the digestive system (K00-K93), and the groups' K00-K14 "concerning diseases of the oral cavity, salivary glands and jaws. These groups were the responsibility of the dentist used in this study. The ICD was established by WHO for the health professionals could communicate without describing the treatment given, not breaking thus the secrecy. Some institutions and companies do not accept dental and medical certificates without the ICD, but it was not the case for the period covered by this study, so all certificates were included regardless of whether or not described the ICD.
The cells of the spreadsheet for the ICD that were left blank means that the dentist who issued the statement did not specify the reason of absence (ICD), yet they were included in the study due to its high prevalence and because they were approved without this information.
Data Analysis
Data were statistically analyzed by descriptive analysis (frequency, percentage) and estimate (Chi-square, Fisher's Exact Test). The analyses were performed using SAS software version 9.1, using a significance level of 5% (p<0.05).
We adopted the concept of medical cause of absenteeism from the International Labor Organization36, i.e., "the period of absence from work which is accepted as attributable to an inability of the individual, except for that derived from normal pregnancy or prison." It is understood by the absence labor uninterrupted period of absence from work, told from the very beginning, regardless of its duration. We used the recommendations of the Subcommittee on Absenteeism of the International Society for Occupational Health, addressing the indices of frequency, severity, and percentage rate of absenteeism, average length of absences, as indicators of absenteeism, represented by the formulas36:
- Frequency index = Σ Total number of cases / Number of employees
- Severity index = Σ Total lost days / number of workers
- Percentage rate of absenteeism = Σ Total lost days x 100 / Total days worked x number of workers
- Average length of absences = Σ Total lost days / Total number of cases
All variables were compared by checking the existence of association. Two tests were used to check for association between variables: the test X2 (Chi-Square) and Fisher's exact test.
Trend lines are used to graphically display trends in data and analyze problems of prediction. This analysis is also called regression analysis. Using regression analysis, you can extend a trend line in a Figure beyond the actual data to predict future values. In our study we used three Figures with trend lines; percentage rate of absenteeism, the number of certificates and the number of servers and judges, all of these variables in relation to time. The closer to 1 the result of equation (R²), the greater the reliability index of the trend line.
Ethical Considerations
This research was approved by the Ethics Committee of the Dental School of Piracicaba, UNICAMP, under Approval Protocol number 019/2009.
Results
The server group (n= 2741) and judge (n=343) studied were homogeneous regarding sociodemographic characteristics. The education level is above the high school, because that is the minimum required for technicians' judiciary. Analysts and judges have completed university level. The socioeconomic factors provide ease of access to health services both medical and dental and reflect on good oral health status of this population. In December 2008, the staff was 2741 servers (1618 females and 1123 males) and 343 judges (195 males and 148 females), totaling 3084 staff.
From December 1986 until December 2008, 1381certificates were approved in dental medical records of servers and judges (n = 3084), totaling 2676 days of work lost due to dental reasons in 22 years. A random sampling of 1072 certificates verified that the technicians had higher judiciary certificates number, 79.38% (n = 851) than analysts, 20.62% (n = 221). Some of these servers and judges are since the foundation; others have been incorporated throughout this period of 22 years.
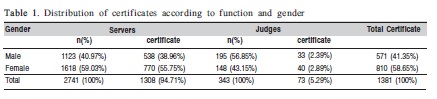
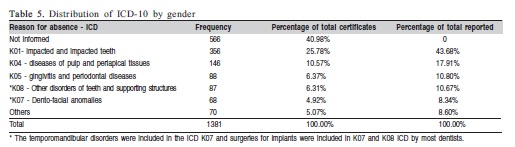
According to Table 1, from 1381 dental certificates analyzed, 58.65% belong to females (n = 810) and 41.35% were from males (n = 571). Of all the servers, 59.03% (n = 1618) represents females and 40.97% (n = 1123) males. Among the judges the proportion is reversed, 43.15% (n = 148) were from females and 56.85% (n = 195) were from males. Regarding the function performed, 94.71% (n = 1308) of dental certificates belonged to servers and 5.29% (n = 73) judges (Table 1). Considering a random sample of 1072 certificates of servers showed that 20.61% (n = 221) were analysts and 79.38% (n = 851) were technicians.
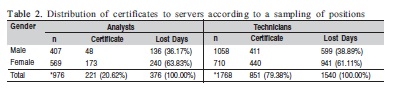
According to Table 2, 851 of the certificates presented by the sample positions, 20.62% (n = 221) was from analysts, with 48 belonging to males and 173 females. Female gender was also responsible for 240 days of sick leave (n = 63.83%), i.e. the majority. For technicians (79.38% of certificate), females accounted for most certificates (n = 440) and also with most days of absence (n = 941).
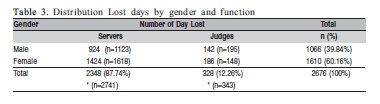
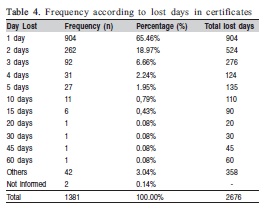
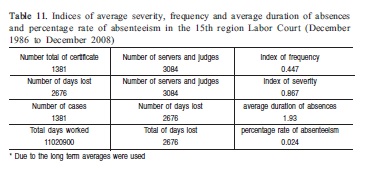
As much as 2676 days were lost for dental reasons along 22 years (Table 3) in the studied population (n = 3084). With regard to the days of absence, most frequently found (65.46%, n = 904) refers to one day of absence followed by two days (18.97%, n = 262) and three days (6, 66%, n = 92) (Table 4). The average number of days apart by certificate is 1.93 day, being six certificates (Table 11), clearance was more than 20 days. Regarding the frequency according to lost days in certificates, we found replenished with spacing of 60 days (n = 1), 45 days (n = 1) and 30 days (n = 1) (Table 4). These extended absences refer to periods of recovery after major surgery. So 95.28% of the leaves are up to 5 days and only 4.72% are clearances over 5 days (Table 4).
Researching the reasons that led dental absences, using the ICD-10 found that 566 (40.98%) did not report the cause of separation (Table 5).
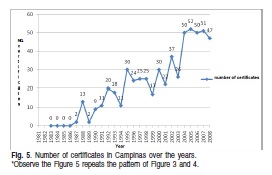
As for the annual frequency of dental certificates, we found that from 1987 to 1999 it ranged from 0.29% (1987) to 2.81% (1999), peaking in 1997 at the rate of 4.10% . From the year 2000, the rate increased significantly, always above 6.43% to 9.54% of total certificates (Figure 1).
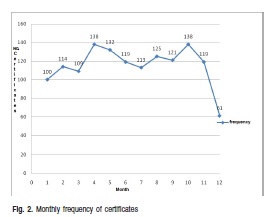
As for the monthly frequency of the number of statements there were no significant differences, except the lowest frequency in December (4.43% of total) (Figure 2). April and October were the months when there are more dental certificates (Figure 2).
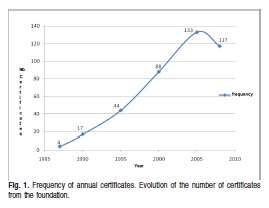
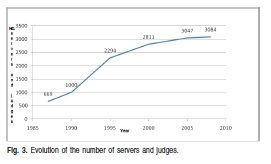
Looking at the Figures 1 and 3, we find that as you increase the number of servers and judges there is a proportional increase in the number of certificates. Since 2005, there has been a considerable increase in the number of servers and thereby the number of certificates even decreased.
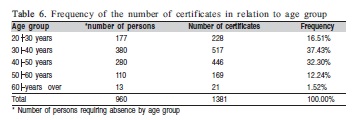
The age groups that had higher frequencies of the number of certificates were 30 to 40 years (37.43%) and 40-50 years (32.30%) (Table 6). For all the people who requested the absence in relation to the number of certificates, there was repetition of statements for the same user. Proportionally, ages 40-50 years, 50-60 years and above 60 years had a greater number of certificates than other age groups (respectively an average of 1.59; 1.47 and 1.61 per user certificates).
Regarding the type of certificate (internal - issued by the Court's dentists; or external – issue by other dentists) it was found that 77.84% of the total (n = 1075) were external and 22.16% (n = 306) internal.
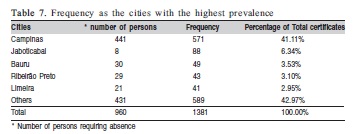
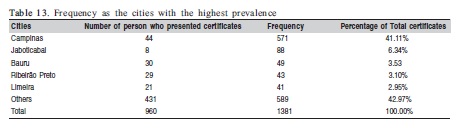
Among the cities inserted by the 15th region, Campinas was the one with the highest frequency (41.11%), then came Jaboticabal (6.34%), Bauru (3.53%), Ribeirão Preto (3.10 %) and Limeira (2.95%) (Table 7).
Analyzing the certificates themselves or own escort, we note that the total of 1381 certificates, 98.78% were dental treatments certificate to the server itself or judge and 1.23% for accompaniment (Table 8).
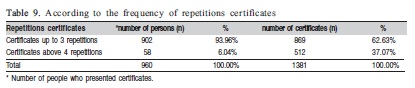
It was identified that 58 judges or servers moved away from work for dental reasons above 4 occasionsin 22 years producing various events, so there repetitions that resulted in 512 certificates. Thus 6.04% (n = 58) showed 37.07% (n = 512) of all certificates (Table 9).
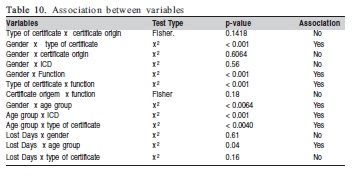
The results from the association between variables wereperformed using SAS version 9.1, using a significance level of 5% (Table 10). Regardless of the type of certificate (external or internal) with certificate origin (own or accompaniment) there was no statistical association. Regarding variables function, age and gender was significantly associated with the type of certificate. The
following variables showed statistically significant association between gender: type certificate, age and function. Regarding the certificate origin and lost days, no statistically significant association was found. The variables that showed statistical association with the function performed were: gender and type of certificate. There was no statistical association in relation to the certificate origin. The variable age showed statistical association between gender, lost days and the type of certificate.
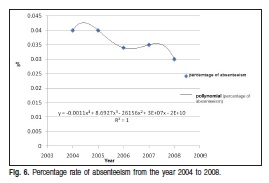
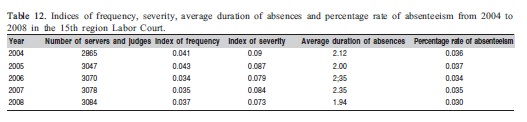
The absenteeism indicators are shown in Table 11. It was calculated the percentage rate of absenteeism for the period 2004 to 2008 to verify the behavior of these latest indicators. The percentage rate of absenteeism for the period 2004 to 2008 remained between 0.030 to 0.037, with some variations (Table 12).
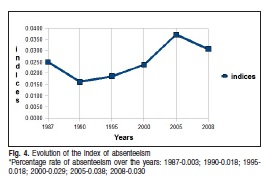
It was observed the evolution of absenteeism during the 22 years of the 15th region. We begin with the year 1987 and ended in 2008 with 5-year intervals for the calculation of these indices years (Figure 4). One can see that the index has increased from the year 1990 reaching its peak in 2005 and decreasing after this year but has remained at values below the averages found in the literature. As seen in Figures 3 and 4 there were peaks in 1995 and 2005 due to high input servers and judges over the years which also happened regarding Campinas (Figure 5).
Bases in Table 13, the large number of certificates in Campinas was probably due to the considerable number of servers and judges who have their homes in this city (n = 1260). Observe that only 5 cities accounted for 57.03% (n = 792) of all certificates. The other cities had 42.97% (n = 589) of all certificates.
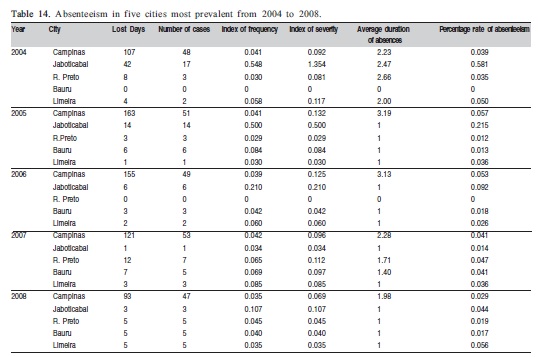
Based on the management of personal data for the period 2004 to 2008, we calculated the dental absenteeism for this period (Table 14). According to Table 14, the 5 cities showed similar rates, but Jaboticabal although presenting the smaller number of servers and judges in all years (2004 to 2008) exhibited indices frequency, severity and rate of absenteeism far above other cities in virtually every year.
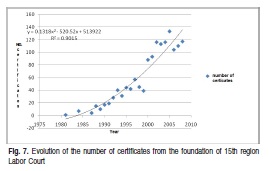
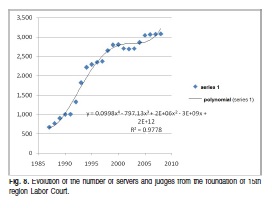
In Figure 6 shows that the percentage rate of absenteeism is stable and expressed a declining trend. In Figure 7 shows that the number of certificates continues to grow and this growth trend to continue in the future. Figure 8 shows that the number of servers and judges continues to grow and the trend is that it remains so.
Discussion
The profile and the factors associated with dentistry absenteeism in Labor Court since its foundation represent the socio-economic factors provide ease of access to health services both medical and dental and reflect on good oral health status of this population, suggesting that this is a relevant factor for the low rates of absenteeism dental found.
Frequency according to gender
Considering the absolute numbers there is a higher prevalence of certificates for females (agreeing with Mazzilli37, 2003 and Martins38, 2005) while the results are proportionally equivalent for both genders. Among the judges, where males predominated, most certificates also belonged to females (Table 1). Diacov and Lima39 (1988) studied absenteeism due to dental problems in 701 employees of the municipal government of São José dos Campos, and Hito40 (2007) in his dissertation studying dental absenteeism in a meat packing company (probably because there was predominance among male employees) found a higher prevalence in males. This result is contrary to our study and the majority of the literature. Lima41 (1997) analyzed comparatively 1774 certified dental City Headquarters and the National Institute of Social Security Assistance Medical (INAMPS) São José dos Campos SP/BR and concluded that, for the range of 10 to 20 years old, was statistically significant the percentage rate of absenteeism in male; if compared with other age groups there were no significant differences, which agrees with our study because it includes age groups above 20 years. Martins38 (2005) researching dental absenteeism in public and private companies reported that there was a female predominance in both the public company and in private enterprise. Salvador and Tonha42 (2006), addressing absenteeism in Union Court also found that the annual rate of absence by gender and general causes was higher in females than males, in agreement with our results although we have only studied dental absenteeism. Calle43 (1971) after studying absenteeism and illness came to the conclusion that at 42349.5 lost days from work due to illness, 30000.5 (70.8%) occurred among female workers which agrees with our study in relation to gender in relation to disagree more often (58.59% in this study).
Frequency second days of absence (lost days)
The data suggest that technicians have turned away more than analysts during the period covered in this study, agreeing with Salvador and Tonha42 (2006) in their study in the Court of Audit (Table 2).
The award criteria and protocols used to approve the certificate seem to influence the incidence of absenteeism and its duration. Silva and Marziale44 (2000) found that the certificate dispensed medical expertise (1 and 2 days) accounted for 79% of certificates issued in the institution studied. In this study it was found that most leaves (up to 5days) did not require expertise. According to Decree 7003 of November 9, 200945 for departures up to 5 days are necessary medical expertise.
The average duration of absences found of 1.93 (Table 11) is compatible with the number found by Martins38 (2005) for a private company (1.93) and well below that found by him to the public company (3.82), and can be explained by some causes such as surgical that elevate the arithmetic mean due to the number of days required for recovery of the patient.
According to Salvador and Tonha42 (2006) all studies, even the most pessimistic, dealing with the cost-effectiveness of prevention of disease and promotion of health and safety at work, has shown a return of at least 20% on invested capital. However, he said, WHO emphasizes that in most optimistic studies for every R$ 1.00 invested, you can save up to R$ 16.00. In a study addressing the absenteeism causes covering all servers in the Court of Audit42 departures a day were the majority (36%) while the leaves above 5 days occurred in 20% of the total days away. Requests for absences were 80% up to 5 days. This study, though it includes only causes dental, agrees with these results: 95.28% of total absence are up to five days, 65.46% are license with 1 day of absence and only 4.72% are departures over 5 days (Table 4).
Frequency over function
Being larger number of servers in positions of technicians (n = 1768) than analysts (n = 973) agree with those obtained by Salvador and Tonha42(2006) in his study on absenteeism in the Court of Audit, ie, technicians deviate more than analysts. Considering the number of lost days, the servers moved away 2348 days (87.74%) and judges 328 (12.26%) (Table 3).
Frequency according to ICD
Saliba and Garbin46 (2000) found in their study that 64.4% of dentists indicated in the certificate the act performed, suggesting lack of confidentiality, or ICD, which was established to ensure that health professionals could communicate without describing the treatment performed, not breaking thus the secrecy. A study by Silva and Marziale44 (2000), with nursing staff of a university hospital revealed that 31% of the certificates did not contain diagnosis or International Classification of Diseases (ICD), alleging as a worker's right to not be exposed. Similar results with our study, we found that 40.98% (n = 566) of the certificates did not inform the ICD and not the procedure performed (Table 5).
Annual and monthly frequency of dental certificates
From the year 2000 the rate increased significantly the annual frequency of dental certificates, probably due to the entry of servers and judges within the Labor Court from that year (Figure 1).The monthly frequency of the number of statements there were no significant differences probably due to the withdrawal of the judiciary that happens from December 20 to January 6 that makes this month with less days worked for the other months of the year (Figure 2).
Frequency in relation to age
Martins38 (2005) found that the age group between 30 to 39 years was the most missed the public service and the range 20 to 29 accounted for the largest fault in private, in a comparative study between these services. Our results agree with those of Martins for public service (Table 6). Lima41 (1997) analyzed comparatively 1774 certified dental City Headquarters and the National Institute of Social Security Assistance Medical (INAMPS) São José dos Campos and concluded that, for the range of 10 to 20 years old, was statistically significant index male and absenteeism compared with other age groups there were no significant differences, the prevalence of absenteeism due to dental problems occurred in the group of workers bureaucratic functions in the ranges of 20 to 30 years, 40-50 years and over 50 years for workers not bureaucratic function.
Frequency according to the type of certificates
Regarding the type of certificate: internal (issued by the Labor Court of dentists) or external (for other dentists) found that: 77.84% of the total (n = 1075) were external and 22.16% (n = 306) internal. The large number of certificates can be justified by external procedures that are not offered by the dental service of the Court, and therefore must be conducted in private. The small number of internal certificates also justified because most appointments are made before, during or after work hours, in the offices of the Court and certificates are provided only when requested by the patient or his superior. Furthermore, servers and judges have the option of being cared for his private dentist of choice. These may be the reasons that explain the low number of statements internal in relation to external.
Reisine47 (1984) found in their research that preventive visits entail greater episode of work absenteeism (62.8%), though they result in fewer lost hours. The author also reported that the prevalence and magnitude of losses for productive reasons oro-dental suffer interaction of several factors, which have social determinants. She concluded that a preventive service can promote a favorable cost-benefit ratio, resulting in the reduction of indirect costs of lost work time and enabling the use of data recorded as adjuncts indicators for dental research. It also revealed that when the individual in the case of oral diseases, participates in a preventive treatment, it decreases their faults with respect to curative treatments, i.e., the preventive service causes less damage to the economy. According to the author, the preventive visits entail greater episode of absenteeism from work (62.8%), though they result in fewer lost hours.
According to Medeiros and Bijella48 (1970) the opportunity to care for a service installed in the workplace reduces losses to a minimum of hand labor because rejoins the worker as soon as possible in their activities. The dental service is expected to be possible with the medical clinic, in order to contribute exams, as well as serving up the same in cases of emergencies. Probably the low percentage of internal certificates was due to the ease of access to servers and judges to use the service according to their needs and schedule availability. Campinas is favored in this respect because it is the headquarters of dental care.
Frequency of 5 cities more prevalent as absence
The large number of certificates in Campinas was probably due to the considerable number of servers and judges who have their homes in this city (n = 1260). Observe that only 5 cities accounted for 57.03% (n = 792) of the total certificates. The other cities had 42.97% (n = 589) of all certificates (Table 7). Proportionally, it can be seen in Table 7 that Campinas despite having the highest frequency of dental certificates due to its large cadre of servers, certificates has averaged 1.30 per person while Jaboticabal, Limeira, Ribeirão Preto and Bauru respectively, 11.0, 1.95, 1.63 and 1.48 on average. These data suggest that the presence of dental care in the city of Campinas can influence the low rates of absenteeism presented by the city.
Frequency of certificate origin
Analyzing the certificates own or accompaniment, we note that the total of 1381 certificates, 98.78% were dental treatments certificate to the server itself or judge and 1.22% for accompaniment (Table 8). The data suggest that followup visits are usually done outside of working hours. It is noteworthy that the Court of dental service not only provides care to dependents servers and judges (Table 8).
Frequency as the repetitions
It was identified that 58 servers or judges moved away from work for dental reasons above 4 times in 22 years producing various events, so there repetitions that resulted in 512 certificates (Table 9). Mazzilli49 (2004) also found repetitions of individuals who had two or more times (n = 276; 23.55%) certificates and represented 44.96% of total cases. The majority (76.45%; n = 896) showed a single request absence work in 4 years.
Association between variables
Based on the associations of the variables (Table 10), it may be concluded that gender is an important variable, the female gender is predominant in most public and private enterprises and the social, emotional, physical, ergonomic and others involved with dental absenteeism should be analyzed by human resources considering the particularities of each gender to obtain the desired results.
Indicators of absenteeism
According to Flippo50 (1970), the percentage rate of absenteeism is considered normal around 3%. Already Forssman51 (1956) argues that the notion of "normalabsenteeism", applied to a group, a profession, or a country is debatable. The correct is that one should have the firm intention to reduce it to the fullest. Possibly for this reason we did not find any reference on the porch ideal for these indices. According to Couto52 (1987), it can be classified as absenteeism excessive values of frequency indices greater than 0.10 per month. Danatro53 (1997) found in a public institution of Montevideo, in Uruguay, in one year, compared with medical absenteeism, index of frequency of 1.08, index of severity of 6.84 and average duration of absences of 6.28 days.
The state government of São Paulo in 2007 has taken steps to combat the high rate of absenteeism of the State. The numbers are alarming, the number of days missed, the main indicator of the problem has been growing in recent years. Days were 5.09 million in 2003, rising to 5.4 million in 2004, 5.5 million in 2005 and reaching 6.3 million days in 2006, i.e. an increase of about 25% in three years. Only between 2005 and 2006 the increase was 15.44%. The total state is 9.81% of faults on the total number of days that should be worked out by the servers.
Bispo54 (2002) argues that according to some human resource consultants, an acceptable index of absenteeism stands at around 2.7%, but that few companies can reach levels well below this.
This study sought to draw a profile of dental absenteeism in the Regional Labor Court over 22 years of existence by analyzing the factors that affect these absences and calculation of indices recommended by the Subcommittee of the International Society for Occupational Health (index of frequency, index of severity, percentage rate of absenteeism and average duration of absences). Found absenteeism indicators are shown in Table 11.
The long period of this study made it difficult to obtain a mean absenteeism. For the calculation of these indices (frequency, severity and percentage rate of absenteeism) was used to calculate indices of 6 (1987, 1990, 1995, 2000, 2005 and 2008) and subsequently obtained the arithmetic average of these indices. This calculation method was selected for the index was not directed to very low values if the number of servers was that of December 2008.
We calculated the rates of absenteeism for the period 2004 to 2008 to verify the behavior of these latest indicators. The indices showed up, mostly lower than those found by Martins38 (2005), but we emphasize that medical and dental causes were researched while we studied only dental causes. The percentage rate of absenteeism for the period from 2004 to 2008 remained between 0.030 to 0.037 with some variations (Table 12).
According to Ferreira4 (1995), dental causes represent 20% of all leaves. Considering the absence of indicators of absenteeism specifically geared to the dental field, following a logical reasoning, we suggest that an acceptable percentage rate of absenteeism for dental 15th region Labor Court would be up to 0.5%. So the indices are found significantly below this level. Only the city of Jaboticabal had an absentee rate above 0.5%. We believe that this kind of simplistic reasoning, but of considerable practical application can be used for both the public sector as the private sector. When a company or institutions in the dental absence are above 20% of total absence, some measures related to the oral health of their workers should be deployed aiming to reduce this rate. So the formula used by the Subcommittee on Absenteeism International Society for Occupational Health can be used both to analyze the index at a given moment and for the projection of goals for the future of an acceptable index of dental absenteeism.
Absenteeism in Campinas
According to what has been observed in relation to the 15th region as a whole, considering only the city of Campinas, the same phenomenon is repeated: as it increases the number of servers and judges, increases the number of absence requests in the dental field. The dental care was deployed at the headquarters of Court in 1991. By the year 1987 the number of statements found in this study was very low (n = 12) even with a considerable number of employees ranged from 332 in 1981 to 669 in 1987. These data suggest that the time servers and judges had no certificates approved because the procedures probably did not follow the current formalities. Figure 5 suggests that what really influences dental absenteeism in the city of Campinas is the entry of new servers and judges and not other variables. The installation of offices in 1991 probably influences the maintenance of low rates of absenteeism in this city though she has the larger number of servers and judges from across the 15th region. Probably the Figures would be higher if there were no dental care, emergency care because they are performed in the dental service itself would have to be made out and it would involve a greater number of leaves. As seen in Figures 3 and 4 there were peaks in 1995 and 2005 due to high input servers and judges over the years which also happened regarding Campinas (Figure 5).
Absenteeism more prevalent in 5 cities
Among the cities encompassed by the 15th region, Campinas was the one with the highest frequency (41.11%) of the total certificates, then came Jaboticabal (6.34%), Bauru (3.53%), Ribeirão Preto (3.10%) and Limeira (2.95%). The large number of certificates in Campinas was probably due to the considerable number of servers and judges who have their homes in this city (n = 1260). Observe that only 5 cities accounted for 57.03% (n = 792) of all certificates. The other cities had 42.97% (n = 589) of all certificates (Table 13).
Returned by the management of personal data for the period from 2004 to 2008, and we calculate the dental absenteeism for this period. According to Table 14, the 5 cities showed similar rates but Jaboticabal although the smaller number of servers and judges in all years (2004 to 2008) got some indices frequency, severity and percentage rate of absenteeism far above other cities in virtually every year. Do not investigate the cause of these high rates.
The duration of absences, Campinas had the highest rates for the years 2005, 2006, 2007 and 2008. Only for theyear 2004 the city with the longest duration of absences was Ribeirão Preto.
For the frequency index, Jaboticabal showed higher rates for the years 2004, 2006 and 2008. In 2005, Bauru was the city that had the highest index and for the year 2007 was Ribeirão Preto.
As for the severity index, a city that had the highest rates for 2004, 2006 and 2008 was Jaboticabal, for 2005 was Bauru and 2007 was Ribeirão Preto.
Draws attention to the fact the city Jaboticabal stand out with high levels even with a relatively small number of servers and judges.
The city of Campinas showed the highest duration of absences, noting the spreadsheet data collection verified that the orthognathic surgery and implants reflect the increase in this index, as seen in Campinas in 2005 and 2006. Jaboticabal showed almost half (46%; n = 41) of total certificates along 22 years (n = 88).
We see that the percentage rate of absenteeism is stable and expressed a declining trend. Probably this is because the servers and judges make their dental visits during inverse to work (Figure 6). The number of certificates continues to grow and this growth trend to continue in the future (Figure 7). Although the number of certificates is increasing the rate of absenteeism shows fall because its calculation involves the lost days are few considering the number of servers and judges. The number of servers and judges continues to grow and the trend is that it remains so (Figure 8). These Figures are useful for the planning of strategic actions in an attempt to reduce rates when necessary and design goals for short, medium and long term.
One of the difficulties encountered in this study was the lack of national parameters as an index of absenteeism recommended as acceptable, especially when related to dentistry that is new in this field. Hopefully with this specialty of Dentistry Labor55 grow interest in the research and so that other researchers have increased availability and access to data.
For the study, it was concluded that:
* Absenteeism dental Regional Labor Court in the 15th region had absenteeism rates lower than those found in the dental literature and frequencies of variables similar to most reported studies. It was found that the entry of new servers and judges is one factor that reflects the frequency of dental certificates, the data suggest that sociodemographic characteristics of this population contributes to good levels of oral health and low rates of absenteeism.
* It was found that the installation of dental care did not affect the drop rates of absenteeism in the 15th region as a whole, probably due to the difficulty of access to the servers and judges domiciled in other cities.
* The dental installed in Campinas, probably due to the ease of access and availability of schedules offered, contributed significantly to the maintenance of low rates of absenteeism (even with the large number of servers and judges), below the rates of other cities with fewer servers (for example Jaboticabal). Some cities had zero indices (Bauru-2004 and Ribeirão Preto-2006); demonstrating low levels of absenteeism dental this federal institution.
References
1. Araújo ME, Marcucci G. Study of the prevalence of oral manifestations caused by chemical agents in the electroplating process: its importance to the area of oral health worker. Odont Soc. 2000; 2: 20-5. [ Links ]
2. Macedo CG, Queluz DP. Quality of life and self-perceived oral health among workers from a furniture industry. Braz J Oral Sci. 2011; 10: 226-32. [ Links ]
3. Brasil, 2012. Decree number 6856 of May 25, 2009. Legislation on frequency of health examinations. Available from: http://www2.camara.leg.br/legin/fed/decret/2009/decreto-6856-25-maio-2009-588402-norma-pe.html. [ Links ]
4. Ferreira R A. The value of oral health in companies. Rev Assoc Paul Cir Dent. 1995; 49: 96-107. [ Links ]
5. Midorikawa ET. Odontology in worker's health as a new professional specialty: definition of the activity field and functions of the surgeon dentist in worker's health team [doctor thesis]. São Paulo: Faculdade de Odontologia, Universidade de São Paulo; 2000. 337p. [ Links ]
6. Hollister MC, Weintraub JA. The association of oral status with systemic health, quality of life, and economic productivity. J Dent Educ. 1993; 57: 901-12. [ Links ]
7. Schou L. Oral health promotion at worksites. Int Dent J. 1989; 39: 122-8. [ Links ]
8. Locker D, Grushka M. The impact of dental and facial pain. J Dent Res. 1987; 66: 1414-7. [ Links ]
9. Locker D, Grushka M. Prevalence of oral and facial pain and discomfort: preliminary results of a mail survey. Community Dent Oral Epidemiol. 1987; 15: 169-72. [ Links ]
10. Hooper HA. Dental services in industry: observations on their effects in the reduction on absenteeism. Industrial Medicine. 1942; 11: 157-62. [ Links ]
11. Bailit H, Beazoglou T, Hoffman W. Work loss and dental disease. Report to the Robert Wood Johnson Foundation. University of Connecticut Health Center; 1982. [ Links ]
12. Hanebuth D, Meinel M, Fisher JEF. Health-related quality of life, psychosocial work conditions, and absenteeism in an industrial sample of blue- and whitecollar employees: a comparison of potential predictors. J Occup Environ Med. 2006; 48: 28-37. [ Links ]
13. Kivimäki M, Head J, Ferri.e. JE, Shipley MJ, Vahtera J,Marmo MG. Sickness absence as a global measure of health: evidence from mortality in the Whitehall II prospective cohort study. BMJ. 2003; 327: 364-8. [ Links ]
14. Davey MM, Cummings G, Newburn-Cook CV, LoEA. Predictors of nurse absenteeism in hospitals: a systematic review. J Nurs Manag. 2009; 17: 312-30. [ Links ]
15. Biron M, Bamberger P. Aversive workplace conditions and absenteeism: taking referent group norms and supervisor support into account. J Appl Psychol. 2012; 97: 901–12.
16. Griep RH, Rotenberg L, Chor D, Toivanen S,Landisbergis P. Beyond simple approaches to studying the association between work characteristics and absenteeism: combining DCS and ERI models. Work Stress. 2010; 24: 179-95. [ Links ]
17. Kristensen TR, Jensen SM, Kreiner S, Mikkelsen S. Socioeconomic status and duration and pattern of sickness absence: a 1-year follow-up study of 2331hospital employees. BMC Public Health. 2010; 10: 643. [ Links ]
18. Markham SE, McKee GH. Declining organizational size and increasing unemployment rates: Predicting employee absenteeism from within- and between-plant perspectives, Acad Manage J. 1991; 34, 952–65.
19. Pearce N. The ecological fallacy strikes back. J Epidemiol Community Health. 2000; 54: 326-7. [ Links ]
20. Probst TM. Safety and insecurity: Exploring the moderating effect of organizational safety climate. J Occup Health Psychol. 2004; 9, 3-10. [ Links ]
21. Queluz DP. Labour Dentistry: a new specialty in Dentistry. Braz J Oral Sci. 2005; 4: 766-72. [ Links ]
22. Nardi A, Michel-Crosato E, Biazevic MGH, Crosato E, Pizzatto E, Queluz DP. Relationship between orofacial pain and absenteeism among workers in Southern Brazil. Braz J Oral Sci. 2009; 8: 50-4. [ Links ]
23. Macedo CG, Queluz DP. Medical and dental absenteeism in workers from a furniture industry in Itatiba, SP, Brazil. Braz J Oral Sci. 2010; 9: 443-8. [ Links ]
24. Tausig M, Fenwick R. Work and mental health in a social context. New York, NY: Springer; 2011. [ Links ]
25. Shoss MK, Penney LM. The Economy and Absenteeism: A Macro-Level Study. J Appl Psychol. 2012; 97(4): 881-9. [ Links ]
26. Anderson RA. Psychoneuroimmunoendocrinoligy. [Cited 2012 Jun] Available from: http://findarticles.com/p/particles/mim01SW/is2003-april. [ Links ]
27. Prevalence of mental disorders in Europe: results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr Scand. 2004; 109(suppl 1): 21-7. [ Links ]
28. Disability and quality of life impact of mental disorders in Europe: results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr Scand. 2004; 109(suppl 1): 38-46. [ Links ]
29. Hensing G, Wahlstro¨m R. Sickness absence and psychiatric disorders. Scand J Public Health. 2004; 32(suppl 63): 152-80. [ Links ]
30. Hensing G, Andersson L, Brage S. Increase in sickness absence with psychiatric diagnosis in Norway: a general population-based epidemiologic study of age, gender and regional distribution. BMC Med. 2006; 4: 19. [ Links ]
31. Primo GMG. O perfil dos trabalhadores, seu adoecimento e absenteísmo em um hospital público universitário [dissertation] Belo Horizonte: Universidade federal de Minas Gerais; 2008. [ Links ]
32. Brasil, 2012. Law number 7520 of July 15, 1986. Creates the 15th Region of the Labour Court, establishing the appropriate Regional Attorney of the Public Prosecution of the Union to the Labor Court, and other measures. Available from: http://www.jusbrasil.com.br/legislacao/103635/lei-7520-86. [ Links ]
33. Brazil, 2012. Law No. 8,112, from 11 December 1990. Describes the legal situation of public civil servants of the country, autonomous federal agencies and public federal foundations. Diario Oficial Uniao. 1990 Dec 12: 23935. [Cited 2012 Jnun] Available from: http://www.planalto.gov.br/ccivil_03/Leis/L8112cons.htm. [ Links ]
34. World Health Organization ICD-10: international statistical classification of diseases and related health problems. 5.ed. Sao Paulo: Edusp; 1997. p.1191. [ Links ]
35. Bezroukov V. The application of the International Classification of Diseases to dentistry and stomatology. Community Dent Oral Epidemiol. 1979; 7: 21-4. [ Links ]
36. Silva LS, Pinheiro TMM, Sakurai E. Absenteeism profile in state bank in Minas Gerais between 1998 a 2003. Cienc Saude Col. 2008, 13(supl 2): 2049-58. [ Links ]
37. Mazzilli ELN. Labor Dentistry. São Paulo: Santos; 2003. [ Links ]
38. Martins RJ. Absenteeism reasons for dental and medical services in the public and private sectors. Rev Bras Saude Ocup. 2005; 30: 9-15. [ Links ]
39. Diacov N, Lima JRS. Absenteeism Dental. Rev Odontol UNESP. 1988; 17: 183-9. [ Links ]
40. Hito SC. Working conditions and dental absenteeism in a meatpacking industry in Brazil: a contribution to the management of occupational health. [Master's degree dissertation]. São Paulo: Centro Universitário SENAC; 2007. [ Links ]
41. Lima J.R. Absenteeism because dental; comparative analysis between officials of the Municipality of São José dos Campos and policyholders of National Institute of Social Security – INAMPS; 1997. Available from: http://www.odontologia.com.br/artigos.asp. [Access 2012 Jun].
42. Salvador P, Tonhá SQ. Quantitative analysis of licenses for treatment of the very health of servers Court of Audit: support for a model of periodic health. [monoFigurey] Brasília: Faculdade de Economia, Administração, Contabilidade e Ciências da Informação, Universidade de Brasília; 2006. [ Links ]
43. Calle Rovirego B- El trabajo de la mujer. In: Instituto Nacional de Previdenciên. Tratado de hygiene y seguridad del trabajo. Madrid; 1971. p.219-26. [ Links ]
44. Silva D M P P, Marziale M H P. Absenteeism of nursing staff in a university hospital. Rev. Latinoam. Enfermagem. 2000; 8: 44-51. [ Links ]
45. Brasil, 2012. Decree number 7003, dated 9 November 2009. Regulates the license for health care. Available from: http://www.planalto.gov.br/ccivil_03/_Ato2007-2010/2009/Decreto/D7003.htm. [ Links ]
46. Saliba TA, Garbin AIO . The dentist and dental issuing certificates. Odontol. Soc. 2000: 2: 89-92. [ Links ]
47. Reisine ST. Dental disease and work loss. J Dent Res. 1984; 63: 1158-61. [ Links ]
48. Medeiros EP, Bijella VT. Bases for organizing programs for dental workers. Rev.Bras.Odontol. 1970; 27: 303-11. [ Links ]
49. Mazzilli LEN. Analysis of absences from work due to dental municipal public servants São Paulo undergoing occupational expertise in the period from 1996 to 2000 [dissertation]. São Paulo: Faculdade de Odontologia da Universidade de São Paulo; 2004. [ Links ]
50. Flippo E.B. Principles of Personnel Management. São Paulo: Atlas; 1970. [ Links ]
51. Forssman S. El absentismo en la industria. Bol. Oficina Sanit.Panam: 1956; 41: 526-30. [ Links ]
52. Couto H A. Occupational health issues: collection of notebooks Ergo. Belo Horizonte: Ergo; 1987. 432p. [ Links ]
53. Danatro D. Ausentismo laboral de causa médica en una institución pública. Rev. Med.Uruguay: 1997; 13: 101-9. [ Links ]
54. Bispo P. Company achieves low level of absenteeism; 2002. Available from: http://carreiraseempregos.com.br/comunidades//Rh/fiquepordentro/311002_rh_casaverde.shtm. [Access 2012 Jun] [ Links ].
55. Federal Dentistry Council. Available from: http://www.cfo.org.br.[Access 2012 Jun] [ Links ].
 Correspondence:
Correspondence:
Dagmar de Paula Queluz
Departamento de Odontologia Social
Faculdade de Odontologia de Piracicaba - UNICAMP
Avenida Limeira, 901, CEP: 13414900
Piracicaba, SP, Brasil
E-mail: dagmar@fop.unicamp.br
Received for publication: August 12, 2012
Accepted: December 14, 2012
