










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.12 no.1 Piracicaba Jan./Mar. 2013
CASE REPORT
Apexification with white MTA in an immature permanent tooth with dens invaginatus
Anderson de Oliveira Paulo; Mário Tanomaru-Filho; Renato de Toledo Leonardo; Gisselle Moraima Chávez-Andrade; Juliane Maria Guerreiro-Tanomaru
Department of Restorative Dentistry, Araraquara Dental School, UNESP - Univ Estadual Paulista, Araraquara, SP, Brazil
ABSTRACT
Dens invaginatus, also known as "dens in dente", is a developmental dental anomaly resulting in an invagination of the enamel organ into the dental papilla. These cases present technical difficulties to the root canal treatment. Apexification using an apical plug of mineral trioxide aggregate (MTA) has been indicated as an alternative to long-term intracanal use of calcium hydroxide in immature permanent teeth. It is considered as a simple and rapid technique. This paper reports a case of Oehlers' Type 1 dens invaginatus in an immature permanent maxillary right lateral incisor, which presented pulp necrosis secondary to dental trauma and was treated by apexification with white MTA apical plugging followed by conventional root canal therapy. The operative procedures are described and the technique is discussed. The physical and biological properties of MTA, associated with appropriate instrumentation and obturation techniques, make this material an excellent option in the endodontic therapy of immature permanent teeth with dens invaginatus.
Keywords: dens invaginatus, dens in dente, apexification, mineral trioxide aggregate, calcium hydroxide.
Introduction
The term dens invaginatus was coined in 1953 by Hallet1, who made the first documented attempt to classify invaginated teeth, suggesting the existence of four types of invagination based on both clinical and radiographic criteria. This is a term that applies for all of variants of this developmental dental anomaly, which results from an alteration in the normal growth pattern of the dental papilla during odontogenesis, showing a wide array of anatomical variations2-6. The classification system proposed by Oehlers2 in 1957 is probably the most clinically relevant and is by far the most commonly used in clinical studies, case reports and case series6-9. It is based on Hallet's original classification1, but the cases are grouped in three major categories, according to the depth of the invagination and the existence of communication with the pulp tissue or periodontal ligament, regardless of the affected tooth (anterior, posterior, supernumerary). A single tooth can present multiple invaginations, but each one may fall into a different classification: Type 1 - the invagination is confined to the tooth crown, being limited to enamel and not extending beyond the cementoenamel junction (CEJ); Type 2 - the invagination extends apically beyond the CEJ and may or may not have pathways of communication with the dental pulp; Type 3 - the invagination extends apically beyond the CEJ and a second foramen is evident in the periodontal region. There is no communication with the pulp.
New perspectives arose in the practice of dentistry with the development of mineral trioxide aggregate (MTA). MTA has been indicated in endodontics for treatment of perforations, retrograde fillings, pulpotomy and as an apical barrier in cases of immature non-vital teeth, also has antimicrobial properties10-12. It has been extensively demonstrated that MTA is a biocompatible material that stimulates the formation of new cementum on its surface and provides good seal10,12-16. White and gray MTA present similar chemical composition and biological properties12,14,17-18.
The use of an apical plug of MTA has been indicated as an alternative to long-term intracanal use of calcium hydroxide for root-end closure of non-vital immature permanent teeth19-23. Apical plugging with MTA is a simple and rapid technique that eliminates the need of successive intracanal dressing changes10,21. Some authors, however, have advocated that the use of calcium hydroxide-based intracanal dressing followed by preparation of an apical MTA plug should be the treatment of choice for apexification of teeth with incomplete apex formation3,13,18,24.
This paper reports a case of Oehlers' Type 1 dens invaginatus in an immature permanent maxillary right lateral incisor, which presented pulp necrosis secondary to dental trauma and was treated by apexification with white MTA apical plugging followed by conventional root canal therapy.
Case Report
A 9-year-old male child presented for treatment 1 day after sustaining a trauma to the maxillary right lateral incisor. The intraoral clinical examination showed no soft tissue lacerations, no crown or root fracture and no mobility. The preoperative periapical radiograph (Figure 1) showed incomplete root formation with open apices and Type 1 dens invaginatus according to Oelhers' classification. No significant periapical alteration was observed. Since the tooth did not respond to cold and hot stimuli, the patient was scheduled for reevaluation within 2 weeks, but he did not show up. The patient returned 3 months later with a fistula associated with the apical region of the traumatized tooth. A new periapical radiograph showed the development of apical periodontitis (Figure 2).


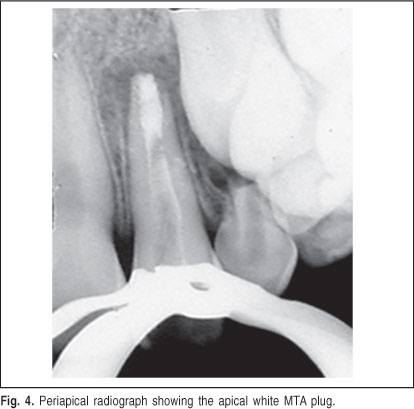
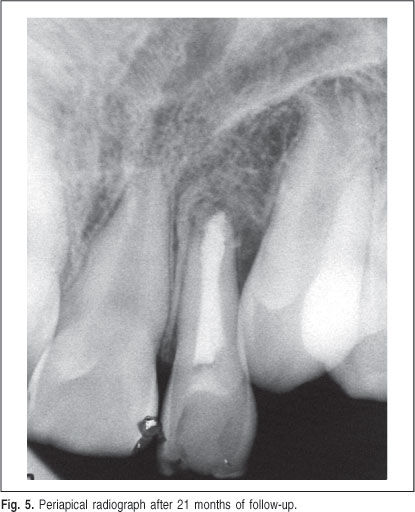
Considering the mode of treatment that is commonly adopted for cases of apexification7,13,18,24, the initial treatment plan was apexification mediated by changes of calcium hydroxide-based intracanal pastes followed by definitive obturation. The coronal access was prepared through the invaginated portion. Monthly changes of the calcium hydroxide-based intracanal medication were done during 6 months, but no progress in apex closure was observed. Therefore, an attempt was made to induce apexification by the placement of an apical plug with white MTA (Angelus Dental Solutions, Londrina, PR, Brazil). After local anesthesia and rubber dam isolation, the provisional restoration was removed access to the root canal was gained. A new determination of root canal length was done with a size 80 K-file, and the total root length was established as being 20 mm (Figure 3). The root canal was instrumented with a size 80 K-file, irrigated with a 1% sodium hypochlorite solution followed by a final flush with EDTA (Byodinamic Europe S.L., Ibiporã, PR, Brazil) and dried with sterile absorbent paper points. The MTA powder and liquid components were mixed according to the manufacturer's instructions and a size 70 K-file was used to prepare a 4-mm-thick apical white MTA plug by repeated movements of file insertion and removal in an anticlockwise direction (Figure 4). Excess MTA was removed from the canal walls and the remainder of the canal was obturated by lateral condensation of gutta-percha and Sealer 26 endodontic sealer (Dentsply Industry and Trade Ltda., Rio de Janeiro, RJ, Brazil). The coronal portion was restored with composite resin. The final radiographs showed a well-obturated root canal. The 21-month post treatment follow-up showed clinical and radiographic success (Figure 5).

Discussion
The etiology of dens invaginatus remains controversial. Most authors2,5-6,9,25 describe its origin in a distortion of the enamel organ causing a protrusion inside the dental papilla, which produces an invagination of the tooth crown before calcification. Also, a genetic source may be a significant factor6,8,26. According to the literature, the prevalence of dens invaginatus ranges from 0.03 to 10%4,6,26-27 and there is a female-to-male predominance of 3:16. The permanent maxillary right lateral incisors are the most commonly affected teeth4,6,26, being bilateral in over 40-43% of the cases5,8-9,25, followed in a decreasing order of prevalence by central incisors, canines, premolars and molars7. The importance of an accurate and early diagnosis is justified because pathways of communication with the oral cavity can be created in invaginated teeth. This permits the penetration of irritating agents and microorganisms into the pulp tissue and leading to potential complications, namely caries disease, internal resorption, pulp necrosis, apical periodontitis and apical cyst formation2,8,26.
In the present case, the tooth was classified as having dens invaginatus Type 1, according to Oehlers' classification2. Depending on the type of malformation and the communication of the invagination with the pulp tissue, the clinician may confine the endodontic therapy to the invaginated portion and, as a result, preserve pulp vitality. However, in most cases, the endodontic treatment must include both the invagination and the root canals. The task can become even more challenging, considering the multiple anatomical variations that a dens invaginatus may present within the root canal system. Complete debridement of the root canal system can be compromised by limited access and as a result some areas may remain uninstrumented when a conventional technique is used. In order to overcome these limitations, some researchers have suggested that the invagination is removed under the operating microscope26. In the present case, the access to the canals was gained through the invaginated portion. If nonsurgical endodontic therapy fails, a combined approach with apical surgery may be indicated.
Pulp involvement can occur at an early age when the roots are not completely formed. The large and irregular volume of the root canal system of invaginated teeth is an additional challenge for cleaning, shaping and instrumentation.
The endodontic therapy of choice for non-vital immature teeth is apexification, which is the induction of apical closure to produce more favorable conditions for conventional root canal filling. Calcium hydroxide is the most commonly advocated medicament because, in addition to a low cost, its efficacy to induce the formation of an apical mineralized barrier is well documented15,16 even in cases of dens invaginatus with necrotic pulp7,9,27. However, apexification with calcium hydroxide requires successive changes of the intracanal medication that may last for several months, which may increase the risk of coronal leakage and recontamination of the root canal system. In addition, there have been reports on the decrease of the fracture strength of teeth subjected to long-term intracanal use of calcium hydroxide to induce apexification13,15,20 and considerable interest has been expressed in the use of other materials, such as MTA.
The use of MTA alternatively to calcium hydroxide has become increasingly widespread. Several studies10,22,28-29 showed that pediatric dentists in the world had used MTA or arranged for its use in apical barrier formation in non-vital immature permanent teeth. Kusgoz et al.10 and Erdem and Sepet21 reported clinical cases in which MTA was used as a filling material in traumatized teeth with necrotic pulp and open apices and concluded that MTA can be considered a very effective option for apexification of traumatized and immature permanent teeth with the advantage of shorter treatment time, good sealing ability and high biocompatibility. D'Arcangelo and D'Amario18 reported two cases of apexification with apical MTA plug after intracanal use of calcium hydroxide, in the same way as used in the present study. The presentation of these cases confirms that MTA acts as an apical barrier and can be considered as an effective material to support regeneration of apical tissues in immature teeth with necrotic pulp for both young and adult patients.
MTA may be used in the treatment of dens invaginatus3,26. Bogen and Kuttler30 report a Type 2 dens invaginatus with periapical periodontitis treated using an apical plug of MTA. A paper describes the use of MTA in two cases of dens invaginatus which were prepared with ultrasonic instrumentation under magnification26. Silberman et al. 25 reported a case of dens invaginatus in an immature tooth that was successfully treated with the placement of an apical plug of gray MTA and conventional endodontics. In the present case, the apical plug was prepared with white MTA, which has similar properties14,23.
In conclusion, apical plugging with MTA for induction of apexification allows for completing the treatment in a single session, which can be preceded by another session for placement of a calcium hydroxide-based intracanal medication in teeth with infected root canals. The physical and biological properties of MTA, associated with appropriate instrumentation and obturation techniques, make this material an excellent option in the endodontic therapy of immature permanent teeth with dens invaginatus.
References
1. Hallett GE. Incidence, nature, and clinical significance of palatal invaginations in the maxillary incisor teeth. Proc R Soc Med. 1953; 46: 491-9. [ Links ]
2. Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957; 10: 1204-18. [ Links ]
3. Paula-Silva FW, Rocha CT, Flores DS, Nelson-Filho P, Silva LA, Queiroz AM. Root canal treatment of an immature dens invaginatus with apical periodontitis: a case report. J Dent Child (Chic). 2011; 78: 66-70. [ Links ]
4. Gharechahi M, Ghoddusi J. A nonsurgical endodontic treatment in open-apex and immature teeth affected by dens invaginatus: using a collagen membrane as an apical barrier. J Am Dent Assoc. 2012; 143: 144-8. [ Links ]
5. Khan SA, Khan SY, Bains VK, Bains R, Loomba K. Dens invaginatus: review, relevance, and report of 3 cases. J Dent Child (Chic). 2012; 79: 143-53. [ Links ]
6. Kallianpur S, Sudheendra U, Kasetty S, Joshi P. Dens invaginatus (Type III B). J Oral Maxillofac Pathol. 2012; 16: 262-5. [ Links ]
7. Kalaskar R, Kalaskar AR. Nonsurgical treatment of periapical lesion associated with type III dens invaginatus using calcium hydroxide: a case report. J Indian Soc Pedod Prev Dent. 2008; 26(Suppl 2): S72-5. [ Links ]
8. Alani A, Bishop K. Dens invaginatus. Part 1: classification, prevalence and aetiology. Int Endod J. 2008; 41: 1123-36. [ Links ]
9. Borges AH, Semenoff Segundo A, Nadalin MR, Pedro FL, da Cruz Filho AM, Sousa-Neto MD. Conventional Treatment of Maxillary Incisor Type III Dens Invaginatus with Periapical Lesion: A Case Report. ISRN Dent 2011; 2011: 257609. doi: 10.5402/2011/257609. [ Links ]
10. Kusgoz A, Yildirim T, Tanriver M, Yesilyurt C. Treatment of horizontal root fractures using MTA as apical plug: report of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107: e68-72. [ Links ]
11. Tanomaru JM, Tanomaru-Filho M, Hotta J, Watanabe E, Ito IY. Antimicrobial activity of endodontic sealers based on calcium hydroxide and MTA. Acta Odontol Latinoam. 2008; 21: 147-51. [ Links ]
12. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review-Part I: chemical, physical, and antibacterial properties. J Endod. 2010; 36: 16-27. [ Links ]
13. Moore A, Howley MF, O'Connell AC. Treatment of open apex teeth using two types of white mineral trioxide aggregate after initial dressing with calcium hydroxide in children. Dent Traumatol. 2011; 27: 166-73. [ Links ]
14. Porter ML, Berto A, Primus CM, Watanabe I. Physical and chemical properties of new-generation endodontic materials. J Endod. 2010; 36: 524-8. [ Links ]
15. Trope M. Treatment of the immature tooth with a non-vital pulp and apical periodontitis. Dent Clin North Am. 2010; 54: 313-24. [ Links ]
16. Stefopoulos S, Tzanetakis GN, Kontakiotis EG. Non-surgical retreatment of a failed apicoectomy without retrofilling using white mineral trioxide aggregate as an apical barrier. Braz Dent J. 2012; 23: 167-71. [ Links ]
17. da Silva EJ, Andrade CV, Tay LY, Herrera DR. Furcal-perforation repair with mineral trioxide aggregate: Two years follow-up. Indian J Dent Res. 2012; 23: 542-5. [ Links ]
18. D'Arcangelo C, D'Amario M. Use of MTA for orthograde obturation of nonvital teeth with open apices: report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104: e98-101. [ Links ]
19. Annamalai S, Mungara J. Efficacy of mineral trioxide aggregate as an apical plug in non-vital young permanent teeth: preliminary results. J Clin Pediatr Dent. 2010; 35: 149-55. [ Links ]
20. Bidar M, Disfani R, Gharagozloo S, Khoynezhad S, Rouhani A. Medication with calcium hydroxide improved marginal adaptation of mineral trioxide aggregate apical barrier. J Endod. 2010; 36: 1679-82. [ Links ]
21. Erdem AP, Sepet E. Mineral trioxide aggregate for obturation of maxillary central incisors with necrotic pulp and open apices. Dent Traumatol. 2008; 24: e38-41. [ Links ]
22. Mooney GC, North S. The current opinions and use of MTA for apical barrier formation of non-vital immature permanent incisors by consultants in paediatric dentistry in the UK. Dent Traumatol. 2008; 24: 65-9. [ Links ]
23. Stefopoulos S, Tsatsas DV, Kerezoudis NP, Eliades G. Comparative in vitro study of the sealing efficiency of white vs grey ProRoot mineral trioxide aggregate formulas as apical barriers. Dent Traumatol. 2008; 24: 207-13. [ Links ]
24. Holden DT, Schwartz SA, Kirkpatrick TC, Schindler WG. Clinical outcomes of artificial root-end barriers with mineral trioxide aggregate in teeth with immature apices. J Endod. 2008; 34: 812-7. [ Links ]
25. Silberman A, Cohenca N, Simon JH. Anatomical redesign for the treatment of dens invaginatus type III with open apexes: a literature review and case presentation. J Am Dent Assoc. 2006; 137: 180-5. [ Links ]
26. Alani A, Bishop K. The use of MTA in the modern management of teeth affected by dens invaginatus. Int Dent J. 2009; 59: 343-8. [ Links ]
27. Carvalho-Sousa B, Almeida-Gomes F, Gominho LF, Albuquerque DS. Endodontic treatment of a periradicular lesion on an invaginated type III mandibular lateral incisor. Indian J Dent Res. 2009; 20: 243-5. [ Links ]
28. Doyle TL, Casas MJ, Kenny DJ, Judd PL. Mineral trioxide aggregate produces superior outcomes in vital primary molar pulpotomy. Pediatr Dent. 2010; 32: 41-7. [ Links ]
29. Subramaniam P, Konde S, Mathew S, Sugnani S. Mineral trioxide aggregate as pulp capping agent for primary teeth pulpotomy: 2 year follow up study. J Clin Pediatr Dent. 2009; 33: 311-4. [ Links ]
30. Bogen G, Kuttler S. Mineral trioxide aggregate obturation: a review and case series. J Endod. 2009; 35: 777-90. [ Links ]
 Correspondence:
Correspondence:
Mário Tanomaru Filho
Rua Humaitá, 1680, Caixa Postal 331, Centro
CEP: 14801-903 Araraquara, SP, Brasil
Phone: +55 16 33016390 Fax. +55 16 33016392
E-mail: tanomaru@uol.com.br
Received for publication: July 06, 2012
Accepted: November 11, 2012
