










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.13 no.2 Piracicaba Abr./Jun. 2014
ORIGINAL ARTICLE
Oblique or orthoradial CBCT slices for preoperative implant planning: which one is more accurate?
Frederico Sampaio NevesI; Taruska Ventorini VasconcelosII; Anne Caroline Costa OenningII; Sergio Lins de-Azevedo-VazIII; Solange Maria de AlmeidaII; Deborah Queiroz FreitasII
I União Metropolitana de Educação e Cultura – UNIME, School of Dentistry, Departament of Clinical and Surgical Propaedeutics, Salvador, BA, Brazil
II Universidade Estadual de Campinas – UNICAMP, School of Dentistry, Department of Oral Diagnosis, Piracicaba, SP, Brazil
III Universidade Federal do Espírito Santo – UFES, School of Dentistry, Department of Clinical Dentistry, Vitoria, ES, Brazil
ABSTRACT
Aim: To assess which slice inclination would be more accurate in measuring sites for implant placement: the oblique or the orthoradial slice. Methods: Five regions of eight edentulous mandibles were selected (incisor, canine, premolar, first molar and second molar). The mandibles were scanned with a Next Generation i-CAT CBCT unit. Two previously calibrated oral radiologists performed vertical measurements in all the selected regions using both the oblique and orthoradial slices. The mandibles were sectioned in all the evaluated regions in order to obtain the gold standard. The Wilcoxon signed rank test compared the measurements obtained in the oblique and orthoradial slices with the gold standard. Results: The bone height measurements for the first and second molar regions using the orthoradial slices were statistically different from the gold standard. Conclusions: Using the orthoradial slices to obtain cross-sectional images may offer insufficient accuracy for implant placement in the posterior region.
Keywords: cone-beam computed tomography; dental implants; mandible; software.
Introduction
Cone beam computed tomography (CBCT) is a radiographic method that has been used in several areas of Dentistry, because it shows three-dimensional images of the dental structures with high contrast1. This image modality became commercially viable and suitable in the dental practice given its small dimension, easy handling, inherently fast image acquisition, relatively low cost and radiation doses1-3.
Dental implant placement depends remarkably on the estimation of the distance between anatomical landmarks and bone dimensions, in which the surgeon uses linear CBCT measurements. Inaccurate bone measurements can lead to a risky relationship between the dental implant and important anatomical structures (e.g. mandibular canal and mental foramen). It may result in injury to the neurovascular bundle and cause some postoperative complaints such as neuroma, paresthesia, anesthesia and hemorrhage4-5.
It has been stated that CBCT anatomical linear measurements are accurate and reliable6-13. However, the inclination of the patient's head during CBCT image acquisition can cause distortion in measurements for preoperative implant planning14-17. On the other hand, there are several types of software designed to assess CBCT images; some of them allow the operator obtaining oblique slices while others do not. The hypothesis of this study is weather the inclination of the slices would be relevant for preoperative implant planning. Therefore, this study aimed to assess which slice would be more accurate in measuring sites for implant placement: the oblique or the orthoradial slice.
Material and methods
This study was conducted after approval from the Ethic Research Committee of UNICAMP's School of Dentistry, Brazil. Eight dry mandibles (totaling 16 hemi-mandibles) with completely resorbed alveolar processes were selected to the study.
The regions to be assessed were determined according the criteria proposed by Neves et al. (2012)13: incisive (1 cm distal from the median sagittal plane), canine (1 cm distal from the incisive region), premolar (at the mental foramen level), first molar (1 cm distal from the mental foramen) and second molar (2 cm distal from the mental foramen) regions. One of the investigators (TVV) draw perpendicular lines to the base of the mandibles with a permanent marker pen (BIC, Cajamar, SP, Brazil) and fixed a 0.7-mm sphere with a radiopaque marker (gutta-percha point) in all extension of the buccal cortical plate above each line (Fig. 1). These procedures aimed at establishing controlled sites, i.e. standard regions for measurements.

In order to simulate soft-tissue attenuation, each mandible was placed in a polystyrene box filled with water prior to the CBCT examination. The mandibles were scanned with a Next Generation i-CAT CBCT unit (Imaging Sciences International, Inc, Hatfield, PA, USA), under specific exposure parameters: 8x8 cm field of view (FOV), full-scan mode (360°), 37.07 mA, 120 kVp, 0.20 mm voxel size and 26.9 s exposure time.
All measurements were performed in cross-sectional images using the OnDemand3D®™ software (version 1.0, CyberMed Inc., Seoul, South Korea) with both oblique and orthoradial slices (Fig. 2). The investigator adjusted the oblique slices by inclination of the cutting plane in the multiplanar reconstruction (MPR) view, until the slice showed all the gutta-percha point in the extension of the buccal cortical plate. The orthoradial slices were obtained by using the curved planar reformat tool of the software to create crosssectional images, without any adjustment to the gutta-percha points. The investigator positioned the cutting lines at the center of the radiopaque spheres for both the oblique and orthoradial slices and saved the images as projects, so the observers only had to open the projects to assess the images without moving or adjusting any line. This procedure guaranteed that all observers assessed the same regions.
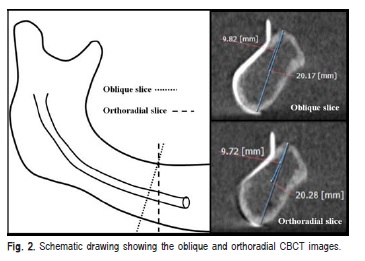
Under dim light conditions, two previously calibrated oral radiologists with 5-years of CBCT experience assessed independently the saved projects to obtain the measurements. The observers obtained the bone height by measuring the distance from the upper to the lowest point in the cortical boundaries of the mandibular body in all the predefined regions of the mandible. Additionally, they measured the distance from the superior cortical ridge of the mental foramen (premolar region) or the mandibular canal (molar regions) to the highest point of the alveolar ridge (Fig. 2). The mandibular canal could not be precisely located in six hemi-mandibles so these measurements were not obtained.
After the observers measured all images, the mandibles were sectioned using an electric saw in all the assessed regions. The slices were done immediately before the drawn lines, so the bone tissue in the site related to the tomographic image was not lost. The investigator obtained the vertical measurements for each site using a digital caliper (SC-6 digital caliper; Mitutoyo Corporation, Tokyo, Japan), repeating three times the direct measurements. The means of these measurements were considered the gold standard for the study (Fig. 3).

Data were analyzed using the SPSS version 18.0 software (Statistical Package for the Social Sciences, Chicago, IL, USA). The variables and factors in study were the measurements and post-processing view (oblique or orthoradial), respectively. The intraclass correlation coefficient (ICC) quantified the interobserver agreement. Descriptive statistics were calculated as mean and standard deviation. The Wilcoxon signed rank test compared the measurements obtained in the oblique and orthoradial slices to the gold standard. The null hypothesis considered that the orthoradial and the oblique slices would not result in statistically significant differences from the gold standard. The significance level was set at 5%.
Results
The interobserver agreement found in the study was excellent (ICC = 0.99; 95% confidence interval [CI] = 0.99 - 0.99).
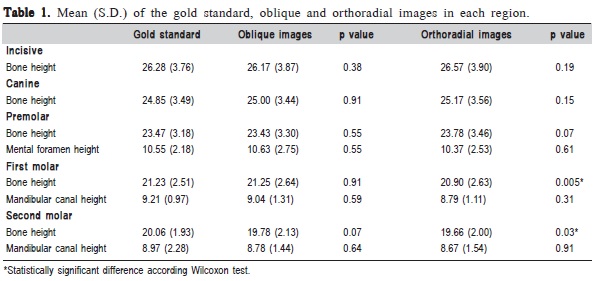
Table 1 shows the mean and standard deviation values of the measurements obtained using the digital caliper (gold standard), the oblique and the orthoradial slices. The results from the Wilcoxon test are also shown for the comparisons of oblique and orthoradial slices vs gold standard. The null hypothesis was only rejected after measuring bone height for the first and second molar regions using the orthoradial slice (p<0.05). These measurements were underestimated in comparison with the gold standard.
Discussion
In this study, the oblique slices were obtained by inclination of the cutting plane in the MPR view while the orthoradial slices were obtained using the curved planar reformat tool to create cross-sectional images. The MPR and especially the cross-sectional images are the views that clinicians mostly use when assessing CBCT images. In some CBCT software – like the one that was used in the study – while the MPR images allow tilting the cut plane along an object of interest (represented in this study by the gutta-percha point), the orthoradial images mostly do not. Therefore, it was aimed at assessing which of the two slices was the most accurate in determining measurements for implant placement.
The literature advises that implants should be placed with their axis parallel to the oclusal forces. Therefore, implant axial angulation should be planned to distribute the occlusal forces vertically along the implant axis18. Considering the Spee curve, where the maxillary posterior teeth are slightly tilted distally, implants in the posterior region of the mandible may require a mesio-inclined position. Also, the adoption of tilted implants has been proposed to avoid injury to the alveolar inferior nerve in edentulous maxilla/mandible cases19. Therefore, it was speculated if the use of orthoradial images - which are very much used by clinicians – would be accurate enough for preoperative planning of tilted implants. The hypothesis was that the clinician should consider the orientation of the implant axis in order to guide accordingly the tomographic cutting plane.
The results demonstrated statistically significant differences between the orthoradial slices and the gold standard for bone height in the first and second molar regions. The other regions and the oblique slice did not provide any statistically significant differences from the gold standard, which indicated that most of the measurements performed in both slices were accurate. This is also demonstrated by the mean values of the measurements performed with the digital caliper (gold standard), the oblique and the orthoradial slices, which were all close to each other.
The gutta-percha points fixed along the buccal cortical plate of the mandibles aimed to set radiopaque marks in the regions to be assessed by the observers. They represented the inclination of hypothetically planned implants. As only the oblique slices could be adjusted along the gutta-percha points, they were more accurate in measuring both the bone and mandibular canal height in the first and second molar regions. It is important to consider that inferior alveolar nerve injury can result in some postoperative complaints, and it is more prone to occur when the length of the implant to be placed is greater than the implant site4,13. This can lead to higher morbidity and additional treatment costs for the patient.
Several studies have shown the influence of maxillomandibular inclination in the bone measurements14-17. Variations in the patient position during CBCT image acquisition can lead to inaccurate bone height and width measurements in different regions of the maxilla and mandible. When the planning is incorrect, important anatomical structures may be harmed, such as the nasal cavity floor and the incisor branch of the inferior alveolar nerve. Dantas et al. (2008)14 and Visconti et al. (2013)17 evaluated the influence of mandible positioning in bone height measurements taken in CT and CBCT images, respectively. The authors reported that for some slices in the orthoradial image, principally those in the premolar region, at the site of what appeared to be the anatomical repair corresponding to the studied area, the radiopaque marker was not present. This confirmed that the considered differences did not correspond to distortions in the reformatted images, but to the performance of measurements at different locations. In this format, the slices obtained would not be perpendicular to the mandible base, but they rather would be oblique in relation to the reference system. This principle may be used in the present study, due to the fact that the oblique and orthoradial slices are in different positions, the radiopaque marker not being completely observed in the orthoradial images.
In the present study, no statistically significant differences were found in the anterior region of the mandible comparing both the orthoradial and oblique slices with the gold standard. This corroborates other authors14,15,17, because they also did not find differences in the anterior region comparing different positions of the skull with normal position. This could probably be justified by the fact that the anterior region of the mandible is straighter, remaining more perpendicular to the horizontal plane when compared with the posterior regions.
The observers could not locate the mandibular canal in six hemi-mandibles, which is justified by the reduction of mineral bone density caused by old age and teeth loss. Lindh et al. (1995)20 found that the compact bone surrounding the neurovascular bundle was missing in some histological sections of edentulous mandibles, with the result that the canal could not be identified in radiographs.
In conclusion, the preoperative planning for implant placement in mandibles using CBCT orthoradial slices to obtain cross-sectional images should be made with special caution. These images may offer insufficient accuracy for implant placement in the posterior region, especially when planning tilted implants.
References
1. Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am. 2008; 52: 707-30. [ Links ]
2. Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol. 1998; 8: 1558-64.
3. Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999; 28: 245-8.
4. Neves FS, de Almeida SM, Bóscolo FN, Haiter-Neto F, Alves MC, Crusoé-Rebello I. et al. Risk assessment of inferior alveolar neurovascular bundle by multidetector computed tomography in extractions of third molars. Surg Radiol Anat. 2012; 34: 619-24.
5. Neves FS, Nascimento MC, Oliveira ML, Almeida SM, Bóscolo FN. Comparative analysis of mandibular anatomical variations between panoramic radiography and cone beam computed tomography. Oral Maxillofac Surg. 2013 Aug 24. (in press).
6. Lascala CA, Panella J, Marques MM. Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCTNewTom). Dentomaxillofac Radiol. 2004; 33: 291-4.
7. Kamburoðlu K, Kiliç C, Ozen T, Yüksel SP. Measurements of mandibular canal region obtained by cone-beam computed tomography: a cadaveric study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107: e34-42.
8. Kim TS, Caruso JM, Christensen H, Torabinejad M. A comparison of cone-beam computed tomography and direct measurement in the examination of the mandibular canal and adjacent structures. J Endod. 2010; 36: 1191-4.
9. Ganguly R, Ruprecht A, Vincent S, Hellstein J, Timmons S, Qian F. Accuracy of linear measurement in the Galileos cone beam computed tomography under simulated clinical conditions. Dentomaxillofac Radiol. 2011; 40: 299-305.
10. Panmekiate S, Apinhasmit W, Petersson A. Effect of electric potential and current on mandibular linear measurements in cone beam CT. Dentomaxillofac Radiol. 2012; 41: 578-82.
11. Torres MG, Campos PS, Segundo NP, Navarro M, Crusoé-Rebello I. Accuracy of linear measurements in cone beam computed tomography with different voxel sizes. Implant Dent. 2012; 21: 150-5.
12. Waltrick KB, Nunes de Abreu Junior MJ, Corrêa M, Zastrow MD, Dutra VD. Accuracy of linear measurements and visibility of the mandibular canal of cone-beam computed tomography images with different voxel sizes: an in vitro study. J Periodontol. 2013; 84: 68-77.
13. Neves FS, Vasconcelos TV, Campos PS, Haiter-Neto F, Freitas DQ. Influence of scan mode (180°/360°) of the cone beam computed tomography for preoperative dental implant measurements. Clin Oral Implants Res. 2014; 25: 155-8.
14. Dantas JA, Montebello Filho A, Campos PS. Computed tomography for dental implants: the influence of the gantry angle and mandibular positioning on the bone height and width. Dentomaxillofac Radiol. 2005; 34: 9-15.
15. Tomasi C, Bressan E, Corazza B, Mazzoleni S, Stellini E, Lith A. Reliability and reproducibility of linear mandible measurements with the use of a cone-beam computed tomography and two object inclinations. Dentomaxillofac Radiol 2011; 40: 244-50.
16. Sheikhi M, Ghorbanizadeh S, Abdinian M, Goroohi H, Badrian H. Accuracy of linear measurements of Galileos cone beam computed tomography in normal and different head positions. Int J Dent. 2012; 214954. doi: 10.1155/2012/214954.
17. Visconti MA, Verner FS, Assis NM, Devito KL. Influence of maxillomandibular positioning in cone beam computed tomography for implant planning. Int J Oral Maxillofac Surg. 2013; 42: 880-6.
18. Machtei EE, Oettinger-Barak O, Horwitz J. Axial relationship between dental implants and teeth: A radiographic study. J Oral Implantol. 2012 Sep 10. (in press).
19. Del Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. Clin Implant Dent Relat Res. 2012; 14: 612-21.
20. Lindh C, Petersson A, Klinge B. Measurements of distances related to the mandibular canal in radiographs. Clin Oral Implants Res. 1995; 6: 96-103.
 Correspondence:
Correspondence:
Frederico Sampaio Neves
Departamento de Propedêutica Clínica e Cirúrgica, União Metropolitana de Educação e Cultura – UNIME
Rua Professor Fernando Rocha, 326
CEP: 41194-020 - Saboeiro, Salvador, BA, Brasil
E-mail: fredsampaio@yahoo.com.br
Received for publication: April 30, 2014
Accepted: June 03, 2014
