










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.13 no.2 Piracicaba Abr./Jun. 2014
ORIGINAL ARTICLE
Dental caries in inland Brazilian adolescents and its relationship with social determinants
Andréa Videira AssafI; Angela Scarparo Caldo-TeixeiraI; Flavia Maia SilveiraI; Maria Isabel Bastos ValenteI; Rafael Gomes DitterichII; Roberta BarcelosI
I Universidade Federal Fluminense – UFF, Nova Friburgo Dental School, Department of Specific Formation, Nova Friburgo, RJ, Brazil
II Universidade Federal do Paraná – UFPR, Dental School, Department of Community Health, Curitiba, PR, Brazil
ABSTRACT
Aim: To identify the prevalence of dental caries in inland Brazilian adolescents, and to analyze the influence of socio-demographic and clinical variables, and access to dental service on caries experience. Methods: This study had a non-probabilistic sample comprising 504 adolescents aged 12 years, attending public schools in the city of Nova Friburgo, mountain region of Rio de Janeiro, Brazil. The World Health Organization (WHO, 1997) criterion was used by previously calibrated examiners to report dental caries. Variables were obtained by means of a semistructured questionnaire applied to the adolescents' parents. Results: The D3MFT mean was 1.90 and the Significant Caries (SIC) Index was 4.54, mainly represented by the carious component. Multiple logistic regression analysis revealed that parents with over 8 years of schooling (OR=0.579), absence of pain (OR=0.396) and not visiting the dentist (OR=0.270) might suggest protective factors against the disease; the possible risk factors were male gender (OR=1.982) and pain, extraction and others were reasons for consultation (OR=2.435). Conclusions: Although the prevalence of caries was slightly below the national mean, polarization of the disease was clearly observed. Education and no access to the dentist led to protection against the disease. These results may contribute to planning of oral health actions directed towards this target population for the control of caries.
Keywords: risk factors; social class; dental caries.
Introduction
Many scientific investigations have been published over the last few years, showing what is generally accepted: the pattern of dental caries has decreased in the last decades, especially among younger groups in most developed countries1. This has been mainly associated with factors such as public water supply fluoridation and the dissemination of fluoridated dentifrices1-3.
In spite of the trend towards a reduction in dental caries, it is still considered a priority disease, especially in developing countries such as Brazil, and this has been demonstrated in the latest national epidemiological surveys4-5. In this context, the polarization of the disease has been observed in groups of younger individuals, with highest incidence (80%) concentrated in a small group of individuals (25 to 30%). This has led to the premise of concentrating efforts especially on certain geographic regions and underprivileged socio-economic groups6.
With this in mind, the development of studies focused on investigating the influence of social inequalities on the caries process have become the basic line of approach to a broader understanding of the multifactorial dynamics of the disease, identification of the most vulnerable groups and making the best decisions, based on identifying these groups and directing care towards them6-7.
In addition to the socio-economic determinants, there has been a welcome emphasis on studies that have pointed out the influence of other factors, both material and symbolic, such as the conditions of the physical, political and cultural environment, aspects related to social behaviors, selfperception and social interaction, on the development of dental caries8. Thus, there has been a continuous endeavor to reach broader understanding of the factors involved in the caries process, in order to achieve the desired improvement and technological development focused on care and attention to oral health, based on the planning and adoption of ethical and equitable public policies for the entire society.
No epidemiological survey has ever been conducted to obtain data on the oral health of adolescents in the city Nova Friburgo, RJ, Brazil. In addition, public water fluoridation, supported by the National Oral Health Policy9, has recently been introduced in that municipality. Therefore, studies aimed at identification and longitudinal monitoring are of utmost importance to measure the impact of this factor on the caries and fluorosis indicators on the different population groups.
The aims of the present study were: to identify the prevalence of dental caries in 12-year-old adolescents in the municipality of Nova Friburgo, RJ, Brazil; to analyze the influence of socio-demographic and clinical variables and access to dental services on caries experience; and to provide "baseline" data, which will serve as a reference for future comparisons of the effects of public water fluoridation on the incidence of dental caries among adolescents.
Material and methods
Ethical Aspects
This study was approved by the Research Ethics Committee of the Universidade Federal Fluminense at Nova Frigurgo (UFF/NF), in accordance with the National Health Council, Ministry of Health resolution 196/96, Process CEP/ CMM/HUAP n.272/2010 - CAAE n. 0217.0.258.000-10. The participants in the study who needed dental treatment were referred to the School of Dentistry of the UFF/NF.
Correspondence was first sent to the Municipal and State Secretaries for Education and later authorization was granted to carry out the project. After this, the directors the Public Schools in the municipality were contacted and granted their support for conducting the research. Parents/guardians of the adolescents also gave authorization by signing an informed consent form. The adolescent was enrolled in the study only after this document was properly filled out and returned to the researchers.
Study Design
- Characterization of the Municipality and Sample Selection
The present cross-sectional study consisted in evaluating the residents of the city of Nova Friburgo, located in the mountain region of the Rio de Janeiro State, Brazil,which has a total area of 938.5 km² and a 0.81 Human Development Index (HDI). The municipality has 8 districts, comprising rural (12.5%) and urban (87.5%) areas, with varying demographic, environmental, socio-economic and cultural characteristics. Regarding schooling, these characteristics are worse in comparison with entire Rio de Janeiro State population, presenting the percentages of 49.5% (Nova Friburgo) and 39.1% (Rio de Janeiro State) for the population group with fewer than 8 years of schooling10, but, the municipality provides differentiated oral health services.
The main economic activities in the municipality are agricultural production in the rural zone and underwear manufactures in both rural and urban zones.
The sample comprised 12-year-old adolescents from all the 43 state and municipal public schools in Nova Friburgo, which corresponded to 1081 individuals, representing 76.47% of the individuals in this age group in the Municipality. The remaining adolescents were enrolled in private teaching institutions.
For sample calculation, a population of 12-year-old adolescents resident in the municipality in the year of 2012 was considered, with a precision of 5% and confidence interval of 95%, for a prevalence of 50% of the disease, since the municipality has no information about dental caries. Thus, the largest possible sample was obtained, considering a sample loss of 20% and this resulted in a minimum sample of 461 individuals.
Individuals were randomly selected from lists of students enrolled in all public schools. The exclusion criteria for participation in the study were: adolescents whose parents/ guardians did not grant permission for participation in the study; or who did not fully respond to the questionnaire, and adolescents with debilitated health. The final sample size was 504 adolescents, which is a larger number than the one calculated for minimum sample.
Preparatory Stage: Pilot Study and Calibration of Examiners
- Pilot Study
The pilot study was conducted before the fieldwork, with adolescents (n=20) and their respective parents/ guardians, from rural and urban regions. The purpose was to verify the parents/guardians' understanding of the questionnaire and training the researchers as examiners to conduct the study. In addition, some of the parameters with regards to the epidemiological evaluation were reviewed, such as the approach to performing the clinical exams on the adolescents. For this latter requisite, learning was complemented with the stage of examiner training and calibration.
- Examiner Training and Calibration
The entire process of training the five examiners was carried out under the supervision of a researcher experienced in epidemiological surveys, for a 20 h period.
In order to provide an initial training phase, theoretical discussions (4 h) and presentation of clinical photographic slides with examples of each criterion were organized. Next, clinical training sessions (8 h) were performed, followed by calibration exercises (8 h). For every period of clinical training, each examiner evaluated 10 to 12 adolescents from a public school of Nova Friburgo, with different levels of dental caries prevalence. In this phase, all examiners discussed about the clinical dental diagnosis to establish a criterion of consensus for the group. After this phase, the examiners undertook two calibration exercises with a 1-week interval between them. A mean kappa interexaminer value of 0.80 was obtained. Duplicate exams in 10% of the sample were performed by the examiners during the field research, in order to calculate the intraexaminer Kappa, where a mean value of 0.89 was obtained.
Field Stage: Questionnaires, Exams and Epidemiological Criteria
- Semi-structured Questionnaires
In this second stage the semi-structured questionnaires were handed over to the adolescents' parents/guardians. The semi-structured questionnaire, previously tested in the pilot study, was applied to collect information relative to: 1) sociodemographic characterization of the family; 2) clinical aspects and 3) access to dental services. This data collection instrument was based on the methodology proposed by the last national oral health survey5.
- Clinical Evaluation
The clinical evaluation of dental caries in the adolescents was performed under natural light, by previously calibrated researchers, with the study subjects seated on ordinary chairs. Millimeter periodontal probes with rounded tips (WHO 621) and plane No.5 dental mirrors were used. The exams were conducted in accordance with the methodology recommended by the WHO11. Before the exam, the schoolchildren performed toothbrushing with fluoridated dentifrice under supervision of the researchers, to help removing dental biofilm and/or food remains that were left on the tooth surfaces, thereby facilitating visual diagnosis.
- Codes and criteria used for clinical evaluation
The indices used for measuring dental caries were the D3MFT (total number of decayed, lost and filled teeth) and SCI (Significant Caries Index)12, for permanent dentition, according to the criteria and codification of the WHO Oral Health Surveys Basic Methods handbook11. The subjects were also evaluated for the presence or absence of fluorosis, using the Dean index11 for diagnosis.
Statistical Analysis
Descriptive analyses of the data were carried out made by calculating the distribution of the independent variables in the sample, the D3MFT index and its respective components, percentage of caries-free individuals and SCI11-12.
For the bi- and multivariate analyses, D3MFT was considered the dependent variable (dichotomized by the median into D3MFT<1 and D3MFT>1)13. All the independent variables were dichotomized as follows13: zone (rural and urban), gender (female and male), fluorosis (absence and presence), number of residents in the house (<4 and >4), family income (by the median: <3 and >3 Brazilian minimum wages), number of assets (by the median: d"7 and >7), parents' schooling (<8 and >8 years of schooling), need for treatment (yes and no), presence of pain (yes and no), visit to the dentist (yes and no), type of service used (public and private), reason for consultation (routine and pain/extraction/others), problems of an oral nature - e.g.: difficulty to eat, to brush the teeth - and of a general nature - e.g.: irritability, embarrassment to smile, talk, to go parties, difficulties to play sports, problems with sleeping or studying - due to the condition of the teeth (yes and no). The Chisquare test at 5% level of significance was used to test the association of the independent variables with the dependent variable (D3MFT). The variables that presented statistical significance at the level of 20% or lower in the bivariate analysis were selected for multiple logistic regression analysis by the stepwise procedure. The Odds Ratios (OR) and the respective confidence intervals (CI) of 95% were estimated for the variables that remained in the multiple regression model at the level of 5%. All the statistical tests were performed with the SAS (SAS User's Guide: Statistics, version 9.2. Cary [NY]: SAS Institute Inc. 2001) software.
Results
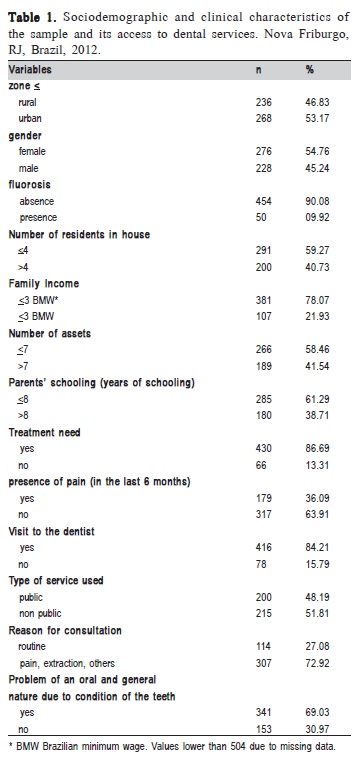
The sample comprised a distribution according to gender: male (45.24%) and female (54.76%) subjects. As regards socioeconomic variables, 78.07% of families had an income <3 Brazilian minimum wages and most parents/ guardians (61.29 %) had fewer than 8 years of schooling. With respect to dental needs and care, 86.69% of the adolescents needed treatment, and 36.09% had a history of dental pain in the last 6 months. The reasons for consultation of the majority of the subjects were due to pain, extraction, others (72.92%) and most of them alleged to have problems of an oral and general nature due to the condition of their teeth (69.03%). Fluorosis was detected in less than 10% of the individuals (Table 1).
The mean (standard deviation) of the D3MFT index was 1.90 (2.25), mainly represented by the decayed component (D=0.98/ds=1.67), followed by the filled (F=0.84/ds=1.46) and missing component (M=0.08/ds=0.42). A total of 201 (39.88%) children were found to be caries-free. The SCI index was 4.54 (1.90), with a mean (standard deviation) for the decayed, lost and filled components of 2.23 (2.30), 0.22 (0.71) and 2.09 (1.90), respectively. This specific caries polarization group showed low social indicators, such as income, with 80.75% (n=130) of the individuals with a family income lower than or equal to 3 minimum wages, and schooling, with 65.85% (n=108) of the parents/guardians with eight or fewer years of schooling, and almost all individuals needing dental treatment (95.21%; n=159).
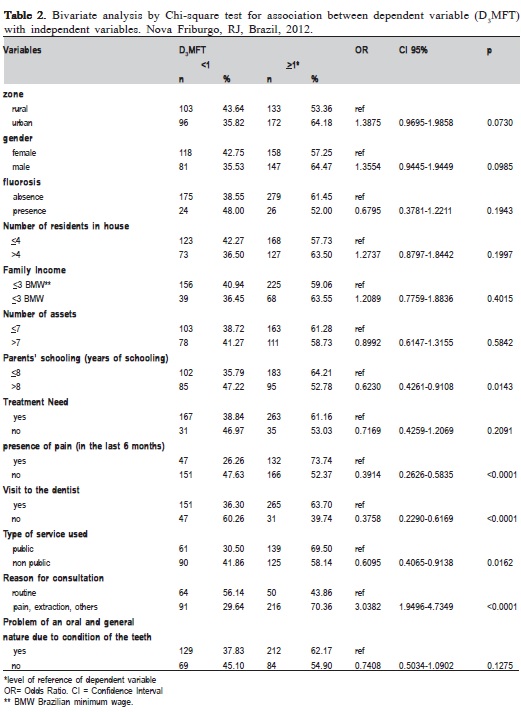
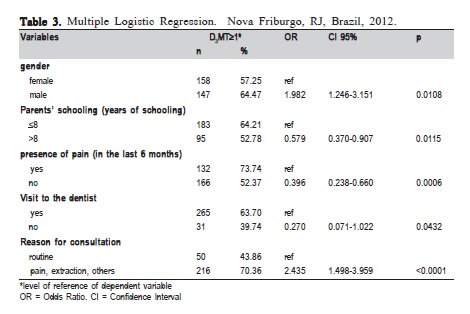
The bivariate analysis by the Chi-square test showed association between D3MFT and parents' schooling (OR=0.6230), presence of pain (OR=0.3914), visit to the dentist (OR=0.3758), type of service used (OR=0.6095) and reason for consultation (OR=3.0382) (Table 2). In the multiple logistic regression analysis, it was observed that the suggested protective factors associated with D3MFT<1 were: parents' schooling over 8 years (OR=0.579), absence of pain (OR=0.396) and not consulting the dentist (OR=0.270). Therefore, the children whose parents had a level of schooling of over 8 years presented less chance of having D3MFT>1. The possible risk factors associated with D3MFT>1 were: male gender (OR=1.982) and reason for consultation due to pain, extraction and others (OR=2.435); that is to say, male children presented 1.982 times more chance of having D3MFT>1 than the female children (Table 3).
Discussion
The evident decline in caries disease has not been homogeneous, that is, to say, the distribution of the disease is still unequal in the population, and remarkable regional differences are observed in the local and international epidemiological indices1,4-5. This factor represents evident inequalities in oral health, which range from differences in the prevalence of the disease, to access to services, products and protective measures in oral health.
A low prevalence of dental caries was found for the 12- year-old age group, with a mean of 1.90 for the D3MFT index, below the national mean value (D3MFT=2.07), but above the mean for the Southeastern region (D3MFT=1.72) and the goal established by the WHO for the year 2010 (DMFT<1)5,14. It may be observed that the percentage of caries-free individuals was around 39.88%, below both the national (44%) and State-wide (50.6%) means5. Moreover, the mean value of the SIC index at the value of 4.54 and mainly represented by the carious component, indicates polarization of the disease and is suggestive of correlation with social indicators such as income and schooling. In addition, the adolescents showed a considerable need for attention to oral health, by means of adequate measures of promotion, prevention and rehabilitation.
The age group caries indexes in Nova Friburgo still surpass those of other cities with fluoridated water. This may suggest some relation between the lack of access to this protective measure in the current panorama of dental caries in this city15-16. This epidemiological scenario in this municipality may be justified by the deficiency of an effective oral health surveillance policy and low coverage by the fluoridated public water supply in the municipality. This is in disagreement with the National Oral Health Policy itself, which prioritizes oral health promotion and preventive actions, including encouragement of healthy dietary habits, fluoridation of public water supply and distribution of dentifrices to the Brazilian population9.
From this point of view, the development of studies to evaluate the inequalities in oral health are a relevant research topic, in order to identify groups with greater vulnerability, because they directly or indirectly reflect the effects of the relevant determinants, such as precarious housing conditions, low income and access to education and health services, among others.
Variables such as family income and schooling have been considered good indicators of disease for this age group, since children belonging to families with differentiated income and education present different levels of the disease15,17.
In the present study, the schooling of the parents/ guardians was pointed out as a possible indicator for protection from the disease, and had a greater influence than the family income itself (Table 3). The results of previous researches have shown that the mother's schooling seems to be one of the main predictors of child's health; that is to say, a low level of schooling, especially the mother's, is related to greater risk for dental caries and to higher treatment needs in children13,18-19.
Social indicators such as schooling have usually been used to evaluate the advance and reversal in the population's living conditions. Generally, education provides access to better employment conditions, consequently generating a higher income level, which has a direct influence on the assimilation of positive behaviors related to oral health17,20.
Therefore, inequality in access to education appears to reflect directly on the oral health of the studied population, which leads to the need for of broader discussions and adoption of educational policy measures in a universal and uniform manner.
Conversely, non-use of dental services might also be regarded as a suggestive protection against the development of caries in the studied population, which generates questions about the quality of oral health care for individuals (Table 2). This fact may be related to the very practice of dentistry still being based on the surgical-restorative philosophy, in addition to inadequate diagnosis and consequent overtreatment of caries lesions, which generates an increase in the caries indices. This result is in agreement with the studies of Nadanovsky et al.21 (1995) and Traebert et al.19 (2011), which showed higher caries indices in the groups and populations who go to the dentist more frequently, or those who have never received any oral health care. In this sense, one perceives that there is a greater influence of population strategies in oral health, such as the mere use of fluoridated water and dentifrice, rather than the individual action of the dentist on the reduction of epidemiological dental caries indices7,22.
With regard to the other clinical variables, it seems to exist a direct relationship between the reasons for the consultation due to pain or extraction and DMF>1, which tends to demonstrate that individuals with symptoms related to more severe sequelae tend to have greater prevalence of the disease (Table 3)23.
The variable gender does not appear to be a relevant predictor for dental caries13,23. Nevertheless, the results of the present study are controversial, because they show the male gender to be at greater risk for caries than the female gender (Table 3), different from other studies which demonstrated a greater risk related to the female gender19,24. From these results, it is suggested that factors of an educational, or even cultural nature, may explain this variable, because there seems to be a consensus that the genders demonstrate different perspectives with regard to their self-care.
It should be pointed out that control of the entire research process with the establishment of a pilot stage, examiner calibration process, obtaining results with adequate reproducibility, control at the stage of data collection and analysis, indicate an adequate internal validity of the study. A clear limitation of this study is the fact that private schools adolescents, which represent 23.53% of the total of students in this age group, were not included in the study because most directors of private schools did not grant authorization to carry out the research at their facilities.
It was concluded that in spite of the prevalence of dental caries in the 12-year-old adolescents from Nova Friburgo being slightly below the national mean value, a clear polarization of the disease was observed. Education and no access to the dentist led to protection against the disease. These results may contribute to the development of oral health actions directed towards this target population for the control of caries.
The present study, which is the first one on oral health conducted in the city, was useful to identify dental caries in the adolescents and the respective factors that limit or favor the onset of caries in this age group. It may provide dentists, especially those from the public health system, with a general framework of the disease that will enable them to identify individuals at higher risk of caries and need for dental care. In view of these findings, it is possible to state that the University has a very important role to play in contributing to the production of epidemiological data which could favor the process of oral health planning by the municipality, with the development of programmed actions by means of adequate individual and population measures required for the control of disease. Furthermore, the study is relevant because this survey was concomitant with the beginning of water supply fluoridation in the city, which will form the basis for future epidemiological comparisons for the effect of this public oral health measure on the control of dental caries.
Acknowledgements
The authors wish to thank Karine Cortellazzi for performing the statistical analysis of data. They also thank FAPERJ for the financial support (Grants No. E-26/111.659/ 2010); and FAPERJ and CNPq for the Scientific Initiation Scholarship grants. They also give special thanks to the undergraduate students Fernanda Balonecker and Carla Lourenço, to the principals of the schools, teachers and all the children who contributed to the accomplishment of the survey.
References
1. Marthaler TM. Changes in dental caries 1953-2003. Caries Res. 2004; 38: 173-81. [ Links ]
2. Frazão P, Peres MA, Cury JA. Drinking water quality and fluoride concentration. Rev Saude Publica. 2011; 45: 964-73.
3. Santos APP, Nadanovsky P, Oliveira BH. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent Oral Epidemiol. 2013; 41: 1-12.
4. Brazil. Ministry of Health. Secretary of Health Care. Department of Primary Care. National Coordination of Oral Health. SB Brazil Project - Survey on Brazilian Population Oral Health Conditions 2002-2003: main results. Report. Brasília: Ministry of Health; 2004. 68p.
5. Brazil. Ministry of Health. Secretary of Health Care. Department of Primary Care. National Coordination of Oral Health. SB Brazil Project 2011: national survey of oral health: main results. Report. Brasília: Ministry of Health; 2011. 92p.
6. Ditmyer M, Dounis G, Mobley C, Schwarz E. Inequalities of caries experience in Nevada youth expressed by DMFT index vs. Significant Caries Index (SiC) over time. BMC Oral Health. 2011, 11: 12.
7. Sheiham A, Alexander D, Cohen L, Marinho V, Moyses S, Petersen PE, et al. Global oral health inequalities: task group—implementation and delivery of oral health strategies. Adv Dent Res. 2011; 23: 259-67.
8. Pattussi MP, Hardy R, Sheiham A. The potential impact of neighborhood empowerment on dental caries among adolescents. Community Dent Oral Epidemiol. 2006; 34; 344-50.
9. Brazil. Ministry of Health. Secretary of Health Care. Department of Primary Care. National Coordination of Oral Health. National Policy on Oral Health. Guidelines. Brasília: Ministry of Health; 2004. 16p .
10. Brazilian Institute of Geography and Statistics – IBGE. 2010 Census. Education and Displacement [accessed 2013 Apr 2]. Available from: http://www.ibge.gov.br/estadosat/ temas.php?sigla=rj&tema=censodemog2010_educ.
11. World Health Organization. Oral health survey: basic methods. 4. ed. Geneva: World Health Organization; 1997.
12. Bratthall D. Introducing the Significant Caries Index together with a proposal for a new oral health goal for 12-year-olds. Int Dent J. 2000; 50: 378-84.
13. Cortellazzi KL, Tagliaferro EPS, Assaf AV, Tafner APMF, Ambrosano GMB, Bittar TO, et al. Influence of socioeconomic, clinical and demographic variables on caries experience of preschool children in Piracicaba, SP. Rev Bras Epidemiol. 2009; 12: 1-11.
14. Hobdell MH, Myburgh NG, Kelman M, Hausen H. Setting global goals for oral health for the year 2010. Int Dent J. 2000; 50: 245-9.
15. Guerra LM, Pereira AC, Pereira SM, Meneghim MC. Assessment of socioeconomic variables in the prevalence of caries and fluorosis in municipalities with and without fluoridated water supplies. Rev Odontol UNESP. 2010; 39: 255-62.
16. Benazzi AST, Silva RP, Meneghim MC, Pereira AC, Ambrosano GMB. Trends in dental caries experience and fluorosis prevalence in 12-year-old Brazilian schoolchildren from two different towns. Braz J Oral Sci. 2012; 11: 62-6.
17. Freire MCM, Leles CR, Sardinha LMV, Paludetto Jr M, Malta DC, Peres MA. Dental pain and associated factors in Brazilian adolescents: the National School-Based Health Survey (PeNSE), Brazil, 2009. Cad Saude Publica. 2012; 28(Suppl): s133-45.
18. Lisboa CM, Paula JS, Ambrosano GMB, Pereira AC, Meneghim MC, Cortellazzi KL, et al. Socioeconomic and family influences on dental treatment needs among Brazilian underprivileged schoolchildren participating in a dental health program. BMC Oral Health. 2013, 13: 56.
19. Traebert J, Jinbo Y, Lacerda JT. Association between maternal schooling and caries prevalence: a cross-sectional study in Southern Brazil. Oral Health Prev Dent. 2011; 9: 47-52.
20. Machry R V, Tuchtenhagen S, Agostini B A, Teixeira C R S, Piovesan C, Mendes F M et al. Socioeconomic and psychosocial predictors of dental healthcare use among Brazilian preschool children. BMC Oral Health. 2013, 13: 60.
21. Nadanovsky P, Sheiham A. Relative contribution of dental services to the changes in caries levels of 12-year-old children in 18 industrialized countries in the 1970s and early 1980s. Community Dent Oral Epidemiol. 1995; 23: 331-9.
22. Antunes JL, Narvai PC. Dental health policies in Brazil and their impact on health inequalities. Rev Saude Publica. 2010; 44: 360-5.
23. Amaral RC, Batista MJ, Meirelles MPMR, Cypriano S, Souza MRL. Dental caries trends among preschool children in Indaiatuba, SP, Brazil. Braz J Oral Sci. 2014; 13: 1-5.
24. Ferraro M, Vieira AR. Explaining gender differences in caries: ( a multifactorial approach to a multifactorial disease. Int J Dent. 2010; 2010:649643. doi: 10.1155/2010/649643.
 Correspondence:
Correspondence:
Andréa Videira Assaf
Rua Sílvio Henrique Braune, n.22, Centro
CEP: 28625-650 Nova Friburgo- RJ-Brasil
E-mail: avassaf@gmail.com
Received for publication: April 05, 2014
Accepted: June 10, 2014
