










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.14 no.1 Piracicaba Jan./Mar. 2015
ORIGINAL ARTICLE
Comparison of two types of biomecanics for deep overbite correction
Ana de Lourdes Sá de Lira I; Yarasmin Nolêto de Sousa Alexandrino I
I Universidade Federal do Piauí – UFPI, Dental School, Department of Orthodontics, Teresina, PI, Brazil
ABSTRACT
Aim: To compare two types of treatment for Class II deep overbite malocclusion assessing maxillary and mandibular arches behavior in subjects submitted to full orthodontic treatment with standard edgewise appliance and those who used straight wire appliance. Methods: The sample consisted of 50 patients treated with full fixed appliances either with edgewise appliance (n=25, Group 1), or with straight wire appliance (n=25, Group 2). In both groups lateral cephalometric radiographs were compared with those done at the beginning of treatment and at its end, in order to quantify the cephalometric measures (8 linear and 6 angular) presenting the maxillary and mandibular arches behavior in the anteroposterior and vertical directions. All patients were treated without extraction or use of Class II intermaxillary elastics during the full orthodontic treatment. Results: In both groups the treatment of malocclusion contributed for mandibular forward displacement, reduction of deep overbite and overjet, reduction of mandibular plane with anti-clockwise rotation and labial projection of maxillary incisors. Conclusions: In both groups the sample showed favorable mandibular displacement, reduction of facial convexity, and profile improvement with anti-clockwise rotation. The correction of deep overbite was due to labial projection and intrusion of maxillary incisors.
Keywords: malocclusion; overbite; orthodontics.
Introduction
Deep overbite is a malocclusion with skeletal dental and neuromuscular implications characterized by the excessive vertical trespass of incisors1 . Excessive overlapping of the maxillary incisors over mandibular incisors is noted when values above of 40% by vertical trespass of upper incisors are observed2 . It can be found in Class I and Class II malocclusions, particularly in Class II division 2 malocclusion3 , and be associated with incisors' wear, palatal lesions and damaged esthetics4 , periodontal disease, functional deviations, inadequate mastication, occlusal trauma, teeth grinding and temporomandibular joint dysfunction5 .
Several etiologic factors have been associated with the occurrence of deep overbite6-7 and they may be of genetic or dentofacial development source origin2 , involving change of maxillomandibular growth, modification of labial and lingual functions and dentoalveolar alterations8 . Among these factors are overstated incisors eruption, excessive overjet, incisor mesiodistal width, incisor inclination, canine position, molars infraocclusion, molar cusp height, mandibular rami height and vertical facial type6 .
Deep bite has potentially harmful effects to mandibular development and may be associated to functional disturbances9 . The treatment allows favorable mandibular growth9-10 . If not treated, it may be observed mandibular displacement difficulty, faulty mandibular functional movement, masticatory cycle alteration, pronounced anterior guide, interference on protrusion and lateral movements, loss of vertical dimension, facial alterations and periodontal disease. It is considered the most harmful malocclusion to dental and alveolar tissues, causing modifications of masticatory function and in temporomandibular articulation, with implications in facial esthetics.
Maxillary incisor intrusion may be adequate to individuals who exhibit maxillary vertical excess, gum smile, lack of labial seal, short upper lip, increased inferior facial height and inclined occlusal plane10-12 . It is indicated to persons with good facial harmony, normal occlusal plane or a little inclined and with excessive Spee curve in the mandibular arch12 .
Posterior tooth extrusion is ideal for patients with hypodivergent facial pattern (short anterior facial height) redundant lips, excessive Spee curve, incisor exposition from moderate to minimal in the growth spurt phase. This procedure will provide inferior facial height increase, mandibular plane opening, facial convexity increase and reduction of inferior lip projection4,10-12 .
The evaluation of post-treatment results may reveal whether the treatment goals were achieved6 . For Nanda4 , the stability of deep bite treatment depends on specific dental correction (intrusion, extrusion or inclination), growth spurt and neuromuscular adaptation. The few studies that dealt with this subject indicate that active treatment is able to induce a moderate improvement of the overbite, but unfortunately the few studies assessing the effects of orthodontic treatment in deep bite patients either did not include untreated control subjects13-18 or used controls with normal overbite values19 .
Due to the scarcity of studies investigating skeletal and dental modifications caused by deep overbite treatment, two types of biomechanics with fixed appliances were searched. The objective of the present study was to compare two types of treatment for Class II deep overbite malocclusion assessing maxillary and mandibular arch behavior in individuals submitted to full orthodontic treatment with standard edgewise appliance or those who used straight wire appliance.
Material and methods
The UFPI's Ethics Committee approved the development of this study under the protocol number (CAAE 35309414800005209).
This clinical research was based on 50 Caucasian Brazilian individuals, 13 girls and 12 boys, who underwent full edgewise appliance (Group 1); and 15 girls and 10 boys that were treated using straight wire appliance (Group 2) during a 26-month period in the Post-Graduation Orthodontic Course of the Federal University of Piauí. All patients were treated in a single phase without extractions and no association of intermaxillary elastics. Each patient was evaluated two times by lateral cephalometric radiographs: at the beginning of the treatment (T0) and at the end of the active orthodontic treatment (T1).
All the subjects were in the pubertal growth spurt period at the beginning of the orthodontic treatment, with skeletal pattern of Class II evidenced by ANB angle>5o and Wits>0 mm, overbite in average between 5 - 5.5 mm (80% - 90%) and overjet between 3-3,5 mm. The skeletal maturity stage of all individuals was analyzed by hand and wrist radiographs. The dental relationship was Class II, according to Angle classification. The individuals also exhibited in average SN.GoGn angled 33o. In Group 1 the mean age for female patients at T0 was 11.8 (±0.61) years; at T1 it was 13.10 (±1.43) years. For male patients at T0 was 12.9 (±0.62) years; at T1 it was 14.11 (±1.42) years. In Group 2 the mean age for female patients at T0 it was 12.2 (±0.54) years; at T1 it was 14.4 (1.22) years. For male patients at T0 it was 12.9 (±0.56) years; at T1 it was 14.11 (±1.35) years.
The cephalograms were obtained by delimitating skeletal, dental and tegumentary structures. The measurements from cephalometric tracings regarding T0 and T1 were tabulated for statistical analysis, with angular measurements rounded up whenever decimal fraction existed.
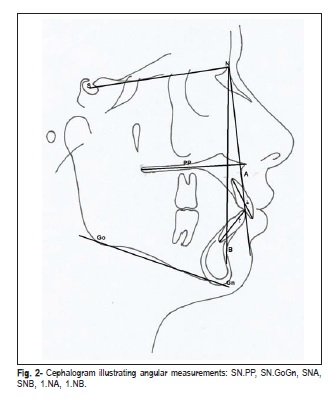
Eight linear and six angular measurements were obtained in the cephalometric tracing regarding T0 and T1 (Figures 1 and 2). To measure skeletal linear modifications a perpendicular line was traced from SN plane (skull base), passing by S point, and called S' line. A parallel line to SN plane was traced between S' and ENA point (S'- ENA) to describe the anterior maxillary displacement and between S' and Pog point (S'- Pog) to measure the horizontal mandibular displacement. The lengths of palatal plane linear and of mandibular plane in T0 and T1 were measured to examine probable maxillary and mandibular horizontal growth. To describe skeletal vertical changes the SN-Palatal Plane and SN-GoGn angles were evaluated. SNA and SNB angles were measured to analyze skeletal horizontal changes.
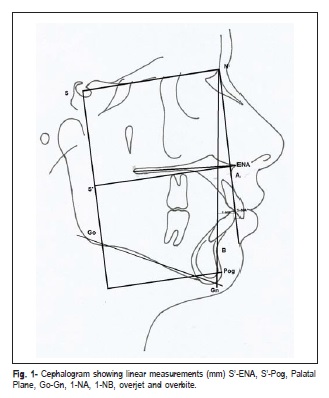
Initial and final overbite were obtained from the distance between incisal border of maxillary central incisor to mandibular central incisor. Overjet was measured from least distance of vestibular face of mandibular central incisor to palatal face of maxillary central incisor (Figure 1).
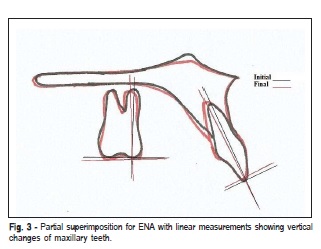
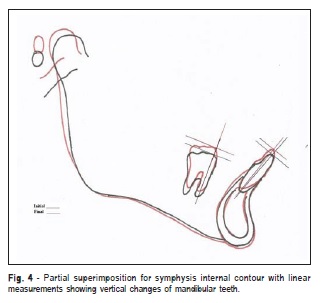
The incisor anteroposterior modifications were observated from linear measurements (1-NA, 1-NB and overjet) (Figure 1) and angular measurements (1.NA and 1.NB) (Figure 2). Vertical changes also were evaluated from linear measurements (Figures 1, 3 and 4).
In the molar tracings, vertical linear measurements were made to quantify the extrusion or intrusion on maxillary and mandibular partial superimpositions at T0 and T1 (Figures 3 and 4). A line was traced on the long axis of these teeth, at a 90º to another line tangent to the incisal border and molar oclusal border. The intersection between these lines was used as a reference point. The difference in vertical direction between initial (black tracing) and final (red tracing) positions of teeth on their tracings (Figures 3 and 4) was measured.
Total superimpositions of initial and final tracing from SN plane (sella-nasion) with register for S were made to analyze the growth direction, the orthodontic treatment and dental movements.
Means and standard deviations were calculated for each cephalometric measurement at T0 and T1. The statistical treatment of the data between T0 versus T1 was analyzed by using the paired Student's t test with 5% significance level. Unpaired t tests were used to evaluate the differences in therapeutic effects and the lengths of active treatment between both groups. The Pearson's r correlation coefficient was applied to determine whether any skeletal or dental characteristics and age were related to the appliance of active treatment.
Error of the methods
The error of the method was evaluated by 30 radiographs chosen at random, traced and digitized by the same investigator on two separate occasions at least two months apart. The Dahlberg20 formula was used: ME =\/Σ d2/2n, where n is the number of duplicate measurements. Random errors varied between 0.26 and 0.92 mm for linear measurements and between 0.28º and 1.1º for angular measurements.
Results
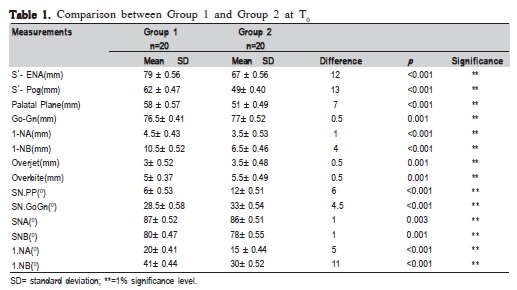
Both groups had comparable mean cephalometric values for linear measurements: S' -ENA, S'-Pog, Palatal Plane, 1- NA, 1-NB, overjet and overbite and angular measurements: SNPP, SNGoGn, SNA, SNB, 1-NA and 1-NB.
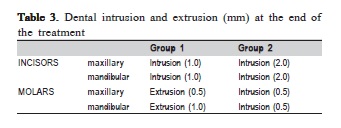
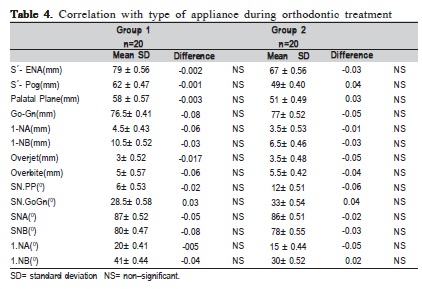
Comparison between Group 1 and Group 2 at T0 is shown in Table 1. Treatment effects on cephalometric values and differences between the two groups may be seen in Table 2. Dental intrusion and extrusion (mm) at the end of treatment is shown in Table 3. The correlation with type of appliance during orthodontic treatment in both groups is presented in Table 4.
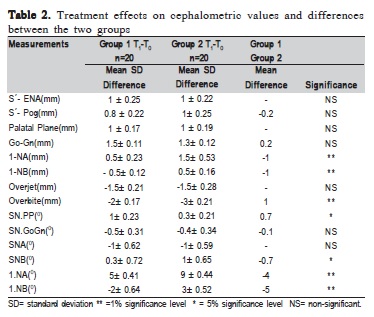
In both groups was observed anterior mandibular displacement, reduction of deep overbite and overjet, reduction of mandibular plane with anti-clockwise rotation and labial projection of maxillary incisors. In Group 1, significant vertical displacement contributed to reduce the overbite.
Discussion
In this study the cephalometric evaluation demonstrated that in both groups there was skeletal Class II with mandibular retraction, deep overbite and favorable vector of facial growth (Table 1).
The group tracings were compared in relation to the skull base (SN) and it was diagnosed that the Group 1 showed brachiocephalic pattern, lower mandibular plane (SN.GoGn) and both maxillary and mandibular arches were more advanced (S'-ENA e S'-Pog) than Group 2. In this group the mesocephalic pattern prevailed (SN.PP, SN.GoGn), with more mandibular retrognathism (S'-Pog, SNB and overjet) than Group 1. Overbite also was more pronounced, probably due to retroinclination of maxillary and mandibular incisors (Table 1).
The main strategy of deep bite treatment for both groups consisted of combined extrusion of the posterior teeth, intrusion and vestibular inclination of the anterior teeth (maxillary and mandibular incisors). This is confirmed in the literature because the decision of extrusion or intrusion should be based on skeletal pattern, vertical pattern, facial esthetic, growth spurt, occlusal plane, severity of final malocclusion, occlusion stability or the combination of these factors1,4-7,10,13-19 .
At first in Group 1 segmented arches (Rickets' technique) 0.018´x 0.025´ were used for intrusion and projection of maxillary and mandibular incisors, enabling the decrease of deep overbite, with anterior brackets glued in the most possible incisal level. In Group 2 continuous arches of nickel and titanium 0.014´ e 0.016´ with pronounced Spee curve in the maxillary arch and reverse curve in the mandibular arch were utilized for little molar intrusion, labial projection and incisor intrusion in deep overbite correction. Since they are flexible, their sockets are complete in all teeth from the beginning of the treatment, as observed by Burstone7 and Chen et al.10 .
After this, in Groups 1 and 2 continuous arches of leveling were sequentially used to maintain Spee curve alterations and obtain the best possible mandibular displacement in downward and forward directions during growth spurt. This approach is corroborated by Martinelli et al.19 , who reported that the favorable mandibular displacement enables achieving the best harmonious profile, and by Woods18 who affirmed that the extrusive movement of only 1 mm of maxillary and mandibular molars reduces effectively the overbite between 1.5 to 2.5 mm.
In Group 1, based on total cephalometric superimposition, skeletal pattern and facial profile maintained the same proportions with maxillary and mandibular residual growth vector to the down and forward directions, associated with the orthodontic mechanics of extrusion to maxillary and mandibular molars during deep bite correction (Tables 1-3), (Figure 5).
The reduction of SNA angle with retraction of A point probably resulted from maxillary incisors projection. In spite of residual growth with anterior displacement and anticlockwise rotation of the mandible, there was little reduction of SNB angle, probably due the forward nasion displacement (Table 2), (Figure 5).
The deep overbite correction occurred because there were intrusion and labial inclination of maxillary incisors and extrusion of maxillary and mandibular molars. The overjet decreased demonstrating late growth of the mandible, in spite of the labial inclination of maxillary incisors and the uprighting of mandibular incisors (Tables 2 and 3).
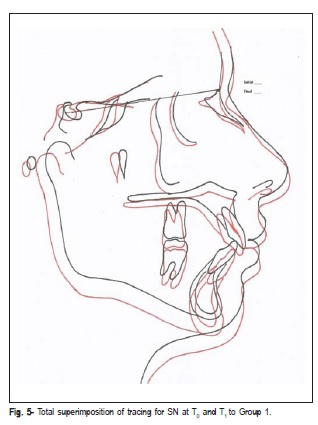
The correction of overbite may be supported because the molar extrusions and the mandibular displacement forward and downward occurred harmoniously, although the mean value of SN.GoGn reduction was 0.5 degree (Tables 2 and 3). The anti-clockwise rotation during puberal growth spurt, representative of brachiocephalic pattern, was not observed probably due the molar extrusions, corroborating with the studies of some authors13-19 .
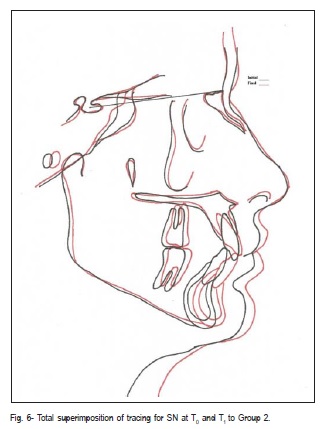
The total cephalometric superimposition between T0 and T1 of Group 2 showed forward displacement and anticlockwise rotation of the mandible, together with profile improvement. This was confirmed by increased SNB angle and linear measurements S'–Pog and Go-Gn, as well as decreased SN.GoGn angle and overjet. The reduction of SNA angle probably happened due to A point backward displacement with labial inclination of maxillary incisors (Table 2 and Figure 6).
The deep overbite correction occurred basically with labial projection and intrusion of maxillary and mandibular incisors. The intrusion of maxillary molars was necessary to correct the reverse Spee curve. Nevertheless, in the mandibular arch molar intrusion was observed to decrease the Spee curve, contributing for an average 0.4 º decrease of SN.GoGn and anti-clockwise rotation of the mandible (Tables 2 and 3) (Figure 6). These data were corroborated by Baccetti et al.15 and Martinelli et al.19 , who reported that the overbite correction resulted of the intrusion of maxillary incisors as well as mandibular incisors accompanied by mandibular growth.
Similar results were found by Quintao et al.17 and Woods18 who investigated the dental movement during deep overbite correction of 87 subjects with Class II division 1 malocclusion and they concluded that the correction basically occurred by intrusion and labial projection of mandibular incisors.
There were no outcome differences between the two groups during the treatment of Class II deep overbite malocclusion in relation to the orthodontic technique applied (Table 4). Similar results were found by Ghafari et al.2 , who compared intrusive mechanics by segmented arches with the treatment using continuous arches of nickel and titanium and observed real intrusion of maxillary and mandibular incisors.
Woods18 evaluated initial and final cephalograms of patients Class II division 1 and division 2 at the end of mixed dentition to determine if skeletal and dentoalveolar alterations with deep overbite were influenced by direction of mandibular growth during the treatment. He concluded that in patients with brachiocephalic and mesiocephalic patterns the point B moved significantly more forward than in dolicocephalic patients. Similar outcomes also were found in this study.
In conclusion, deep overbite correction in Group 1 was supported especially by incisors intrusion and molars extrusion, associated with mandibular displacement, due to growth spurt with anti-clockwise rotation. In Group 2 the incisors' intrusion and labial projection of maxillary incisors provided the deep overbite correction. Meanwhile the molars intrusion to correct Spee curve promoted mandibular forward displacement with anti-clockwise rotation. In both groups the treatment showed reduction of facial convexity and improvement in profile.
References
1. Baccetti T, Franchi L, McNamara JA Jr. Longitudinal growth changes in subjects with deepbite. Am J Orthod Dentofacial Orthop. 2011; 140: 202-9. [ Links ]
2. Ghafari JG, Macari AT, Haddad RV. Deep Bite: Treatment options and challenges. Seminars Orthodontics. 2013; 19: 253-66.
3. Lindauer SJ, Lewis SM, Shroff B. Overbite correction and smile aesthetics. Semin.Orthod. 2005; 11: 62-6.
4. Nanda SK. Growth patterns in subjects with long and short faces. Am J Orthod Dentofacial Orthop. 1990; 98: 247-58.
5. Schutz-Fransson U, Bjerklin K, Lindsten R. Long-term follow-up of orthodontically treated deep bite patients. Eur J Orthod. 2006; 28: 503-12.
6. Parker CD, Nanda RS, Currier GF. Skeletal and dental changes associated with the treatment of deep bite malocclusion. Am J Orthod Dentofacial Orthop. 1995; 107: 382-93.
7. Burstone CJ. Biomechanics of Deep Overbite Correction. Seminars Orthodontics. 2001; 7: 26-33.
8. Franchi L, Baccetti T, Giuntini V, Masucci C, Vangelist A, Defraia E. Outcomes of two-phase orthodontic treatment of deep bite malocclusions. Angle Orthod. 2011; 81: 941-52.
9. McDowell EH, Baker IM. The skeletodental adaptations in deep bite correction. Am J Orthod Dentofacial Orthop. 1991; 100: 370-5.
10. 10 Chen YJ, Yao CCJ, Chang HF. Nonsurgical correction of skeletal deep overbite and Class II Division 2 malocclusion in an adult patient. Am J Orthod Dentofacial Orthop. 2004; 126: 371-8.
11. Lira ALS, Souza MMG, Bolognese AM. Long-term maxillary behavior in treated skeletal Class II malocclusion. Braz J Oral Sci. 2012; 11: 120-4.
12. Lira ALS, Souza MMG, Bolognese AM, Nojima M. Comparison of 2 types of treatment of skeletal Class II malocclusion: a 5-years postretention analysis. Braz J Oral Sci. 2014; 13: 251-6.
13. Martinelli FL, Ruellas AC, Lima EM, Bolognese AM. Natural changes of maxillary first molars in adolescent with esqueletal Class II malocclusion. Am J Orthod Dentofacial Orthop. 2010; 137: 775-81.
14. Engel G, Cornforth G, Damerell JM, Gordon J, Levy P, McAlpine J et al. Treatment of deep bite cases. Am J Orthod. 1980; 77: 1-13.
15. Baccetti T, Franchi L, Giuntini V, Masucci C, Vangelisti A, Defraia E. Early vs late orthodontic treatment of deep bite: a prospective clinical trial in growing subjects. Am J Orthod Dentofacial Orthop. 2012; 142: 75-82.
16. Millett DT, Cunningham SJ, O'Brien KD, Benson PE, Oliveira CM. Treatment and stability of Class II division 2 malocclusion in children and adolescents: a systematic review. Am J Orthod Dentofacial Orthop. 2012; 142: 159-69.
17. Quintao CCA, Miguel JAM, Brunharo IP, Zanardi G, Feu D. Is traditional treatment a good option for na adult with a Class II deepbite malocclusion. Am J Orthod Dentofacial Orthop. 2012; 141: 105-12.
18. Woods MG. Sagittal mandibular changes with overbite correction in subjects with different mandibular growth directions: Late mixed-dentition treatment effects. Am J Orthod Dentofacial Orthop. 2008; 133: 388-94.
19. Martinelli FL, Reale CS, Bolognese AM. Class II malocclusion with deep overbite: A sequential approach. Dental Press J Orthod. 2012; 17:76-82.
20. Dahlberg G. Statistical methods for medical and biological students. London: Allen & Unwin; 1940..
 Correspondence:
Correspondence:
Ana de Lourdes Sá de Lira
Universidade Federal do Piauí, Faculdade de
Odontologia, Departamento de Ortodontia.
Rua Senador Joaquim Pires, 2076 -Ininga-
CEP: 64049-590 Teresina- PI- Brasil
E-mail: anadelourdessl@hotmail.com
Received for publication: January 23, 2015
Accepted: March 23, 2015
