










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.14 no.2 Piracicaba Abr./Jun. 2015
ORIGINAL ARTICLE
Periodontal status and treatment need among adolescents in Ibadan, Southwestern Nigeria
Bamidele Olubukola PopoolaI; Elizabeth Bosede DosumuII; Joy Ucheonye IfesanyaI
I University of Ibadan, College of Medicine, Faculty of Dentistry, Department of Child Oral Health, Ibadan, Oyo, Nigeria
II University of Ibadan, College of Medicine, Faculty of Dentistry, Department of Periodontology and Community Dentistry, Ibadan, Oyo, Nigeria
Abstract
A previous Nigerian study had reported high incidence of periodontal disease in young Nigerians though global studies show the contrary. Aim: To determine the periodontal status and treatment needs of adolescents attending private and public secondary schools in Ibadan, south-western Nigeria. Methods: One thousand, five hundred and twenty two secondary school children in Ibadan were assessed. Sociodemographic data was obtained using a data extraction form. Intraoral examination was performed on all participants. Oral cleanliness was assessed using the plaque index of Silness and Loe, while periodontal health status and treatment needs were assessed using the Community Periodontal Index of Treatment Needs (CPITN). Data were analyzed with the Statistical Package for Social Sciences (SPSS) version 22. Statistical significance was set at p<0.05. Results: Only eight participants (0.5%) had healthy component of periodontal status. The mean plaque index was 1.12±0.41. The CPITN scores varied significantly with the gender of participants (p<0.001). Number of sextants affected by periodontal diseases varied significantly with the socioeconomic status (p=0.02). Conclusions: Gingival ill-health is prevalent among adolescent Nigerians with a great need for oral hygiene instructions and professional cleaning. There is need for oral health education among this sub-population of Nigerian children and provision of mobile dental clinics to help meet their treatment needs.
Keywords: periodontium; adolescent health; treatment outcome; student.
Introduction
Periodontal disease is a spectrum of health anomalies affecting the surrounding structures of the teeth including the gums, periodontal ligament and alveolar bone. These anomalies may be restricted to the gingiva (gingivitis) or may extend to the periodontal ligament space and alveolar bone (periodontitis). Periodontitis may lead to tooth mobility, pathologic migration and eventual loss of teeth. The clinical signs of periodontal disease may appear at any age1 and epidemiological studies indicate that gingivitis, which varies in severity, is almost a universal finding in children and adolescents, while destructive periodontitis is of lower prevalence in younger individuals when compared with adults2. A Nigerian study has reported a relatively high occurrence of deep pockets in young Nigerians3. However, whether these pockets are true (pockets greater than 6 mm deep) or false pockets (less than or equal to 6 mm) was not specified.
The first step in proper planning for oral health among young children is to establish the prevalent oral health problem, which in this case is the periodontal health condition. This will help to promote evidence-based intervention programs4. The Community Periodontal Index for Treatment Needs is thus a valuable tool in assessment for health policy making and strategic planning for oral health implementation programs5 and this is true even among children.
Epidemiological trends have shown waxing and waning in both oral cleanliness and occurrence of gingivitis in children and adolescents. Deterioration appears to be more evident when the age range of subjects studied is wide6. An earlier Nigerian study in Ile-Ife reported a prevalence of periodontal diseases of 84.2% among 3-20-year olds3, while a more recent study in Benin City revealed a prevalence rate of 99.2% among 5-19-year old7. Both studies reported a high occurrence of gingivitis and heavy deposits of calculus but little evidence of damage to the periodontal tissues. However, these studies used the gingival index of Loe and Silness, plaque index of Silness and Loe and the oral hygiene index of Greene and Vermilion in their assessment. In a study among institutionalized mentally handicapped Nigerian children using the CPITN8, a high level of gingivitis and periodontal diseases was reported, with 92.9% of assessed sextants involved in periodontal tissue changes. A similar finding was reported in a similar population of Iranian children9. A study comparing public and private school children found that presence of calculus and gingivitis was less in private school children10. This suggests that oral hygiene was better when socio-economic status was high, as it has been previously reported11.
Another study has reported that only 17.8% of 11-14 years old Nigerian children had good oral hygiene, while about 50.4% had fair oral hygiene12. This study corroborated the gender difference in oral cleanliness reported by previous studies7,10, with female children exhibiting better hygiene status than males. It has also been reported that severity of gingivitis lessens as age increases13.
This study aimed to describe the pattern of periodontal health status of secondary school adolescents in private and public institutions in Ibadan as well as their treatment needs.
Material and methods
In this study, children aged 11 to 16 years old from secondary schools in Ibadan, Nigeria were examined for periodontal diseases.
Sample size was determined using the formula for determining the sample for cross-sectional studies assessing qualitative variables as shown below:
N= Zα 2 p(1-p)/d2
Where:
N= minimum sample size
Zα= standard normal variety at p<0.05 =1.96
p= prevalence of periodontal diseases among children in this environment from a previous study =71% =0.71
1-p= 29% =0.29
d= minimum acceptable error=5%.
1.962x0.71x0.29/0.052
N=316.
The participants for the study were selected from public and private secondary schools in five local government areas in Ibadan metropolis. The list of all public and private secondary schools in these local government areas was obtained from Oyo State Ministry of Education and 20 schools were selected using proportionate sampling method. Ethical clearance for this study was obtained from Oyo State Ministry of Health and permission to visit the schools was obtained from the principals of the various schools. These schools have on average 3 branches per class with approximately 30 students in each class. At each school, total population samples of students who gave assent and whose parents consented to their participation in the study were collated. Random selection from the classes by simple random technique using ballot process was used to obtain the study participants.
Demographic data for each participant were obtained and socioeconomic status assessed according to the criteria of Oyedeji14 (1985). Oral examinations were conducted by the field team that included two dentists (PBO & IJU). Intra oral examinations were done under natural light outdoors with sterile mouth mirrors and WHO CPITN probe. Examination for periodontal disease was carried out using the Community Periodontal Index for Treatment Needs as instituted by Ainamo et al.15 (1982). The index teeth in each sextant were examined by running the CPITN probe around the entire sulcus of each tooth and the highest score recorded. The participants were categorized as:
Score 0= healthy periodontium
Score 1= Gingival bleeding after gentle probing
Score 2=supra or sub-gingival calculus
Score 3=pathologic pockets 4-5.99 mm deep
Score 4= pathologic pocket 6 mm and above.
Treatment needs were classified according to the highest score recorded in all assessed sextants.
TN 0=No need for treatment
TN 1=Need for oral hygiene instructions
TN 2=Need for oral hygiene instructions and professional cleaning
TN 3=Need for complex treatment.
Oral cleanliness was assessed using the plaque index of Sillness and Loe16.
Calibration of the two examiners was done by repeat examination of 20 children on two occasions. The results were subjected to Cohen's Kappa statistics and intra class correlation coefficient for inter and intra-examiner reliability; values were 0.8 and 0.8 respectively. Data obtained were analyzed using the Statistical Package for Social Sciences (SPSS) Version 22. Descriptive statistics was used to summarize the variables in the data set. Qualitative variables were assessed using the Chi Square test, while the independent sample Student t-test and ANOVA were employed to test association involving descriptive data in two or more groups. Level of significance was set at p<0.05.
Results
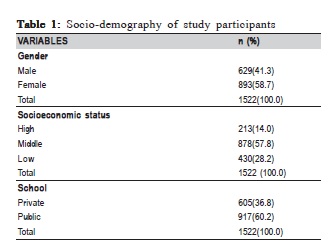
A total of 1522 secondary school children were seen. Mean age was 13.5±1.1years. Other socio-demographic variables are as shown in Table 1.
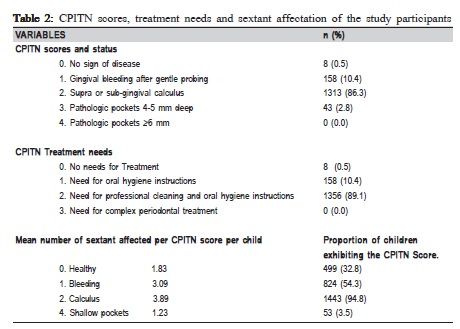
None of the children had a missing or edentulous sextant. Of the 9132 sextants assessed, 8219 (90.0%) were involved in periodontal tissue changes. Only eight children (0.5%) had no sign of periodontal disease as assessed with the CPITN. Periodontal health status and treatment needs as well as the mean number of sextants affected by periodontal diseases in the children assessed are as shown in Table 2.
The mean plaque index was 1.12±0.41. The males had higher plaque scores than females (p<0.001). The CPITN scores varied significantly with oral cleanliness as assessed by the plaque index (p<0.001). Though younger adolescents (age 11 to 13) had worse plaque scores than older adolescents (14 to 17 years old), there was no significant difference in the plaque scores on the basis of age (p=0.06). The CPITN scores did not vary significantly with the age group (p=0.12), socioeconomic status (p=0.12), nor with the type of school attended by the children (p=0.37). In contrast, CPITN scores varied significantly with the gender p<0.001. While more males had CPITN scores 0 and 1, more females had scores 2 and 3 (Table 3).
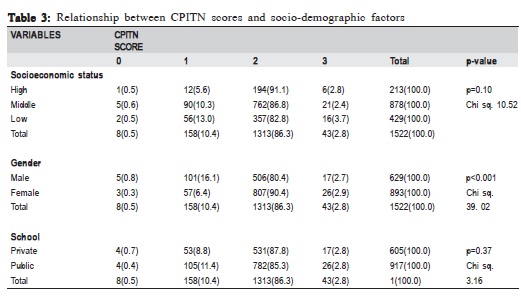
The number of sextants affected by periodontal diseases increased as the socioeconomic status of the children worsened (p=0.02). Though females had more sextants affected by periodontal diseases than males, this relationship was not statistically significant (p=0.05).
Discussion
This study has observed a high prevalence of adverse periodontal tissue changes among Nigerian adolescents with about 90% of the sextants assessed involved in various stages of periodontal ill health. This figure slightly improves on but is similar to that reported by Denloye8 among mentally handicapped children. The present finding is an improvement because our participants have better musculoskeletal capability than the handicapped children. According to the WHO stipulated goal for periodontal health among children aged 15 years as at the year 2010, 100% of 15-year-olds should have at least five healthy sextants5. However, findings from this study demonstrated that less than one third of the studied population had less than two healthy sextants. This finding falls severely short of the global goal for periodontal health and implies that there is still a great periodontal health need among these children. The study also found that the plaque score was higher among children with CPITN scores 1, 2 and 3. This is similar to the observation in an Iranian study among 15-19-year olds5, and further asserts the relationship between plaque and gingival health17.
Contrary to a previous study18, this study observed that there was no significant association between periodontal tissues status and the type of school attended or to the socioeconomic status of the children. However, we did find that children of lower socioeconomic class had more diseased sextants than those from higher social class. This suggests a need for a firmer surveillance system that will enable proper measurement of both the extent of spread and control of oral health conditions as well as impact of oral health promotion strategies19.
The prevalence of periodontal disease in the studied group is high and is accounted for largely by gingival bleeding, presence of calculus and shallow pockets. This is similar to previous findings in this environment based on other assessment criteria3,7,12 and has been attributed to the combined effect of dental cleaning ability as reflected by the association between gingival health scores and plaque scores5. Change in bacterial composition of the dental plaque, inflammatory cell response and the hormones of puberty are other factors which may be responsible for this poor gingival health20.
This study also found no difference between periodontal health and socio-economic status of all the children assessed. This is contrary to a previous report that has documented worsened periodontal status in children of lower socioeconomic strata10,21.
However, since the present study also found that children in the lower socioeconomic class had more sextants affected by periodontal pathologic changes, the absence of an association between the previous variables may not be the true status of association. This occurred because the methods of classifying socioeconomic strata in the previous studies were not specified. On the other hand, the observed lack of association may be a pointer to the emergence of an alarming trend where high social class parents are beginning to ignore their children's oral health care.
In congruence with previous studies12,21, the females had better oral cleanliness than males. We also found a significant relationship between gender and gingival health in the present study as in previous documentations7,12,10,21. However in this study, more boys had healthy gingival status and CPITN score 1 than the girls, who had more calculus accumulations and shallow pockets. Considering that the girls cleaned better that their male counterparts, the effect of the puberty hormones especially oestrogen and progesterone which are responsible for most of the modulator actions seen in hormone based gingivitis22-23 may be responsible for this finding. Especially since these hormonesare found in higher concentration in females.
In conclusion, gingival ill-health is prevalent among adolescent Nigerians resident in Ibadan Oyo state with a great need for oral hygiene instructions and professional cleaning. There is need for oral health education among this sub-population of children and provision of mobile dental clinics to help meet their treatment needs.
References
1. Mârþu S, Solomon S, Potârnichie O, Ãrin LPÃS, Mârþu A, Nicolaiciuc O, et al. Evaluation of the prevalence of the periodontal disease versus systemic and local risk factors. Int J Med Dent. 2013; 3: 212-8. [ Links ]
2. Chauhan VS, Chauhan RS, Devkar N, Vibhute A, More S. Gingival and Periodontal Diseases in Children and Adolescents. J Dent Allied Sci. 2012; 1: 26-9.
3. Akpata ES. Oral health in Nigeria. Int Dent J. 2004; 54: 361-6.
4. Folayan MO, Adeniyi AA, Chukwumah NM, Onyejaka N, Esan AO, Sofola OO, et al. Programme guidelines for promoting good oral health for children in Nigeria: a position paper. BMC Oral Health [Internet]. 2014 Jan [cited 2015 Feb 26]; 14: 128.
5. Sane A-S, Nikhbakht-Nasrabadi A. Periodontal health status and treatment needs in iranian adolescent population. Arch Iran Med. 2005; 8: 290-4.
6. Hatem AE. Epidemiology and risk factors of periodontal disease. In: Manakil DJ, editor. Periodontal disease- a clinician's guide. InTech; 2012. p.213-30.
7. Odai CD, Azodo CC, Braimoh OM, Obuekwe ON. Oral health profile of primary and post primary school children at a health facility in Uselu, Benin city. Benin J Postgrad Med. 2009; 11: 34-9.
8. Denloye OO. Periodontal status and treatment needs of 12-15 year old institutionalized mentally handicapped school children in Ibadan , Nigeria. Odontostomatol Trop Trop. 1999; 86: 8-10.
9. Nematollahi H, Makareem A, Noghani AR. Periodontal treatment needs amongst 9-14 year old institutionalized mentally retarded children in Mashhad, Iran. Shiraz Univ Dent J. 2010; 10: 15-20.
10. Adenubi JO. The gingival health of eight year old Nigerian children. J Public Health Dent. 1984; 44: 67-72.
11. Khan MA, Khan D, Qureshi ZUR. Dental ailments among low and high socioeconomic status school children aged 11-12 years. Pakistan Oral Dent J. 2011; 31: 388-91.
12. Kolawole KA, Oziegbe EO, Bamise CT. Oral hygiene measures and the periodontal status of school children. Int J Dent Hyg. 2011; 9: 143-8.
13. Pauraite J, Milciuviene S, Sakalauskiene J. The prevalence of gingivitis among 4-16 year old schoolchildren in Kaunas. Stomatol Balt Dent maxillofac J. 2003; 5: 97-100.
14. Oyedeji GA. Socioeconomic and cultural background of hospitalised children in Ilesha. Nig Paed J. 1985; 12: 111-7.
15. Ainamo J, Barnes D, Beaagrie G, Cutress T Martin J, Sardo-Infirri J. Development of the World Health Organization (WHO) Community Periodontal Index of Treatment Needs. Int Dent J. 1982; 32: 281-91.
16. Silness J, Loe H. Periodontal disease in pregnancy II: corelation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964; 22: 121-35.
17. Fukuda H, Ogada CN, Kihara E, Wagaiyu EG, Hayashi Y. Oral Health Status among 12-Year-Old Children in a Rural Kenyan Community. J Dent Oral Heal. 2014; 2: 1-5.
18. Awad F, Idris I. Periodontal disease prevalence and some related factors among 15 years old school children in Khartoum State, Sudan. Sudan J Public Health. 2010; 5: 187-92.
19. Petersen PE, Ogawa H. Strengthening the prevention of periodontal disease: the WHO approach. J Periodontol. 2005; 76: 2187-93.
20. Borrell LN, Papapanou PN. Analytical epidemiology of periodontitis. J Clin Periodontol. 2005; 32: 132-58.
21. Agbelusi GA, Jeboda SO. Oral health status of 12 year old Nigerian children. West Afr J Med. 2006; 25: 195-8.
22. Güncü GN, Tözüm TF, Ça"layan F. Effects of endogenous sex hormones on the periodontium – Review of literature. Aust Dent J. 2005; 50: 138-45.
23. Bhardwaj A, Bhardwaj SV. Effect of Androgens , Estrogens and Progesterone on Periodontal Tissues. J Orofac Res. 2012; 3: 165-70.
 Correspondence:
Correspondence:
Bamidele O. Popoola
Department of Child Oral Health
Faculty of Dentistry
University College hospital and University of Ibadan
ZIP CODE: 200009, Ibadan, Oyo, Nigeria
E-mail: olubukolap@gmail.com
Received for publication: March 02, 2015
Accepted: May 28, 2015
