










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.14 no.3 Piracicaba Jul./Set. 2015
ORIGINAL ARTICLE
Failure of prosthetic screws on 971 implants
Carolina Schäffer MorschI; Caroline Freitas RafaelI; Juan Felipe Montero DumesI; Gabriella Mercedez Peñarrieta JuanitoI; João Gustavo Oliveira de SouzaI; Marco Aurélio BianchiniI
I Universidade Federal de Santa Catarina – UFSC, Department of Dentistry, Area of Implantolology, Florianópolis, SC, Brazil
ABSTRACT
Aim: To evaluate the presence of failures in prosthetic screws and whether these failures are related to the type of prosthesis, abutment angulation and presence or not of intermediate. Methods: Two-hundred and sixty-seven patients were evaluated at the Federal University of Santa Catarina, totaling 971 external hexagonal implants in place for at least one year. A Tobit regression model for censored variables was used and the explanatory variables were subjected to percentage analysis. Results: The results demonstrated a relationship between the failure in prosthetic screws and the investigated factors with a significance of F=0.003 and p<0.05. The percentage analysis showed that the prosthetic screw failed in 8.82% of 238 unitary prostheses and 10.1% of 773 multiple prostheses. Among 912 abutments, 9.43% failed and in the 59 angled abutments, failures appeared in 15.25%. A total of 200 prostheses were placed over the implant platform and 13% failed. A total of 771 prostheses were made over abutment and 8.95% of these screws failed. Conclusions: Through multiple linear regression it could be concluded that the type of prosthesis showed no significant influence on the prosthetic screw failure, but other variables were related to this mechanical failure. There was a significant relationship among the variables, demonstrating the need for greater attention in choosing the type of prosthesis, the abutment angulation and whether the prosthesis will be placed directly on the implant platform or on the abutment.
Keywords: dental implant-abutment design; /complications; prosthesis failure; dental prosthesis, implant-supported.
Introduction
It is evident that due to the high survival rates that the implant-supported prostheses are fully accepted today as a reliable treatment option for the replacement of single or multiple missing teeth1. However, some complications are mentioned in several studies including screw loosening and screw, veneer, abutment, framework and implant fractures, and fracture of the luting cement2. Screw loosening is recognized as one of the most evident complications3, like fractures of the veneering material4. The reasons for screw loosening include fatigue, inadequate tightening torque, inadequate prosthesis fit, poorly machined components, vibrating micro-movement and excessive loading2,5. External hexagon connection systems have been considered more prone to screw loosening as a result of their mechanical properties under dynamic load. To reduce some of these complications, internal connection systems were developed to improve the biomechanical properties of implant-abutment joints and have shown significant biomechanical advantages over external-hex connection2.
The biomechanical behavior of implant-retained restorations, including the screw, may be compromised by some factors6, such as type of prosthesis, the abutment angulation and if the prostheses are placed directly on the implant platform or on the abutment. Regarding the type of prosthesis, it is known that a single prosthesis allows for higher patient satisfaction and also facilitates hygiene; however it presents more possibilities of screw loosening7. Concerning the abutment angulation, when a compensating strategy is required this abutment may be used where aesthetics and quantity of soft tissue allow. However, this abutment can present more screw failures due to the small thread area that often loses retention and produces cracks due to the low amount of metal.
Placing a prosthesis connected directly to the implant has advantages, including low cost, possibility to overcome problems such as limited interocclusal spaces and the possibility of correction of implant angulation error. However, this abutment requires laboratory steps that may cause implant/abutment misfit, which may result in screw loosening and/or fracture6.
The aim of this research was to investigate if there is a relationship between the screw failure and the type of prosthesis, the abutment angulation and the presence or not of intermediate.
Material and methods
The present study was approved by the research ethics committee of the Federal University of Santa Catarina (UFSC, Florianópolis, SC, Brazil) under number 367.077. All the participants were briefed about the purpose and process of the study and patient's written consent was obtained. Data was obtained from a 10-year retrospective study. The researcher was calibrated. A total of 297 patients with implantsupported prostheses, 1001 implants in total, were invited to attend the dentistry department with the purpose of being evaluated. The patients were rehabilitated with external hexagon connection dental implants and with prosthesis in function for at least 1 year. The screw torque ranged from 10 to 32 Ncm according to the manufacturer's instructions and the type of abutment. The cemented restorations were cemented with zinc phosphate cement (Vigodent Coltene, Rio de Janeiro, RJ, Brazil).
The inclusion criterion was patients with implant reconstruction in function for at least 1 year that attended the recall visits. Patients rehabilitated with internal hexagon connection implants and morse tapper, as well as implants supporting overdentures were excluded from the sample. Out of 297 patients evaluated, 267 were selected according to the inclusion and exclusion criteria, totaling 971 implants.
All the patients were enrolled in a follow-up program. This provided the opportunity to check the patient every 6 months in the first year and then annually. The following explanatory variables were assessed:
- Amount of implants
- Time in function
- Prosthesis type (single or multiple)
- Presence or absence of the intermediate
- Straight or angulated abutment
- Screw failure (fracture or loosening)
Statistical Analysis:
The collected data were submitted to frequency analysis, for the evaluation of prosthetic screw failure percentage (explained variable) in each explicative variable. Multiple linear regression was applied to correlate the screw failure with the explained variable and to confirm results the Tobit regression method for censored variables.
Results
Frequency analysis
From the 971 implants, 238 were rehabilitated with single prostheses and 733 with multiple prostheses, including partial arch (168) and total arch (69). From this amount, 21 showed prosthetic screw failure (8.82%) and 74 (10.1%), respectively. From the evaluated 912 straight abutments, 86 (9.43%) presented screw failure. From the 59 angled abutments, 9 (15.25%) failed. Two-hundred prostheses were made directly on the implant platform, and from those 200, 26 (13%) had screw failures. A total of 8 (8.95%) screw failures were observed among the 771 prostheses placed on the abutment.
Multiple linear regression and Tobit method
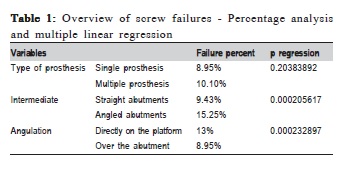
The explicative variable 'type of prosthesis' had p=0.20, the 'presence or not of intermediate', p=0.00020 and 'angulation' had p=0.00023 as may be seen in the Table 1.
By multiple linear regression, it may be stated that the type of prosthesis did not show statistically significant differences on the prosthetic screw failure, but other explicative variables were related with this mechanical failure (p<0.05).
Both linear regression and the Tobit method showed one f of significance lower than 5% (0.003), which prevents rejecting the null hypothesis and turns the model valid.
The explanation percentage of the model was close in both methods (1.8% in the linear regression and 1.76% in Tobit), indicating that new variables can be incorporated to the model to facilitate more learning.
The results demonstrated relationship between the explained variable and the explanatory variables with a significance of F 0.003 and p<0.05.
Discussion
Regarding the type of prosthesis, multiple prostheses showed more screw failures (10.1%) compared with the single prosthesis (8.82%), contradicting what is found in the literature. This may be explained since the number of multiple prostheses (773) was larger than the single ones (238). Pjetursson et al.1, showed in a systematic review that 5.6% of single crowns and 4% of fixed dental prostheses (FDPs) presented screw loosening and 0.3% to 0.8% screw fractures in 5 years, respectively. Glauser et al.7, observed 5.55% of screw loosening in single crowns and Bambini et al.8, 9.37%, close to the results of this study. The third most common technical complication of FDPs found by Pjetursson et al.4 was abutment or occlusal screw loosening. The cumulative complication rate after 5 years follow-up was 5.3%.
The angled abutments had more screw failures (15.25%) than the straight ones (9.43%), probably due to the small area of contact between the screw thread and the abutment. Another possibility described in the literature is the masticatory force, which is not distributed on the long axis of the implant, but can be questioned due to the occlusal force exerted axially on the prosthetic screw. When compressive occlusal loads are applied along the implant axis, a torsional force that may increase the risk of screw loosening or fracture is created. Compared with a straight abutment, a 15º to 25º abutment angulation increased the micromotion level by 30 percent. This micromotion may explain the screw failure9. However, not a single screw failure occurred in a study with 2261 implants evaluated for 96 months10.
The restorations placed directly on the implant generated more failures (15,25%) compared with the 8.95% on abutments. These results are confirmed by Montero et al.6 that connected 10.8% of screw failure of reconstructions to UCLA castable abutments. These findings may be explained by the reduction of the torque values after casting procedures and the presence of roughness and irregularities on the contact surface2. The misfit between implant and abutment increases stress on the screw and results in metal fatigue failure and screw loosening10-11. Even the smallest misfit could result in changes in screw geometry and cause incidence of strain on the screws12. However, Junqueira's et al study demonstrated that mechanical cycling reduced the torque of abutments without significant difference between cast or pre-machined UCLA abutments (p=0.908)13.
The statistical analysis indicated that new variables may be included in the model for further learning. This mechanical failure may be related with other variables like the length of the crown, type of antagonist, initial preload or torque value, time in place, veneering material and overload. The relationship between these variables and the prosthetic screw failure should be availed.
The change of screw material from titanium to gold, the use of defined screw fixation torques and implants with internal connections led to significant lowering of screw loosening1,9. Another alternative to reduce the screw loosening is the conical spring washer that extends its resistance to loosening14-16.
It was concluded that the presence or absence of intermediate and the abutment angulation are directly related to prosthetic screw failure in implant-supported prostheses, and the type of prosthesis has no significant relation with the presence of faults. Considering the outstanding need of similar studies with sample quantities and control over external factors, these results are considered highly significant. Due to the consequences generated by mechanical failures it is important to consider these factors in the prognosis of rehabilitation treatment.
Acknowledgements
The authors declare that there is no financial support by any agency.
References
1. Pjetursson BE, Dent M, Perio MAS, Asgeirsson AG. Improvements in implant dentistry over the last decade/ : comparison of survival and complication rates in older and newer publications Bjarni. Int J Oral Maxillofac Implants. 2014; 29: 308-24. [ Links ]
2. Ha C-Y, Lim Y-J, Kim M-J, Choi J-H. The influence of abutment angulation on screw loosening of implants in the anterior maxilla. Int J Oral Maxillofac Implants. 2011; 26: 45-55.
3. Barbosa GS, Silva-Neto JP Da, Simamoto-Júnior PC, Neves FD Das, Mattos MDGC De, Ribeiro RF. Evaluation of screw loosening on new abutment screws and after successive tightening. Braz Dent J. 2011 [cited 2014 Oct 15]; 22: 51-5. Available from: http://www.scielo.br/pdf/bdj/v22n1/ v22n01a09.pdf.
4. Pjetursson BE, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res. 2012; 23(Suppl 6): 22-38.
5. Kim E-S, Shin S-Y. Influence of the implant abutment types and the dynamic loading on initial screw loosening. J Adv Prosthodont. 2013 [cited 2015 Mar 10]; 5: 21-8. Available from: http://www.ncbi.nlm.nih.gov/pmc/ articles/PMC3597922/pdf/jap-5-21.pdf.
6. Montero J, Manzano G, Beltrán D, Lynch CD, Suárez-García M-J, Castillo-Oyagüe R. Clinical evaluation of the incidence of prosthetic complications in implant crowns constructed with UCLA castable abutments. A cohort follow-up study. J Dent. 2012; 40: 1081-9.
7. Glauser R, Sailer I, Wohlwend A, Studer S, Schibli M, Schärer P. Experimental zirconia abutments for implant-supported single-tooth restorations in esthetically demanding regions: 4-year results of a prospective clinical study. Int J Prosthodont. 2004; 17: 285-90.
8. Bambini F, Muzio L Lo, Procaccini M. Retrospective analysis of the influence of abutment structure design on the success of implant unit. Clin Oral Implants Res. 2001; 12: 319-24.
9. Kao H-C, Gung Y-W, Chung T-F, Hsu M-L. The influence of abutment angulation on micromotion level for immediately loaded dental implants: a 3- D finite element analysis. Int J Oral Maxillofac Implants. 2007; 23: 623-30.
10. Sethi a, Kaus T, Sochor P. The use of angulated abutments in implant dentistry: five-year clinical results of an ongoing prospective study. Int J Oral Maxillofac Implants. 2000; 15: 801-10.
11. Barbosa GAS, Bernardes SR, das Neves FD, Fernandes Neto AJ, de Mattos MDGC, Ribeiro RF. Relation between implant/abutment vertical misfit and torque loss of abutment screws. Braz Dent J. 2008 [cited 2014 Dec 5]; 19: 358-63. Available from: http://www.scielo.br/pdf/bdj/v19n4/ v19n4a13.pdf.
12. Burguete RL, Johns RB, King T PE. Tightening characteristics for screwed joints in osseointegrated dental implants. J Prosthet Dent. 1994; 71: 592-9.
13. Junqueira MC, Ribeiro RF, Faria ACL, Macedo AP, Almeida RP. Screw loosening of different UCLA-type abutments after mechanical cycling. Braz J Oral Sci. 2013 [cited 2014 Aug 22]; 12: 228-32. Available from: http:// www.scielo.br/pdf/bjos/v12n3/a14v12n3.pdf.
14. Jamiyandorj O, Kim S, Shim J-S, Lee K-W. Effect of using a titanium washer on the removal torque of an abutment screw in the external connection type of dental implant. Implant Dent. 2012; 21: 156-9.
15. Tom W. P. Korioth, Antonio C. Cardoso AV. Effect of washers on reverse torque displacement of dental implant gold retaining screws. J Prosthet Dent. 1999; 82: 312-6.
16. Versluis a, Korioth TW, Cardoso A C. Numerical analysis of a dental implant system preloaded with a washer. Int J Oral Maxillofac Implants. 1999; 14: 337-41.
 Correspondence:
Correspondence:
Carolina Schäffer Morsch
Rua Ana Luiza Vieira Street, 143, apt 305
CEP 88063-640 - Campeche
Florianópolis, SC, Brazil
E-mail: dracarolmorsch@gmail.com
Received for publication: May, 17 2015
Accepted: September, 17 2015
