










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.14 no.3 Piracicaba Jul./Set. 2015
ORIGINAL ARTICLE
Feasibility of including trained acupuncturists in the detection of oral lesions and oral cancer screening
Roberta Blanco dos SantosI; Luciane ZaninII; Flávia Martão FlórioI
I São Leopoldo Mandic - SLMANDIC, School of Dentistry and Research Center, Area of Public Health, Campinas, SP, Brazil
II Faculdade de Medicina de Jundiaí – FMJ, Medical School, Area of Public Health, Jundiaí, SP, Brazil and Fundação Hermínio Ometto - UNIARARAS, School of Dentistry, Area of Public Health, Araras, SP, Brazil
ABSTRACT
Aim: To demonstrate the feasibility of enabling trained acupuncturist as professionals able to detect oral lesions, with a role in the screening of oral cancer. Methods: This study was conducted in two phases. In the first, 11 acupuncturists were trained for visual detection of oral lesions and support content available on : <www.kankou.com.br>, especially developed for this study. They were evaluated at the end of training by a written exam. The inclusion criteria were to sign the consent form and to obtain a minimum of 90% of correct answers in the assessment. Four acupuncturists fulfilled both criteria and were included as study subjects. In the second phase, the subjects and the researcher (gold standard) examined 43 volunteer patients. The inclusion criterion for volunteers was just to sign the consent form. The volunteers' sample was established by saturation. Volunteers with changes deemed suspicious by the subjects were reexamined 15 days after the first examination. Results: First exam: mouth alterations were detected in 56% (n=24) of the volunteers. Among the alterations, 21% (n=5) were deemed suspicious by the subjects and 8% (n=2) by gold standard. Second exam: two mouth alterations remained suspicious and these volunteers were referred to the Dental Specialty Center for diagnosis and treatment. Compared to the gold standard, no injury remained undetected by the subjects. Conclusions: This study concluded for the feasibility of enabling trained acupuncturist to visually detect oral lesions and have a role in oral cancer screening.
Keywords: acupuncture; mouth neoplasms; pathology, oral diagnosis; training.
Introduction
Oral cancer is considered the 12th most common malignant tumor worldwide1. The incidence in 2008, for both sexes, was 263,020 cases for cancer in the lip and oral cavity, with a mortality rate of 127,6542.
In Brazil, mortality rates due to oral cancer in 1994 were 2,899 and 707 per 100,000 for men and women, respectively. In 2004, they increased to 4,418 and 1,045. In 2008, the number of deaths due to oral cancer reached 6,265 combining men and women3.
Most tumors arise in the oral cavity preceded by potentially malignant lesions or even as a carcinoma in situ, with intraoral manifestation as a white or red patch. Therefore, early diagnosis is consensually paramount4.
Statistically, almost half of all cases are detected at advanced stages, therefore, 50% of patients have a probable average survival of five years only5-6.
Early detection of oral lesions is best achieved by dentists, who perform oral examinations routinely in their professional practice7-8.
The incorporation of professionals other than dentists and physicians, such as community health care workers, dental nurses and dental hygienists to identify oral lesions has been suggested in literature to improve early diagnosis and treatment of these lesions4,9-10.
Acupuncture is a therapy advocated by Chinese Medicine and is regarded as Traditional Medicine11, based on its own medical rationality. According to Dr. Madel Luz, the term "medical rationality" must be understood as an operational concept to the style of a Weberian model, which establishes that any medical rationality denotes a complex, symbolic and empirically structured system in six fundamental dimensions: cosmology, medical doctrine, morphology, physiology or human vital dynamics, a diagnostic system and a therapeutic intervention system12.
In Brazil, acupuncturists are included in the Unified Health System (SUS), in accordance with the National Policy for Complementary and Integrating Practices (PNPIC – Política Nacional de Práticas Integrativas e Complementares)13 and similar to dentists, acupuncturists have regular access to the oral cavity to perform tongue examination, analyzing the shape, color, coating and changes of the tongue, to gather information about the patient's health. This is an important stage of the anamnesis, according to Traditional Chinese Medicine/Acupuncture semiology14.
This may be an opportunity for early detection of oral precursor lesions and, therefore, prevent oral cancer, provided they are properly trained.
Patients seeking acupuncture are not after an oral examination primarily, but a well-trained acupuncturist may by occasion visually detect the presence of oral lesions that can be suggestive of oral cancer and refer the patient for diagnosis, thus acting within the principles of referral and counter-referral13.
In view of the aforementioned arguments, the purpose of this study was to evaluate the feasibility of including adequately trained acupuncturists in the team of professionals able to detect oral lesions, thus widening the spectrum of professionals that may help oral cancer prevention.
Material and methods
This study was performed according to principles established by Resolution 196/96 of the National Health Council of the Ministry of Health, approved by Committee of Ethics for Research of São Leopoldo Mandic School of Dentistry and Research Center (nº 2012/0363). The subjects and volunteers signed an Informed Consent Form.
Phase 1 – Capacitation
Twelve acupuncturists were invited to participate in the capacitation phase, and 11 accepted the invitation. The training was carried out by a dentist also acupuncturist aiming to prepare the acupuncturists for detects oral lesions visually.
The training process consisted of six-hour theory lessons, for which the candidates were present. The lessons comprised the below-described subjects, based on the literature2-3,9,15-17 and adapted to this study: anatomy of the oral cavity, variations of normality, epidemiology of oral cancer, types of lesions found in the oral cavity, risk factors for oral cancer, visual examination of the mouth for lesions, using a especially designed map for this study.
The acupuncturists enrolled in the capacitation course received all lecture materials in printed form as well as supporting references on the website www.kankou.com.br, specifically designed for this study17. In standard mandarin, official language of the People's Republic of China, birthplace of acupuncture, the name kankou ( 看口- kànkǒu ) of the site may be translated as "look in the mouth". The site was developed in five languages.
At the end of the theory lessons, the enrolled acupuncturists were subjected to a written exam to demonstrate the knowledge they acquired on routine examination of the mouth, risk factors for oral cancer and visual detection of oral lesions or absence thereof. Photographs of the oral cavity exhibiting some alterations were used. The acupuncturists were expected not only to identify them but also to classify them into categories based on the atlas issued by the International Agency for Research on Cancer (IARC)15, "A digital manual for the early diagnosis of oral neoplasia", adapted for this study:
a) Anatomical variations: anatomical structures that may suggest pathology but are normal;
b) Common lesions: idiopathic changes or alterations related to non-neoplastic pathology;
c) Benign lesions: alterations compatible with benign tumors or similar to benign tumors;
d) Potentially malignant lesions: changes that suggest a potential for cancer development;
e) Malignant lesions: changes highly suspicious of oral cancer.
In order to qualify for the second phase of the study, the acupuncturists were expected to achieve 90% of correct answers in the written exam and to sign the consent form. Four acupuncturists were successful in fulfilling the inclusion criteria.
Phase 2 – Exams
In the second phase of the study, the subjects chose patients from the Acupuncture outpatient clinic at Pedro de Alcântara Hospital - Rio de Janeiro - RJ, who hereafter will be referred to as 'the volunteers'.
The inclusion criterion for the volunteers was only their acceptance to take part by signing a consent form, as proposed by the acupuncturists to the volunteers.
The final sample of volunteers was defined by saturation18, i.e., inclusion was suspended when the obtained data started to present, according to the researcher, redundancy and repetition. Therefore, during the data collection period, from December 2012 to April 2013, 43 volunteers were included.
An oral examination form was specifically designed for this study and after the examination a copy was attached to the patient's records.
It should be stressed that, in this phase of the study, the subjects were instructed to classify the lesions with a potentially malignant or malignant aspect into a single group, namely suspicious lesions, since diagnosis is no part of the acupuncturist's scope.
The volunteers were randomly examined by the subjects, following the outpatient routine of the institution, e.g., at the time of the consultation, the volunteer would be seen by any of the subjects available at the time. The volunteers that wore removable prosthetic appliances were instructed to remove them for examination purposes.
As acupuncture contraindicates the often necessary tongue traction maneuvers to examine the posterior third of the tongue because of possible pressure-induced changes to color or coating status, as it could compromise the data deemed necessary for acupuncture, a set of specific guidelines was designed and made available for acupuncturists at the website: www.kankou.com.br17.
The examination performed by the head researcher was considered as gold standard and, therefore, she re-examined the volunteers on the same day.
According to the National Institute of Cancer (INCA) directions16, volunteers that presented suspicious oral lesions were re-examined 15 days after the first examination by the same subject and then by the gold standard.
The volunteers presenting oral changes compatible with common lesions and/or benign lesions were advised to have regular follow-ups with a dentist.
At the end of the study, the volunteers with suspicious oral lesions were referred to the oral medicine service of the Dental Specialty Center (Centros de Especialidades Odontológicas - CEO) for diagnosis and treatment whenever applicable.
Education and Health Promotion
All volunteers received instructions regarding the risks involved with tobacco use and other risk factors for oral cancer as well as treatment options to help quitting their tobacco habits should they be smokers3,19.
Data analysis
The data were recorded on Microsoft Excel 2010 and analyzed descriptively using figures containing data on distribution as well as absolute and relative frequencies.
Results
Phase 1 – Capacitation
From the 11 acupuncturists that took part in the capacitation, 64% (n=7) had 90% or more correct answers, whilst 36% (n=4) scored between 80 to 90% in the written exam.
The results showed that among the subjects, 18% (n=2) were male and 82% (n=9) female. The mean age was 52.6 years (SD=6.87). Those with a college degree were 82% (n=9) against 18% (n=2) with a high school degree. Subjects with a health-related background were 55% (n=6), humanities background were 36% (n=4) and technology background 9% (n=1). Regarding the acupuncture training, 46% (n=5) were qualified by a postgraduate course in acupuncture, 36% (n=4) by a technical course and 18% (n=2) by an open course. The average time in practice as professional acupuncturists was 9 years.
Four acupuncturists were included as subjects, all of them females aged between 50 to 60 years. Regarding education level, 75% (n=3) had a college degree (physical education, social sciences and psychology) and 25% (n=1) had a high school degree. Regarding their acupuncture training, 75% (n=3) were qualified by a technical course acknowledged by the Ministry of Education (MEC) and the State Education Secretariat (SEE) – RJ, whereas 25% (n=1) was qualified by an open course. Their average acupuncture practice time was 9 years.
Phase 2 – Examination
Among the volunteers, 35% (n=15) were male and 65% (n=28) were female. Their age ranged from 12 to 79 years, with a mean age of 55 years (SD=15.42). Regarding tobacco use, 11% (n=5) were current smokers, 5% (n=2) were former smokers and 84% (n=36) were non-smokers.
Once the oral examination was performed both by the subjects and the gold standard, visible alterations were identified in 56% (n=24) of the volunteers, whilst no changes were observed in 44% (n=19).
Figure 1 shows the total results in relation to the gold standard.
Amongst the detected alterations, 16% (n=4) were considered as variations of normal anatomy, 46% (n=11) as common changes, 17% (n=4) as benign lesions and 21% (n=5) as suspicious lesions.
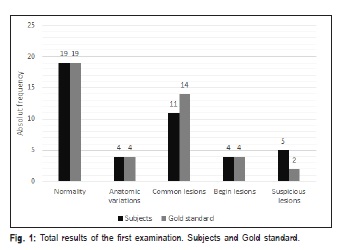
According to the gold standard of this study, among the lesions found in the first examination, 17% (n=4) were classified as anatomical variations, 58% (n=14) as common lesions, 17% (n=4) as benign lesions and 8% (n=2) as suspicious lesions.
The gold standard of this study identified 60% (n=3) of the lesions identified as suspicious by the subjects as low severity on visual examination.
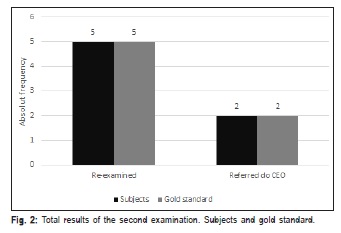
The results from the second examination of the oral cavity performed 15 days after the first, as advised for the volunteers detected by the subjects as suspicious lesions and therefore needing confirmation, are described in Figure 2.
Among the five subjects re-examined, 40% (n=2) presented persisting lesions and were referred to the CEO for diagnosis and treatment, according to the criteria established by the dentist in charge of the local specialty service.
Discussion
In Brazil, the demand for acupuncture in the public sector increased 128% in two years, according to data from the Ministry of Health, increasing from 97,274 consultations in 2007 to 221,862 in 200920.
The increased supply of acupuncture treatment in the Unified Health System (SUS) was one of the basic aspects in this study. The aim was to evaluate the feasibility of including appropriately trained acupuncturists to visually detect oral lesions, on account that these professionals have regular access and familiarity with the oral cavity to examine the tongue in their routine practice, as well as being part of SUS, according to the National Policy for Complementary and Integrating Practices (PNPIC – Política Nacional de Práticas Integrativas e Complementares)13.
The scientific literature suggests the inclusion of other professional categories for the task of detecting oral lesions suggestive of cancer, thus favoring early diagnosis of the disease, as reported by LeHew et al.9, where training was provided to physicians, nurses and a hospital administrator for that purpose. Melo et al.10 and Morse et al.4 encourage the capacitation of community health workers and other professionals involved in primary care, such as dental hygienists and nurses, in order to increase the chances of early detection, which therapeutically would result in less complex and more effective approaches, thus improving prognosis and reducing treatment costs4,9-10.
There are no studies in the literature regarding the feasibility of training acupuncturists for visual detection of oral lesions. This study is the first to demonstrate a successful outcome from training acupuncturists and, differently from LeHew et al.9, they were trained for visual detection of oral lesions, supervised during examination and assessed both at the capacitation and clinical examination phases.
The availability of an electronic source for support (<www.kankou.com.br>)17 made it easier for the subjects to access the teaching material anytime and anywhere, which was also used during the examination phase to clarity questions that could relative to the detected oral changes.
Expanding knowledge through digital media has been used by the Ministry of Health in an attempt to overcome the territorial and sociocultural distances of the Brazilian population and health professionals. At the same time, it contributes to ongoing education in health, diagnosis and information on general health. Advantages such as fast and easy access, as well as interaction and research incentives make the digital media an important permanent tool that may encourage the professionals to search for information in order to complement their practice in the health services21-23.
Regarding screening programs, the Canadian Task Force on Preventive Health Care (CTFPHC) and the United States Preventive Service Task Force (USPSTF), do not advise the inclusion of organized oral cancer screening in routine practice, according to a systematic review performed by the American Dental Association Council on Scientific Affair. Instead, they recommend that screening be directed only at those at higher risk of developing oral cancer24. Opportunistic screening has yet no firm evidence on effectiveness to be included or excluded from routine practice16,25.
This study suggests that opportunistic screening may occur during a consultation with a trained acupuncturist, especially at the primary care level established by SUS, where the acupuncturist is included according to the PNPIC13 and considering that 221,862 acupuncture consultations were recorded in 200920.
During the clinical examination phase, initial resistance by the patients (volunteers) to allow a complete oral examination was noticed, e.g., embarrassment upon denture removal. In order to solve this issue, the posture and explanations offered by the acupuncturist, in terms of objectives and possible benefits, the ease, speed, lack of risk and cost of the examination during the history were essential. Care and a competent patient approach are narrowed down to the concept of Humanization, which is based on respect and dignity, thus constituting a process that aims at cultural institutional change, via the construction of ethical commitments and methods for health care26. In this study, following explanation to the volunteers, full compliance was obtained and the screening process was performed satisfactorily.
Currently, acupuncture has different levels of academic qualifications in Brazil, especially those as a specialist degree (latu sensu ) offered by universities. There are still some technical courses running in some States of the Federation regulated by MEC and SEE, as well as open courses. Although acupuncture is not a registered profession per se, in 1982 the Ministry of Work and Employment – MTE designed the Brazilian Classification of Occupations, which included the occupation of acupuncturist. A newer version of the classification was made based on Entry nº397/2002, describing the profession of acupuncturist as independent from any other professional class, including medicine, with its own registration nº 3221-0527.
According to the gold standard, at the first examination, a higher severity was attributed to some oral alterations. Such conduct did not imply risks to the patient. On the second examination, both subjects and gold standard showed agreement.
Taking into account the fears and expectations experienced by the volunteers facing suspicious lesions, despite the advice to wait 15 days to follow them up, acupuncturists should promptly refer patients with suspicious lesions to a dentist, a dental school or other health services in their region.
Acupuncture is mostly known in the West for the analgesic activity, acting by the release of endogenous opioid peptides28 but its semiology and diagnosis methods deserve our attention.
Based on the results presented in this study, the inclusion of acupuncturists in the detection of oral lesions that suggest oral cancer may increase the number of patients undergoing oral examination secondary to acupuncture sessions. Such opportunistic screening may also be widened to include the private sector, where most acupuncturists are placed29, thus contributing even further for early referral, diagnosis and treatment of oral cancer.
The afore mentioned data and the results presented in this study suggest that if training were to be offered in regular acupuncture courses, the dentist should be administering its content, since they are the professionals with suitable experience to perform opportunistic oral cancer screening and they also have the knowledge to train professionals to assist them in doing so7,10,30.
This study established an interdisciplinary team approach focusing on the visual detection of oral lesions, capacitating and including acupuncturists in a field primarily dominated by dentists and eventually by physicians.
Decuyper et al.31 highlighted that cooperation, communication and the opportunity to confront and integrate knowledge and individual competencies are fundamental actions and, moreover, experiencing a constructive conflict that reveals the diversity of opinions may guide interdisciplinary actions, thus integrating and shaping cooperative active professionals within their working environment.
Therefore, although this study may present some limitations such as a small sample, it verified the feasibility of including appropriately trained acupuncturists into the practice of visual detection of oral lesions, thus contributing to early detection of oral cancer in the public and private health services, via visual examination of the entire oral cavity as part of their clinical practice.
References
1. Eadie D, MacKintosh AM, MacAskill S, Brown A. Development and evaluation of an early detection intervention for mouth cancer using a mass media approach. Br J Cancer. 2009; 101 (Suppl 2): S73-9. [ Links ]
2. IARC. GLOBOCAN 2008 Fast Stats. Section of Cancer Information 2010 [cited: 2013 Aug 27]. Available form: http://globocan.iarc.fr/factsheets/ populations/factsheet.asp?uno=900#BOTH.
3. WHO Health Statistics and Health Information Systems 2013 [cited 2013 Aug 26]. Available fromt: http://www.who.int/healthinfo/mortality_data/en/ index.html.
4. Morse DE, Vélez-Vega CM, Psoter WJ, Vélez H, Buxó CJ, Baek LS, et al. Perspectives of San Juan healthcare practitioners on the detection deficit in oral premalignant and early cancers in Puerto Rico: a qualitative research study. BMC Public Health. 2011; 11: 391.
5. Kujan O, Glenny AM, Duxbury J. Evaluation of Screening Strategies for Improving Oral Cancer Mortality: A Cochrane Systematic Review. J Dent Educ. 2005; 69: 255-65.
6. Gomez IS, Warnakulasuriya S, Varela-Centelles PI, Lopez-Jornet P, Suarez- Cunqueiro M, Diz-Dios P, et al. Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay? Oral Diseases. 2010; 16: 333-4.
7. Applebaum E, Ruhlen TN, Kronenberg FR, Hayes C, Peters ES. Oral cancer knowledge, attitudes and practices: a survey of dentists and primary care physicians in Massachusetts. J Am Dent Assoc. 2009; 140: 461-7.
8. Epstein JB, Sciubba JJ, Banasek TE, Hay LJ. Failure to diagnose and delayed diagnosis of cancer: medicolegal issues. J Am Dent Assoc. 2009; 140: 1494-503.
9. LeHew CW, Epstein JB, Koerber A, Kaste L. Training in the primary prevention and early detection of oral cancer: Pilot study of its impact on clinicians' perceptions and intentions. Ear Nose Throat J. 2009; 88: 748-53.
10. Melo NS, Figueiredo PTS, Leile AF, Souza TAC, Lucena, EHG, Zanetti CHG. Early oral diagnosis in the Uniûed National Health System: individual analysis, health surveillance and teamwork as a (re)structuring possibility. Tempus - Actas Saude Colet. 2011 [cited 2013 Sep 21]; 5: 89-103. Available from: http://www.tempusactas.unb.br/index.php/tempus/article/view/1045.
11. Choi SH. WHO Traditional Medicine Strategy and Activities "Standardization with Evidence-based Approaches". J Acupunct Meridian Stud. 2008; 1: 153-4.
12. Tesser CD, LUZ MT. [Medical rationalities and integrality]. Cienc. Saude Colet. 2008; 13: 195-206. Available from: http://www.scielo.br/pdf/csc/v13n1/ 23.pdf. Portuguese.
13. Brazil. Ministry of Health. National Policy on Integrative and Complementary Practices in Unified Health System - Extension attitude access. Brasília: Ministry of Health, 2006.
14. World Health Organization (WHO). Consultation on acupuncture guidelines on basic training and safety in acupuncture. WHO: Cervia; 1996.
15. IARC. IARC Screening Group. A digital manual for the early diagnosis of oral neoplasia [cited 2013 Aug 27]. Available from: http://screening.iarc.fr/ atlasoral.php.
16. Brazil - INCA. National Cancer Institute. Mouth cancer. 2012 [cited 2013 Jul 27]. Available from: http://www2.inca.gov.br/wps/wcm/connect/ tiposdecancer/site/home/boca/evidencias_cientificas_para_rastreamento.
17. Kankou - The acupuncturist and the inspection of the tongue. Learn to optimize your routine clinical examination and participate in the prevention of mouth cancer. 2013 [cited 2014 Mar 18]. Available from: http://www.kankou.com.br.
18. Denzin NK, Lincoln YS, editors. Handbook of qualitative research. Thousand Oaks: Sage Publications; 1994.
19. Santos JDP, Duncan BB, Sirena SA, Vigo A, Abreu MSN. [Indicators of effectiveness of the Unified Health System Smoking Cessation Program in Minas Gerais, Brazil, 2008]. Epidemiol Serv Saude. 2012; 21: 579-88. Portuguese.
20. Aranda F. IG homepage. [Health and Wellbeing]; 2010 Aug 24 [cited 2014 Mar 3]. Available from: http://saude.ig.com.br/bemestar/ em+dois+anos+acupuntura+gratuita+cresce+128+no+pais/ n1237750946329.html. Portuguese.
21. Cardoso BAP, Pacheco CMA, Souza RF. [Website development on the internet. Permanent improvement in nursing: Contribution for continuing education]. Enfermeria Global. 2010 [cited 2013 Aug 27]; (19). Available from: http://scielo.isciii.es/pdf/eg/n19/miscelanea2.pdf. Spanish.
22. Rezende EJC, Melo MCB, Tavares EC, Santos AF; Souza C. [Ethics and eHealth: reflections for a safe practice]. Rev Panam Salud Publica. 2010; 28: 58-65.Portuguese
23. Rendeiro MMP, Vieira P, Figueiredo DLTM. [Infoculture: a barrier of access to permanent learning?] Rev Hosp Univ Pedro Ernesto. 2012 [cited 2014 Jan 1];11(Suppl 1). Available at: http://revista.hupe.uerj.br/ detalhe_artigo.asp?id=303.
24. Rethman MP, Carpenter W, Cohen EE, Epstein J, Evans CA, Flaitz CM et al. Evidence-based clinical recommendations regarding screening for oral squamous cell carcinomas. J Am Dent Assoc. 2010; 141: 509-20.
25. Brazil. Ministry of Health. [Screening: Series A - Standards and Technical Manuals. Primary Care Guide, n. 29]. Brasília: Ministry of Health; 2010. Portuguese.
26. Rios IC. [Health humanization pathways - practice and reflection]. São Paulo: Áurea; 2009 [cited 2015 nov 3]. Available from: http:// pessoacomdeficiencia.sp.gov.br/usr/share/documents/ CAMINHOS_DA_HUMANIZACAO_NA_SAUDE.pdf. Portuguese.
27. Kurebayash LSF, Oguisso T, Freitas GF. Acupuncture in brazilian nursing practice: ethical and legal dimensions. Acta Paul Enferm. 2009; 22: 210-2.
28. Gondim DV, Carvalho KM, Vale ML. Pain behavior to electroacupuncture in rabbit tooth pulp. Braz J Oral Sci. 2010; 9: 415-20.
29. Sousa IM, Bodstein RC, Tesser CD, Santos F de A, Hortale VA. [Integrative and complementary health practices: the supply and production of care in the Unified National Health System and in selected municipalities in Brazil]. Cad Saude Publica. 2012; 28: 2143-54. Portuguese.
30. Wade J, Smith H, Hankins M, Llewellyn C. Conducting oral examinations for cancer in general practice: what are the barriers? Fam Pract. 2010; 27: 77-84.
31. Decuyper S, Dochy F, Van den Bossche P. Grasping the dynamic complexity of team learning: An integrative model for effective team learning in organisations, Educ Res Rev. 2010; 5: 111-33.
 Correspondence:
Correspondence:
Roberta Blanco dos Santos
Praça General Portinho nº6 apt 203
CEP: 20271-010 Maracanã
Rio de Janeiro, RJ, Brasil
E-mail: robertablanco@gmail.com
Received for publication: August 30, 2015
Accepted: September 28, 2015
