










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkBrazilian Journal of Oral Sciences
versão On-line ISSN 1677-3225
Braz. J. Oral Sci. vol.15 no.1 Piracicaba Jan./Mar. 2016
ORIGINAL ARTICLE
Removable orthodontic appliances: frequency and cleaning agents used by students and recommended by dentists
Rita Regina Souza LamasI, Mabel Miluska Suca SalasI, Tatiana Pereira CenciII,Marcos Britto CorrêaI,Rafael Guerra LundI
I Universidade Federal de Pelotas – UFPel, Pelotas Dental School, Department of Restorative Dentistry, Pelotas, RS, Brazil
II Universidade Federal de Pelotas – UFPel, Pelotas Dental School, Area of Prosthetic Dentistry, Pelotas, RS, BrazilCorrespondence
ABSTRACT
Aim: To evaluate the prevalence and hygiene habits of 13-19 years-old adolescent users of removable orthodontic appliances (ROA) and to determine hygiene methods for the appliances prescribed by dentists, in the city of Pelotas. Methods:The study had two stages. The first stage was a telephone interview with dentists. Dentists were interview by telephone calls in order to obtain information regarding the hygiene methods for cleaning acrylic appliances. Second stage was a cross-sectional study performed with schoolchildren. Children from public and private schools with secondary level were included in the sample. A questionnaire was applied to the students using any type of ROA. Questionnaires included demographic information and behavioral characteristics. Data collected were subjected to Chi-square test and logistic regression. Results: he prevalence of children using ROA was 5.4%. Students (89.7%) and dentists (47.2%) reported to prefer mechanical methods to clean their ROA. Cleaning with soup, hydrogen peroxide or effervescent tabs were less used. High frequency of use was associated with higher frequency of hygiene on the ROA. Conclusion: The prevalence of schoolchildren using removable appliances was low. The common cleaning method used by children and prescribed by dentists was mechanical. Hygiene frequency was significantly associated with the routine of use of the appliance and with the type of hygiene method..
Keywords: Adolescent. Disinfection. Hygiene. Orthodontic Appliance Design.
Introduction
Concern for aesthetics has increased in the population1 and during the last three decades there has been a great demand for orthodontic treatments2. Children in treatment with removable orthodontic appliances (ROA) have higher risk for proximal caries, gingivitis and halitosis than children without ROA3.
A proper hygiene of the orthodontic appliances could reduce bacteria in the oral environment4. Studies have investigated the efficacy of diverse hygiene methods to control the presence of microorganism in removable acrylic appliances5-9. Most of them showed that the combination of a mechanical and chemical methods reduced microorganisms on the appliance surface, compared with other methods7-9.
The role of the dentist in oral health promotion is important since dentists have evidence-based knowledge of oral health and could influence patient's behavior10. Few studies investigated the attitudes of dentists toward oral preventive measures. Habits and characteristics of orthodontic patients including hygiene and attitudes toward ROA are scarce. Moreover, studies assessing the hygiene methods used by children to clean their ROA are inexistent. Knowledge of children's characteristics treated with orthodontic appliances is important. Dentist's recommendation should include effective alternatives to reduce microbiota and be able to prevent oral diseases. The present study had two objectives: (1) to determine the prevalence of the ROA use in schoolchildren and its possible association with some socio-demographic factors and hygiene habits; and (2) to verify the hygiene methods prescribed by dentists.
Material and methods
The study was approved by the Ethics Committee of the Federal University of Pelotas (protocol number 216/2011 UFPel/RS).
A cross-sectional study was performed among schoolchildren and dentists in Pelotas, a mid-sized city of the southern Brazil, 260 km from Porto Alegre, the capital of Rio Grande do Sul state.
The study was performed in two stages.
1) Dentists interview.
A full list of the dentists registered in the state was obtained from the Regional Council of Dentistry of Rio Grande do Sul state (CRO – RS) and the Brazilian Dental Association – region of Pelotas (ABO-Pelotas).
Eligibility criteria for the enrollment of dentists for this study: dentists living in the city of Pelotas, actively working in the clinical practice with treatments involving ROA and that agreed to participate were included in the study. Dental specialties of dentists were not asked. Interviews were conducted by phone calls.
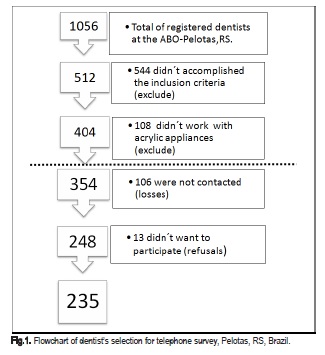
The sequence to obtain the final dentists sample is shown in Figure 1 . The questionnaire included two open question regarding the recommended methods and frequency (once, twice and three times a day) for ROA cleaning. Dentists not contacted on the first call, were re-called. After the third attempt without contact, dentists were considered as losses.
2) Students interview
According to the Department of Education of Rio Grande do Sul State, Pelotas has 19 states, 1 municipal and 9 private schools with secondary education. The number of children enrolled in secondary education of the city was 9,237 in public schools and 1,711 in private schools.
Stratification by type of school (private and public) was carried out from the number of high schools. Four private schools and 16 public schools were randomly selected by the method of proportionality, where the probability of selection is proportional to the number of students in the school. The number of 20 schools was adequate to ensure good variability of the sample11. Students from secondary education were initially eligible for the study. Schoolchildren enrolled regularly in the selected high schools of the city, users of ROA and able to answer the questionnaires were included in the study. Parents or legal guardians and school tutors signed a written consent form to allow the participation of adolescents. Previously developed questionnaires were administered to children by an interviewer in the classrooms. The interviewer was a previously trained post-graduate student.
Questionnaires included socio-demographic and behavioral data of children, such as age (complete years and later categorized in 13-14, 15-17, 18-19), sex, type of school, mother's education in years (categorized in ≤ 8, 9-12, ≥13), frequency of ROA use (categorized in sometimes and frequently), ROA time of use, reason for the orthodontic treatment, usage discomfort and cleaning method of ROA. The frequency of hygiene of the ROA was categorized in low - one or less times during a week - and high - every day.
Statistical analysis
Data were recorded in duplicate in the EpiData 3.1 database (version 3.1, release 2006, EpiData Association, Denmark). Statistical analyses were carried out in Stata 10.0 (StataCorp. 2007. Stata Statistical Software: Release 10; StataCorp LP College Station, TX, USA). Descriptive analysis was performed to describe the dentists' recommendations and the children's studied characteristics. Bivariate analyses were performed to assess the association between frequency of hygiene (outcome) and the investigated variables (age, sex, type of school, frequency of ROA use, reason for treatment, maternal education and cleaning habits) of children using ROA. Pearson's chi-square test or Linear Trend were used depending on the type of variable. Variables with p-value <0.30 were included in the multivariate analysis. For multivariate analysis, the Poisson regression was used, considering a p value <0.05 as statistically significant with 95% confidence interval.
Results
In the city of Pelotas 1,056 dentists were on the ABO-RS list. After the application of the eligibility criteria, 354 dentists remained as potential participants. Two hundred and thirty five dentists participated in the study. The response rate was 66.4%. The selection process of the dentists is in Figure 1.
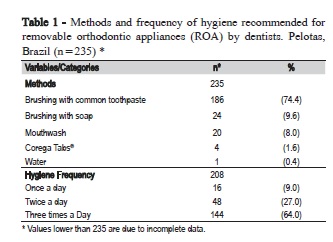
Table 1 describes dentists' recommendations. Dentists recommended mainly to brush the acrylic appliances with toothpaste (74.4%), 9.6% indicated to brush the ROA with soap, 8.0% advised immersions in hypochlorite, chlorhexidine or peroxide solutions, 6.0% suggested other cleaning materials, 1.6% suggested Corega Tabs®, and 0.4% to brush with water. Most dentists recommended cleaning the removable appliances 3 times per day (64.0%).
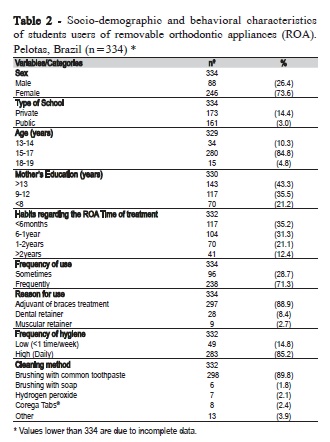
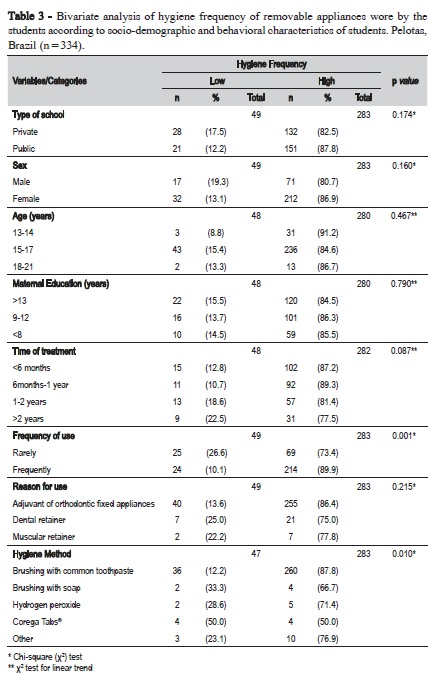
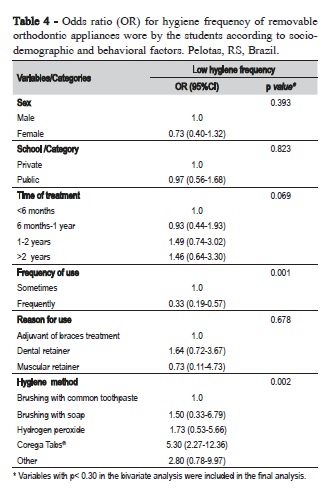
Distribution of the children according to the outcome and the investigated factors is presented in Table 2. Our study included a total of 6,158 schoolchildren from high schools. The prevalence of the ROA users in the schools was 5.4% (n=334). In private schools, the frequency of ROA users was 14.3% and in public schools it was 3.0%. Data showed that most users of the removable appliances were female (73.6%). A larger number of 15-17-year-old children (84.8%) used ROA as the main orthodontic treatment. Most children (35.1%) were using their ROA for 6 months or less. Children used their ROA daily (71.3%). The ROA were used mostly after the fixed appliances as adjuvant to orthodontic treatments (88.9%). Most students (85.2%) cleaned their ROA daily. The method most commonly used was brushing with toothpaste (89.8%). Bivariate analysis is described in Table 3. Adolescents who used their ROA only occasionally also cleaned them less frequently (p<0.001). The type of cleaning method was associated with the hygiene frequency (p<0.001) and children with lower frequency of hygiene used less frequently brushing tooth with soap. Multivariate analysis (Table 4) showed that children that used their ROA frequently had less chances to clean less their appliances (OR = 0.33; 95% CI: 0.19 to 0.57).
Discussion
In our study, the prevalence of schoolchildren from high schools using ROA was 5.4%. This result was lower than other studies12,13. Krey and Hirsch13 (2012) found that 16% of 11-14-year-old children used ROA in Germany. In England, Chestnutt et al.12 (2006) observed that 28% of 12-year-old children and 18% of 15-year-old children used ROA. This difference may be explained by the fact that in other countries such as Germany13 and England12, orthodontic treatments were included in the health insurance, allowing orthodontic treatment for children. In Brazil, the public health services do not include the orthodontic treatment as primary care policy, situation that could produce some social inequalities regarding the need and the actual used of an orthodontic appliance. In the present study, most children using an orthodontic appliance came from private schools. However, these results were not statistically different. Demographic characteristics of the population can also influence the access to orthodontic treatment. The present study found a higher frequency of girls (73.6%) using removable appliances. Similar results were found by O'Brien et al.14 (1996). This situation was attributed to a higher demand of esthetic treatments by women15.
Regarding the hygiene methods, schoolchildren mostly used toothbrush and toothpaste to clean their ROA (89.9%). Patients often clean their acrylic removable appliances with toothbrush and toothpaste12. This method was reported to be effective to maintain the health of the mucosa in contact with the acrylic appliance16. The use of a single hygiene method, without any chemical disinfectant, has been criticized, due to its poor biofilm removal from acrylic surface and improper control of microbial load8. In fact, several cleaning methods were investigated, including mechanical, chemical or the combination of both methods. The use of chlorhexidine6, mechanical brushing with water8 or effervescing tabs5 has shown a reduction of microbial load, but the comparison was with surfaces without any cleaning. Studies have observed that the combination between a mechanical and a chemical method reduced significantly the presence of microorganisms7-9 from removable appliances compared with other methods.
Our results showed that dentists that usually work with acrylic appliances recommended mainly brushing the acrylic appliances with toothpaste (74.4%). Eichenauer et al.17 (2012) reported similar results regarding dentists' attitudes regarding hygiene method for ROA. These results contradict those of several studies8-9 with the most effective method to remove oral microbiota from surfaces. The dental practice should be related to these findings. Studies have shown that some dental recommendations and examination protocols used by dentists are partially18 or totally in disagreement with scientific evidence19. The clinician's decisions seem to be influenced by their knowledge and attitudes, as well as the dentist's feelings and conscience10. The cost of the hygiene materials seems to be an important factor that determines dentists' recommendations, as well as the facility for cleaning the ROA by patients17.
Oral hygiene instructions for patient self-care and for ROA cleaning are important activities to promote oral health and prevent diseases. Healthy behaviors can prevent future oral problems. Dentists could influence the patient behaviors10. For instance, the schoolchildren in our study seem to follow dentists' recommendations regarding ROA care. The importance of a correct hygiene relies on adequate control of the biofilm on surfaces20, especially for children undergoing orthodontic treatment. Adolescence also could modulate and promote the increment of microorganism in the oral environment21 increasing the risk for caries and gingivitis3. It is necessary to learn the habits of children's at risk to implement adequate oral health education programs.
Some limitations of this study can be pointed out. It had a cross-sectional design which is limited to the moment of data collection. The response rate of dentist was intermediate and was obtained by telephone survey. Surveys have used telephone contact to obtain information in a fast way, with low cost22, especially if used as complement of other methods23. However, the telephone method has some limitations and could induce biased answers, increasing non-responses and lack of representativeness. To minimize bias, we used telephone survey and the internet to contact and interview dentists.
Even though in our study it was observed descriptively that adolescents are using the same cleaning method recommended by dentists, both observations were conducted in two different populations. Hence, it is not possible to make predictions using any correlation.
Further research should be conducted to define the profile of children in orthodontic treatment and the optimal methods for cleaning ROAs, and most important to communicate this protocol to orthodontists/dentists and the population.
In conclusion, the prevalence of schoolchildren using ROA is low. Children frequently clean the ROA and frequently use them. The cleaning method prescribed by dentist and used by adolescents are different from the most effective method showed in the literature.
Acknowledgements
The authors are grateful to the State secretary of Education, the Municipal Secretary of Education and the Direction of Private and public Schools, which allowed the study to be performed.
References
1. de Couto Nascimento V, de Castro Ferreira Conti AC, de Almeida Cardoso M, Valarelli DP, de Almeida-Pedrin RR. Impact of orthodontic treatment on self-esteem and quality of life of adult patients requiring oral rehabilitation. Angle Orthodont. 2016 Feb. [ Links ]
2. Dimberg L, Lennartsson B, Arnrup K, Bondemark L. Prevalence and change of malocclusions from primary to early permanent dentition: a longitudinal study. Angle Orthod. 2015 Sep;85(5):728-34. doi: 10.2319/080414-542.1.
3. Pathak AK, Sharma DS. Biofilm associated microorganisms on removable oral orthodontic appliances in children in the mixed dentition. J Clin Pediatr Dent. 2013 Spring;37(3):335-9.
4. Chauhan P, Dua VS, Kainth N, Tosh A, Tomar A. The effect of various oral hygiene products on the microbial flora in patients undergoing orthodontic treatment. APOS Trends Orthod. 2015;5(2):63-9.
5. Nisayif DH. The effects of removable orthodontic appliance hygiene on oral flora. J Bagh College Dentistry. 2009;21(2):105-8.
6. Friedman M, Harari D, Raz H, Golomb G, Brayer L. Plaque inhibition by sustained release of chlorhexidine from removable appliances. J Dent Res. 1985 Nov;64(11):1319-21.
7. Salas MMS, Lamas RRS, Cenci TP, Lund RG. How are children and adolescents cleaning their orthodontic appliances? A cross-sectional study in private schools. Braz J Oral Sci. 2014 Jan/Mar;13(1):34-6.
8. Paranhos HF, Silva-Lovato CH, de Souza RF, Cruz PC, de Freitas-Pontes KM, Watanabe E, et al. Effect of three methods for cleaning dentures on biofilms formed in vitro on acrylic resin. J Prosthodont. 2009 Jul;18(5):427-31. doi: 10.1111/j.1532-849X.2009.00450.x.
9. Peixoto IT, Enoki C, Ito IY, Matsumoto MA, Nelson-Filho P. Evaluation of home disinfection protocols for acrylic baseplates of removable orthodontic appliances: A randomized clinical investigation. Am J Orthod Dentofacial Orthop. 2011 Jul;140(1):51-7. doi: 10.1016/j.ajodo.2009.12.036.
10. Madan C, Arora K, Chadha VS, Manjunath BC, Chandrashekar BR, Rama Moorthy VR. A knowledge, attitude, and practices study regarding dental floss among dentists in India. J Indian Soc Periodontol. 2014 May;18(3):361-8. doi: 10.4103/0972-124X.134578.
11. Bennett S, Woods T, Liyanage WM, Smith DL. A simplified general method for cluster-sample surveys of health in developing countries. World Health Stat Q. 1991;44(3):98-106.
12. Chestnutt IG, Burden DJ, Steele JG, Pitts NB, Nuttall NM, Morris AJ. The orthodontic condition of children in the United Kingdom, 2003. Br Dent J. 2006 Jun 10;200(11):609-12;quiz 638.
13. Krey KF, Hirsch C. Frequency of orthodontic treatment in German children and adolescents: influence of age, gender, and socio-economic status. Eur J Orthod. 2012 Apr;34(2):152-7. doi: 10.1093/ejo/cjq155.
14. O'Brien K, McComb JL, Fox N, Wright J. Factors influencing the uptake of orthodontic treatment. Br J Orthod. 1996 Nov;23(4):331-4.
15. Zhang YF, Xiao L, Li J, Peng YR, Zhao Z. Young people's esthetic perception of dental midline deviation. Angle Orthod. 2010 May;80(3):515-20. doi: 10.2319/052209-286.1.
16. Rossato MB, Unfer B, May LG, Braun KO. Analysis of the effectiveness of different hygiene procedures used in dental prostheses. Oral Health Prev Dent. 2011;9(3):221-7.
17. Eichenauer J, Serbesis C, Ruf S. Cleaning removable orthodontic appliances: a survey. J Orofac Orthop. 2011 Oct;72(5):389-95. doi: 10.1007/s00056-011-0043-2.
18. Norton WE, Funkhouser E, Makhija SK, Gordan VV, Bader JD, Rindal DB, et al. Concordance between clinical practice and published evidence: findings from The National Dental Practice-Based Research Network. J Am Dent Assoc. 2014 Jan;145(1):22-31. doi: 10.14219/jada.2013.21.
19. Frame PS, Sawai R, Bowen WH, Meyerowitz C. Preventive dentistry: practitioners' recommendations for low-risk patients compared with scientific evidence and practice guidelines. Am J Prev Med. 2000 Feb;18(2):159-62.
20. Duyck J, Vandamme K, Krausch-Hofmann S, Boon L, De Keersmaecker K, Jalon E, et al. Impact of Denture Cleaning Method and Overnight Storage Condition on Denture Biofilm Mass and Composition: A Cross-Over Randomized Clinical Trial. PLoS One. 2016 Jan 5;11(1):e0145837. doi: 10.1371/journal.pone.0145837.
21. Sampaio-Maia B, Monteiro-Silva F. Acquisition and maturation of oral microbiome throughout childhood: An update. Dent Res J (Isfahan). 2014 May;11(3):291-301.
22. Mokdad AH, Remington PL. Measuring health behaviors in populations. Prev Chronic Dis. 2010 Jul;7(4):A75. Epub 2010 Jun 15.
23. Moura EC, Claro RM, Bernal R, Ribeiro J, Malta DC, Morais Neto O. A feasibility study of cell phone and landline phone interviews for monitoring of risk and protection factors for chronic diseases in Brazil. Cad Saude Publica. 2011 Feb;27(2):277-86.
 Corresponding author:
Corresponding author:
Rafael Guerra Lund
Universidade Federal de Pelotas, Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
Área de Concentração em Dentística
Rua Gonçalves Chaves, 457 / Sala 503 – Centro
CEP: 96015568, Pelotas, RS, Brasil
E-mail: rafael.lund@gmail.com
Received for publication: March 09, 2016
Accepted for publication: May 17, 2016
