










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.11 no.1 Recife Jan./Mar. 2012
RELATO DE CASO / CASE REPORT
Surgical excision of mucocele with local anesthesia in an 8-month-old baby
Excisão cirúrgica de mucocele sob anestesia local em um bebê de 8 meses de idade
Carla Vecchione GurgelI; Natalino Lourenço NetoI; Dafna Geller-PaltiI; Vivien Thiemy SakaiII; Thaís Marchini de OliveiraIII; Maria Aparecida de Andrade Moreira MachadoIII
IMaster, Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo
IIPhD, Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo
IIIAssociate Professor, Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo
ABSTRACT
Mucoceles are common disorders of the minor salivary glands, occurring specially on the lower lip. Their occurrence in newborn babies has rarely been reported. In addition, the surgical removal of oral lesions in babies has often been performed with general anesthesia, which option is usually related to the patients' ages, irrespective of the lesion's size and the access to anatomic region where it is located. The present report, however, details the treatment of a mucocele excision performed in an 8-month-old baby with local anesthesia. This case illustrates well that knowledge of the lesion and dentist's experience in the attendance of babies is important, as often only conservative treatment with local anesthesia is required. Therefore, clinicians and parents should be reassured that early surgical intervention under local anesthesia will provide a swift and satisfactory resolution to the problem.
KEYWORDS: Infant; Mucocele; Oral Surgery; Mouth Mucosa.
RESUMO
Mucocele é uma ocorrência comum nas glândulas salivares menores, que acontece, principalmente, no lábio inferior. Em bebês, tem sido raramente reportada na literatura. Em adição, a remoção cirúrgica de lesões orais em bebês tem sido realizada sob anestesia geral, cuja opção geralmente se refere à idade do paciente, sem ter relação com o tamanho da lesão e o acesso à região anatômica onde está localizada. O presente caso clínico, no entanto, descreve a excisão da mucocele realizada em um bebê de 8 meses de idade, sob anestesia local. Esse caso ilustra bem que o conhecimento da lesão e a experiência do dentista no atendimento de bebês é muito importante, já que somente um tratamento conservador sob anestesia local é necessário. Portanto, clínicos e pais devem ser alertados para o fato de que uma intervenção cirúrgica precoce sob anestesia local irá proporcionar uma resolução rápida e satisfatória do problema.
Descritores: Mucocele; Cirurgia bucal; Mucosa Bucal.
INTRODUCTION
Mucoceles are probably the most common disorders of the minor salivary glands1-4, typically presenting as single bluish or translucent asymptomatic nodules, especially on the lower lip1-3,5. They are fluctuant and movable because of their mucinous contents. The diameter may range from a few millimeters to a few centimeters. If left without intervention, episodic decreases and increases in size may be observed, corresponding to rupture and subsequent mucin production2.
The majority of mucoceles are extravasation type in which there is pooling of mucus in the connective tissue presumably arising from trauma to a salivary duct. Less common are retention mucoceles, resulting from ductal obstruction and retention of saliva within the ductal system. The two types of mucoceles cannot be distinguished clinically1,3,6.
Extravasation mucoceles have a tendency to occur in younger patients whereas retention mucoceles may occur most often in middle to late life1,3. Few cases have been reported in the first decade of life7,8 and their occurrence in newborn babies has rarely been reported1,6,9,10,11. In babies, the surgical removal of oral lesions has been performed with general anesthesia1,6. The present report, however, details the treatment of a mucocele excision performed in a baby with local anesthesia.
CASE REPORT
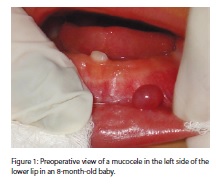
An 8-month-old white baby girl was referred to the dentist presenting a "little ball" on the lower lip. The mother reported during the anamnesis that the girl presented 4 similar lesions since birth, but 3 have remised spontaneously and one had not changed in size since that time.
Upon examination, a small, pedunculated papule with the overlying mucosa of normal appearance was observed in the left side of the lower lip (Figure 1). Primary mandibular left central incisor had just erupted in the oral cavity.
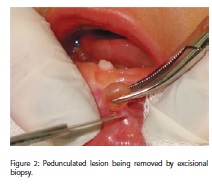
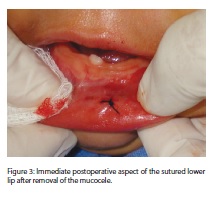
The lesion was suggestive of mucocele and excisional biopsy was performed under local anesthesia (Figures 2 and 3). The wound was further closed with 4-0 suture (Figure 4).
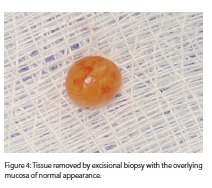
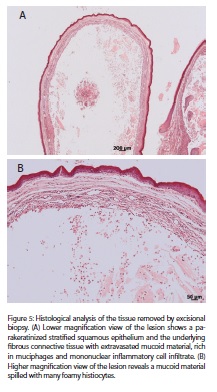
The removed tissue was sent to histopathological examination (Figure 5). Microscopic sections (Figure 6) revealed an oral mucosa composed of parakeratinized stratified squamous epithelium.
The underlying fibrous connective tissue exhibited extravasated mucoid material containing several muciphages, surrounded by hemorrhage, focal hemosiderosis and predominantly mononuclear inflammatory cell infiltrate. No salivary glands were found.

Postoperative recovery was uneventful with the patient returning to normal feeding within some hours. Suture was removed 1 week after the surgery. No recurrence was observed up to 18-months follow-up examinations.
DISCUSSION
In practice, mucoceles are hardly ever considered a clinical problem1, although sometimes they can appear alarming especially to the child's parents6. Mucoceles occur in both genders in all age groups, the peak of incidence being between 10 and 29 years3. These lesions are rare in infants and have been rarely reported in neonates1,6,12.
Currently, the main area of controversy surrounding the mucocele in neonates is related to the anesthetic modality that should be used during surgical excision. Surgical removal under general anesthesia has been indicated for the treatment of congenital lesion1,6. The option for general anesthesia is usually related to the patients' ages1 irrespective of the size of the lesion and the access to anatomic region where it is located.
Despite a decline in mortality in pediatric general anesthesia during the last two decades, publications still highlight the high incidence of perioperative morbidity and the increased risk for perioperative critical events among newborns and infants13. In addition, although the majority of children undergoing anesthesia is healthy, it is crucial to detect any underlying risk factor that may lead to an unexpected adverse event in the perioperative period13.
This case illustrates well that knowledge of the lesion and dentist's experience in the attendance of babies are important, as often only conservative treatment with local anesthesia is required. Differently from the conservative approach we proposed for the treatment of congenital epulis14, in this case the surgical removal was necessary because development of a mucocele is characterized by intermittent episodes of increased and decreased volumes1. In addition, teeth were beginning to erupt in the baby's oral cavity, and repeated trauma arising out of feeding habits could initiate inflammatory/ hemorrhagic phenomena, leading to a more generalized disturbance1.
In conclusion, clinicians and parents should be reassured that early surgical intervention under local anesthesia will provide a swift and satisfactory resolution to the problem.
REFERENCES
1. Gatti AF, Moreti MM, Cardoso SV, Loyola AM. Mucus extravasation phenomenon in newborn babies: report of two cases. Int J Paediatr Dent. 2001 Jan;11(1):74-7. [ Links ]
2. Mustapha IZ, Boucree SA Jr. Mucocele of the upper lip: case report of an uncommon presentation and its differential diagnosis. J Can Dent Assoc. 2004 May;70(5):318-21. [ Links ]
3. Porter SR, Scully C, Kainth B, Ward-Booth P. Multiple salivary mucoceles in a young boy. Int J Paediatr Dent. 1998 Jun;8(2):149-51. [ Links ]
4. Sousa FB, Etges A, Corrêa L, Mesquita RA, de Araújo NS. Pediatric oral lesions: a 15-year review from São Paulo, Brazil. J Clin Pediatr Dent. 2002 Summer;26(4):413-8. [ Links ]
5. Bermejo A, Aguirre JM, Lopez P, Saez MR. Superficial mucocele: report of 4 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Oct;88(4):469-72. [ Links ]
6. Crean SJ, Connor C. Congenital mucoceles: report of two cases. Int J Paediatr Dent. 1996 Dec;6(4):271-5. [ Links ]
7. Cataldo E, Mosadomi A. Mucoceles of the oral mucous membrane. Arch Otolaryngol. 1970 Apr;91(4):360-5. [ Links ]
8. Harrison JD. Salivary mucoceles. Oral Surg Oral Med Oral Pathol. 1975 Feb;39(2):268-78. [ Links ]
9. Meechan JG, Blair GS. Bilateral lower lip mucoceles: cause of functional malocclusion in a three-year-old child. J Dent Child. 1986 Sep-Oct;53(5):386-7. [ Links ]
10. Poker ID, Hopper C. Salivary extravasation cyst of the tongue. Br J Oral Maxillofac Surg. 1990 June; 28(3):176-7. [ Links ]
11. Standish SM, Shafer WG. The mucus retention phenomenon. J Oral Surg Anesth Hosp Dent Serv. 1959 July; 17(4):15-22. [ Links ]
12. Das S, Das AK. A review of pediatric oral biopsies from a surgical pathology service in a dental school. Pediatr Dent. 1993 May/June;15(3):208-11. [ Links ]
13. Von Ungern-Sternberg BS, Habre W. Pediatric anesthesia - potential risks and their assessment: part I. Paediatr Anaesth. 2007 Mar;17(3):206-15. [ Links ]
14. Sakai VT, Oliveira TM, Silva TC, Moretti AB, Santos CF, Machado MA. Complete spontaneous regression of congenital epulis in a baby by 8 months of age. Int J Paediatr Dent. 2007
Jul;17(4):309-12.
 Endereço para correspondência:
Endereço para correspondência:
Carla Vecchione Gurgel
Al. Octávio Pinheiro Brisolla, 9-75 - Bauru/SP CEP 17012-901
e-mail: carlagurgel@usp.br
Recebido para publicação: 11/05/10
Aceito para publicação: 15/07/10
