










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.12 no.1 Recife Jan./Mar. 2013
ARTIGO ORIGINAL / ORIGINAL ARTICLE
Oral smooth muscle tumors: analysis of 49 cases and literature review
Tumores musculares orais: análise de 49 casos e revisão de literatura
Paula Prieto OliveiraI; Fábio Daumas NunesI
I Faculdade de Odontologia da Universidade de São Paulo (USP)- São Paulo- Brasil
ABSTRACT
The aim of this study is to analyse and compare the clinical features of leiomyoma and leiomyosarcoma, because they help in the differential diagnosis. Records from Oral Pathology Department of Dental School at University of São Paulo during the period 1962-2010 were analysed. There were 49 cases of smooth muscle tumors: 27 leiomyomas and 22 leiomyosarcomas. Cases of smooth muscle tumors of the oral cavity were also compiled from 1970 to 2010. These tumors represented 0,092% of all oral lesions, with similar distribution between genders. Leiomyoma was more frequent in the fifth decade of life. The lips and the tongue were the most common sites. The majority of cases were asymptomatic. The accomplished treatment was surgical excision, with excellent prognosis. Leiomyosarcoma was more frequent in patients up to 50 years and the jaws were the most affected sites. The majority of cases were symptomatic and the pain was the most present symptom. Complete surgical resection was the most appropriate treatment. The recurrence rate was 27%, with 24% of metastasis and 30% of mortality, demonstrating the bad prognosis of this lesion.
KEYWORDS: Leiomyoma, leiomyosarcoma, epidemiology, mouth.
RESUMO
O objetivo deste estudo foi avaliar e comparar as características clínicas de leiomioma e leiomiossarcoma de boca, visto que auxiliam no diagnóstico diferencial. Foram analisados 49 casos de tumores de músculo liso em cavidade oral diagnosticados no Departamento de Patologia Bucal da Faculdade de Odontologia da Universidade de São Paulo entre 1962 e 2010, sendo 27 leiomiomas e 22 leiomiossarcomas. Também foi realizado um levantamento de casos de tumores de músculo liso publicados na literatura entre 1970 e 2010. Foi observada uma frequência de 0,092% de tumores de músculo liso em boca, com distribuição semelhante entre os sexos. O leiomioma foi mais comum na quinta e sexta décadas de vida, sendo os lábios e a língua os locais mais afetados. A maioria dos casos eram assintomáticos. O tratamento realizado foi a excisão cirúrgica, com prognóstico excelente. Já o leiomiossarcoma apresentou maior frequência em pacientes acima de 50 anos, sendo os ossos gnáticos as regiões mais acometidas. A maioria dos pacientes eram sintomáticos e a dor foi o sintoma mais encontrado. O tratamento mais adequado foi a ressecção cirúrgica completa.O índice de recidiva foi de 27%, com 24% de metástases e 30% de mortalidade, demonstrando o prognóstico sombrio dessa lesão.
DESCRITORES: Leiomioma, leiomiossarcoma, epidemiologia, boca.
Introduction
Smooth muscle tumors are very rare in the oral cavity due to the scarcity of smooth muscle in this region, and arise mainly from tunnica media of blood vessels. Leiomyomas represent from 0,016% to 0,064% of buccal benign lesions, while leiomyosarcomas are even less frequent1,2,3,4.
The histologic distinction between atypical leiomyoma and low grade leiomyosarcoma is difficult and is based on the following criteria: number of mitosis, cellular atypia and pattern of necrosis5,6. However, there isn't an exact number of mitosis or other features that warrants separation between both lesions. For this reason, clinical data are of paramount importance and must be considered in the diagnosis.
The aim of this retrospective study is to evaluate and compare clinical features, like gender, age, location and symptomatology of leiomyoma and leiomyosarcoma, and review the literature from 1970 to 2010, since there isn't any recent comparative article.
Material and Methods
Records of oral leiomyoma and leiomyosarcoma from Oral Pathology Department of Dental School at University of São Paulo during the period 1962-2010 were analysed. A review of published cases from 1970 to 2010 was accomplished by means of pubmed. Only english articles were considered. Data from both casuistry were analysed separately, including age, sex, race, location, symptomatology, treatment and prognosis. Cases with uncertain location were excluded.
Results
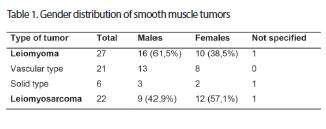
Nine thousand seven hundred and seventy histopathologic exams were accomplished during this period and only 64 (0,092%) were diagnosed as smooth muscle tumors, that corresponded to 49 cases, being 27 (55%) leiomyomas e 22 (45%) leiomyossarcomas. From 27 leiomyomas, 21 (78%) were vascular type and only 6 (22%) were solid, no epithelioid was found. The table 1 shows distribution of lesions according to gender. This datum was known in 47 cases. There was a male predominance in leiomyomas, with incidence of 61,5%, while leiomyosarcomas were more common in females, that corresponded to 57,1% of cases. The male-female ratio was 1,6:1,0 for leiomyoma and 1,0:1,3 for leiomyosarcoma.
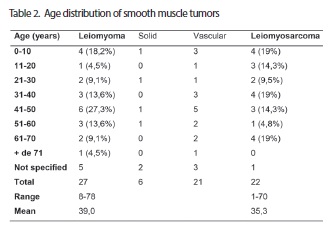
The age was known in 43 cases (table 2). The leiomyoma ocurred mainly in the fifth decade of life, while leiomyosarcoma presented a more balanced distribution between age groups. The age of leiomyoma patients ranged from 8 to 78 years, with mean of 39 years; while age of leiomyosarcoma patients ranged from 1 to 70 years, with mean of 35 years.
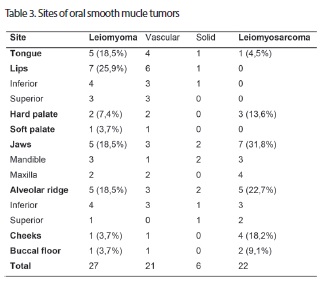
For location (table 3), leiomyomas were more common in lips, tongue, jaws and alveolar ridge, while leiomyosarcomas were more frequent in the jaws, followed by alveolar ridge and cheeks.
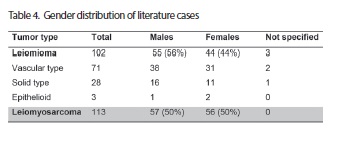
There were 215 published cases of smooth muscle tumors from 1970 to 2010: 102 leiomyomas and 113 leiomyosarcomas. Out of 102 leiomyomas, 71 (69,6%) were vascular, 28 (27,4%) solid and 3 (3%) epithelioid. Table 4 shows distribution of lesions according to gender. This information was known in 99 cases. The men were more affected in leiomyomas, while leiomyosarcomas presented a similar distribution between genders. The ratio male-female was 1,2:1,0 for leiomyomas and 1,0:1,0 for leiomyosarcomas.
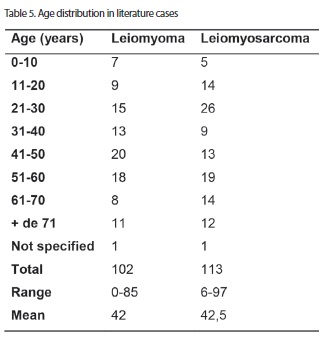
The age was known in 213 cases (table 5). Leiomyomas were more common in fifth and sixth decades of life, while leiomyosarcomas affected mainly the third decade of life. The age varied from 2 months to 85 years, with mean of 42 years, for leiomyoma, and from 6 to 97 years, with mean of 42,5 years for leiomyosarcoma.
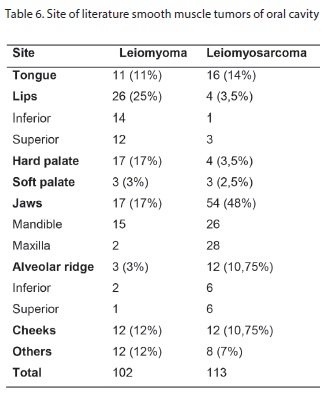
For location (table 6), leiomyomas were more common in lips, hard palate and jaws, while leiomyosarcomas affected mainly the jaws, tongue, alveolar ridge and cheeks.
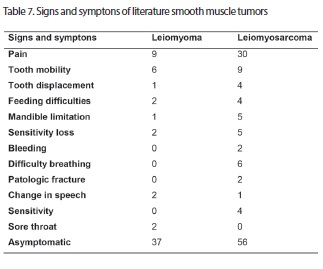
The symptomatology was related in 75 pacients with leiomyoma and 92 with leiomyosarcoma. Out of these cases, 75% and 40%, respectively, were asymptomatic. The main signs and symptons observed are described in table 7.
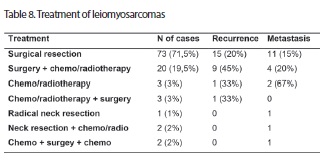
Surgical excision was accomplished for all leiomyomas with related treatment. For leiomyosarcomas, the main treatment of choice was surgical resection in the 102 patients with known treatment (table 8).
Follow up data were reported for 53 cases with leiomyoma and 95 cases with leiomyosarcoma. Only 3 (6%) leiomyomas were reported to recur. Out of leiomyosarcomas, 26 (27%) presented recurrence, 23 (24%) suffered metastases and 29 (30%) died of disease.
Discussion
The frequency of smooth muscle tumors in our study was very low and corresponded to 0,092% of all biopsies, as described in literature1,4,7. There was a slight predominance of leiomyomas (55%) in relation to leiomyosarcomas (45%), although some authors report that only from 20% to 25% of oral smooth muscle tumors are malignant1,8. The most common histological type of leiomyoma in both analyzed groups was vascular, as observed in others studies2,8,9,10,11,12,13,15,16. However, Liang et al 17 found a slight predominance of solid leiomyoma.
Males were more affected in leiomyomas of both casuistics, as described by other articles1,2,7,14,15,16,17,18. However, Brooks et al 19 and Gaitan-Cepeda et al 20 found more females. Ravindranathan and Heslop21, Praal et al 22, Giles and Gosney23, Yamamoto et al 24 and Epivatianos et al 25 didn't observed any gender predilection. For leiomyosarcomas, there was a slight predominance of women in our cases, while in literature cases no gender predilection was found. Dry et al 26, Lo Muzio et al 27, Vilos et al 3 and Centeno et al 28 also observed a slightly higher incidence of females. However, many authors reported a slight predominance of men1,15,29,30,31,32,33,34,35, and others observed intense predilection for males36,37,38,39,40,41.
The age more affected for leiomyomas was the fifth decade of life in both groups, as described by others articles9,10,12,14,15,19,20,21,22,23,25,42,43. However, Yamamoto et al 24found more frequency in the third and fouth decades of life. For leiomyosarcomas, there was a similar distribution between the ages in our casuistic, while in the literature cases, there was a predominance of third decade, as reported for Vilos et al 3. However, the majority of articles observed higher incidence in older patients, up to 50 years15,27,30,33,35,41,44. Yan et al 34 found more frequency of second and fifth decades of life.
For location, the leiomyomas were more common in lips in both groups, as reported by others studies2,7,12,13,14,15,19,42,43,45. However, some articles found higher incidence in tongue1,9,21,22,23,25. The leiomyosarcomas affected mainly the jaws in both casuistics, agreeing with many studies3,15,26,29,30,33,34,39,40,46. However, Muzio et al 27 observed predominance of tongue and gums. Farman and Kay1, Robinson and Whyte47 found higher incidence in cheeks.
The majority of patients with leiomyoma were asymptomatic, as described in literature8,11,18,19,20,22,23,43,48,49,50. However, according to Wertheimer-Hatch et al 15, only 40% were asymptomatic. For leiomyosarcomas, 60% of cases presented some kind of symptomatology and the most found symptom was pain, agreeing with other sutdies15,26,30. However, according to Amarapala and Tilakaratne32, Ethunandan et al 33 and Yan et al 34, the most leiomyosarcomas are asymptomatic.
The treatment used for all leiomyomas was surgical excision and the prognosis was very good, with only 6% of recurrence, as described in literature2,8,15,16,17,18,19,21,22,45,50,51,52. For leiomyosarcomas, the majority of cases suffered surgical resection, with 20% of recurrence and 15% of metastasis. For surgery followed by chemo/radiotherapy, there was 45% of recurrence and 20% of metastasis. Many authors question the eficiency of radio and chemotherapy in the control of these lesions and claim that complete surgical resection is the best treatment3,31,34,39,41,53,54,55,56,57,58. However, Aydin and Dreyer59 used radiotherapy in an inoperable leiomyosarcoma in posterior region of tongue and there was remission of the lesion, without evidence of recurrence and metastasis after one year and six months of follow up. Mitsudo et al 60 accomplished chemotherapy with docetaxel and cisplatin using superselective intra-arterial infusion via superficial temporal artery for treatment of a leiomyosarcoma in the maxillary sinus and observed a reduction of more than 50% of tumor size. Abn et al 35 accomplished chemotherapy with ifosfamide and doxorubicin in an incurable leiomyosarcoma of tongue, with multiple metastases, as a palliation and ocurred a significant reduction of the lesion.
In our study, there was recurrence in 27% of patients with leiomyosarcoma, 24% were affected by metastases and 30% died of disease, showing the bad prognosis of tumor. Some authors report even higher indices15,30,32,33.
The literature review showed that smooth muscle tumors are very rare in the oral cavity and presented a similar distribution between genders. The leiomyoma is more common in the fifth decade of life and the most affected sites are lips and tongue. The majority of cases are asymptomatic. The treatment is surgical excision, with excelent prognosis and low recurrence index. The leiomyosarcoma presents higher incidence in people up to 50 years and affect mainly the jaws. The majority of patients are asymptomatic and the main symptom is pain. The best treatment is complete surgical resection. Radiotherapy is used in inoperable cases and chemotherapy as a palliation. The prognosis is bad, with high recurrence, metástase and mortality rates.
References
1. Farman AG, Kay S. Oral leiomyosarcoma. Report of a case and review of the literature pertaining to smooth muscle tumors of the oral cavity. Oral Surg. 1977;43(3):402-409. [ Links ]
2. Baden E, Doyle JL, Lederman DA. Leiomyoma of the oral cavity: a light microscopic and immunohistochemical study with review of the literature from 1884 to 1992. Oral Oncol, Eur J Cancer. 1994;30B(1):1-7.
3. Vilos GA, Rapidis AD, Lagogiannis GD, Apostolidis C. Leiomyosarcomas of the oral tissues: clinicopathologic analysis of 50 cases. J Oral Maxillofac Surg. 2005 Oct;63(10):1461-77.
4. Nonaka CFW, Pereira KMA, Miguel MCC. Oral vascular leiomyoma with extensive calcification areas. Braz J Otorhinolaryngol. 2010;76(4):539.
5. Bell SW, Kempson RL, Hendrickson MR. Problematic uterine smooth muscle neopasms. A clinicopathogic study of 213 cases. Am J Surg Pathol. 1994;18(6):535-58.
6. Hendrickson MR, Tavassoli FA, Kempson RL, Mc Cluggage WG, Haller U, Kubik-Huch RA. Mensenchymal tumours and related lesions. In: Tavassoli FA, Devilee P, editors. Word Health Organization Classification of tumours. Pathology and genetics of tumours of the breast and female genital organs. Lyon: IARC Press 2003.
7. Brooks JK, Ricalde P, Nikitakis NG, Levy BA. Angioleiomyoma of the togue. General Dentistry 2004;52(1):52-54.
8. Haedicke G, Kaban LB. Smooth-muscle tumors of the oral cavity. Plastic and Reconstructive Surg. 1988 feb;81(2):264-69.
9. Cherrick HM, Dunlap CL, King OH Jr. Leiomyomas of the oral cavity: review of the literature and clinicopathologic study of seven new cases. Oral Surg Oral Med Oral Pathol. 1973 jan;35(1):54-66.
10. Galili D, Shteyer A. Leiomyoma of the oral cavity. J Oral Med. 1974;29(3):69-71.
11. Natiella JR, Neiders ME, Greene GW. Oral leiomyoma: report of six cases and a review of the literature. J Oral Pathol. 1982;11:353-65.
12. Savage NW, Adkins KF, Young WG, Chapman PJ. Oral vascular leiomyoma: review of the literature and report of two cases. Aust Dent J. 1983;28(6):346-51.
13. Svane TJ, Brian RS, Cosentino BJ, Cundiff EJ, Ceravolo JJ. Oral leiomyomas: Review of the literature and report of a case of palatal angioleiomyoma. J Periodontol. 1986;57:433-35.
14. Esguep A, Solar M. Oral vascular leiomyoma- report of 5 cases and review of the literature. J Oral Med. 1986 apr-jun;41(2):126-29.
15. Wertheimer-Hatch et al. Tumors of the oral cavity and pharynx. World J Surg. 2000;24:395-400.
16- Lloria-Benet M et al. Oral leiomyoma: a case report. Oral Med. 2003;8:215-9.
17- Liang H, Frederiksen NL, Binnie WH, Cheng YS. Instraosseus oral leiomyoma: systematic review and report of one case. Dentomaxillofac Radiol. 2003;32(5):285-90.
18- Suresh L, Matsumura E, Calixto LEM, Ruckert E, Aguirre A. Intraosseous angiomyoma of the mandible. General Dentistry 2007;55(2):132-35.
19- Brooks JK et al. Clinicopathologic caracterization of oral angioleiomyomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:221-7.
20- Gaitan-Cepeda LA, Quezada-Rivera D, Tenorio-Rocha F, Leyva-Huerta ER, Mendez-Sánchez E. Vascular leiomyoma of the oral cavity. Clinical, histopathological and imunohistoquemical characteristics. Presentation of five cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2008 aug; 1;13(8):E483-8.
21- Ravindranathan N, Heslop IH. Oral leiomyoma- a case report and review of the literature. Br J Oral Surg 1978-79;16:93-99.
22- Praal FR, Ioannides CA, Beek GJ, Molengraft F. Oral leiomyomas. J Maxillofac Surg. 1982;10:229-35.
23- Giles AD, Gosney MBE. Oral angiomyoma: a case report. Br J Oral Surg. 1982;20:142-6.
24- Yamamoto H, Takagi M, Otake S, Ohmori Motoh. Leiomyoma of the right lower gingiva: a case and a review of the japanese literature. J Oral and Maxillofac Surg. 1983;41:671-75.
25- Epivatianos A, Trigonidis G, Papanayotou P. Vascular leiomyoma of the oral cavity. J Oral Maxillofac Surg. 1985;43(5):377-82.
26- Dry SM, Jorgensen JL, Fletcher CD. Leiomyosarcomas of the oral cavity: an unusual topographic subset easily mistaken for nonmesenchymal tumours. Histopathology 2000 Mar;36(3):210-20.
27- Lo Muzio L et al. Primary gingival leiomyosarcoma. A clinicopathological study of 1 case with prolonged survival. J Clin Periodontol 2002;29:182-7
28- Centeno CR, Nadini F, Adam R, Godoy H, Reichart PA. Primary leiomyosarcoma of the mandible. Oral Oncol Extra 2006;42:40-5.
29- Poon CK et al. Leiomyosarcoma of gingiva: Report of a case and review the literature. J Oral Maxillofac Surg. 1987;45(10):888-92.
30- Izumi K, Maeda T, Cheng J, Saku T. Primary leiomyosarcoma of the maxilla with regional lymph node metastasis. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Sep;80(3):310-9.
31- Carter LC et al. Primary leiomyosarcoma of the mandible in a 7 year old girl. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:477-84.
32- Amarapala H, Tilakaratne WM. Leiomyosarcoma of the oral cavity: Report of seven cases and review of the literature. Oral Oncol Extra 2006;42:14-17.
33- Ethunandan M, Stokes C, Higgins B, Spedding A, Way C, Brennan P. Primary oral leiomyosarcoma: a clinico-pathologic study and analysis of prognostic factors. Int J Oral Maxillofac Surg. 2007 May;36(5):409-16.
34- Yan B, Li Y, Pan J, Xia H, Li LJ. Primary oral leiomyosarcoma: a retrospective clinical analysis of 20 cases. Oral Dis. 2010 Mar;16(2):198-203.
35- Abn JH, Mirza T, Ameerally P. Leiomyosarcoma of the tongue with multiple metastases: a case report and review of the literature. J Oral Maxillofac Surg. 2011;
36- Brandjord RM, Reaume CE, Wesley RK. Leiomyosarcoma of the floor of the mouth: review of the literature and report of case. J Oral Surg. 1977 Jul;35:590-4.
37- Kratochvil FJ et al. Leiomyosarcoma of the maxilla. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol. 1982;54(6):647-55.
38- Miettinen M et al. Leiomyosarcoma of the mandible: diagnosis as aided by immunohistochemical demonstration of desmin and laminin. J Oral Pathol. 1984;13:373-81.
39- Nishi M, Mimura T, Senba I. Leiomyosarcoma of the maxilla. J Oral Maxillofac Surg. 1987;45:64-68.
40- Shenberg ME, Slootweg PJ, Koole R. Leiomyosarcomas of the oral cavity. Report of four cases and review of the literature. J Craniomaxillofac Surg. 1993; 21(8):342-7.
41- Yang SW, Chen TM, Tsai CY, Lin CY. A peculiar site of leiomyosarcoma: the tongue tip- report of a case. Int J Oral Maxillofac Surg. 2006;35:469-71.
42- Gutmann J et al. Angiomyoma of the oral cavity. Oral Surg Oral Med Oral Pathol. 1974;38:269-73.
43- Leung K, Wong DY, Li W. Oral leiomyoma:case report. J Oral Maxillofac Surg. 1990;48(7):735-38.
44- Sakamoto K et al. A case of leiomyosarcoma arising from the tongue. Oral Oncol Extra. 2005;41:49-52.
45- Anastassov GE, van Damme PA. Angioleiomyoma of the upper lip: report of a case. Int J Oral Maxillofac Surg. 1995;24:301-302.
46- Freedman PD, Jones AC, Kerpel SM. Epithelioid leiomyosarcoma of the oral cavity: report of two cases and review of the literature. J Oral Maxillofac Surg. 1993;51:928-32.
47- Robinson EC, Whyte AM. Leiomyosarcoma of the cheek: a case report. Br J Oral Surg. 1978-79;16:100-104.
48- McMillan MD, Ferguson JW, Kardos TB. Mandibular vascular leiomyoma. Oral Surg Oral Med Oral Pathol. 1986;62(4):427-33.
49- Toida M, Koizumi H, Shimokawa K. Painful angiomyoma of the oral cavity: report of a case and review of the literature. J Oral Maxillofac Surg. 2000;58:450-53.
50- Raffaini M et al. Mandibular leiomyoma in an infant. Report of a case. Int J Oral Maxillofac Surg. 1990;19:367-69.
51- Bertolini F et al. Mandibular intraosseus leiomyoma in a child: report of a case. J Clin Pediatr Dent. 2003;27(4):385-87.
52- Scheper MA, Nikitakis NG, Meiller TF. A stable swelling of the hard palate. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 oct;104(4):461-4.
53- Bass B et al. Case 62: Expansile radiolucent lesion of the mandible. J Oral Maxillofac Surg. 1986;44:799-803.
54- Martin-Hirsch DP et al. Post-irradiation leiomyosarcoma of the maxilla. J Laryngol Otol. 1991 dec;105:1068-71.
55- Lo Muzio L, Favia G, Mignogna MD, Piattelli A, Maiorano E. Primary intraoral leiomyosarcoma of the tongue: an immunohistochemical study and review of the literature. Oral Oncol. 2000 Nov;36(6):519-24.
56- Sumida T et al. Leiomyosarcoma of the maxillary sinus with cervical limph node metastasis. J Oral Maxillofac Surg. 2001;59:568-71.
57- Yadav R, Barathan S. Leiomyosarcoma of the buccal mucosa: A case report with immunohistochemistry findings. J Oral Sci. 2008;50(2):215-18.
58- Qureshi SS, Mistry RC, Natrajan G, Gujral S, Laskar S, Banavali S. Leiomyosarcoma of the maxilla as second malignancy in retinoblastoma. Indian J Cancer jul-sep 2008;45(3):123-25.
59- Aydin H, Dreyer T. Leiomyosarcoma of the base of the tongue treated with radiotherapy: a case report. Oral Oncol Eur J Cancer 1994;30B(5):351-55.
60- Mitsudo K et al. Leiomyosarcoma of the maxilla: effective chemotherapy with docetaxel (DOC) and cisplatin (CDDP) using superselective intra-arterial infusion via superficial temporal artery. Oral Oncol Extra 2006;48:258-62.
 Endereço para correspondência:
Endereço para correspondência:
Av Dr Altino Arantes 620 ap 201 Vila Clementino
CEP: 04041-003 São Paulo-SP
Master's degree student Oral Pathology Department from Dental School at University of São Paulo (USP)
e-mail: paulaprietoterra@yahoo.com.br
Recebido para publicação: 05/11/12
Aceito para publicação: 28/01/13
