










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.12 no.1 Recife Jan./Mar. 2013
ARTIGO ORIGINAL / ORIGINAL ARTICLE
Knowledge that general practitioners of dentistry have about treating tooth avulsion in João Pessoa/PB, Brazil
Conhecimento do cirurgião-dentista acerca do tratamento da avulsão dentária na cidade de João Pessoa/PB, Brasil
Julierme Ferreira RochaI; Fabiano Gonzaga RodriguesI; Eduardo Dias RibeiroII; Danilo Batista Martins BarbosaII; José Wilson NoletoI; José Cadmo Wanderley Peregrino de Araújo FilhoI; Tânia Lemos Coelho RodriguesII
I Department of oral and Maxillofacial Surgery, Federal University of Campina Grande,Patos,Paraíba/Brazil
II Department of Oral and Maxillofacial Surgery, Federal University of Paraíba, João Pessoa, Brazil
ABSTRACT
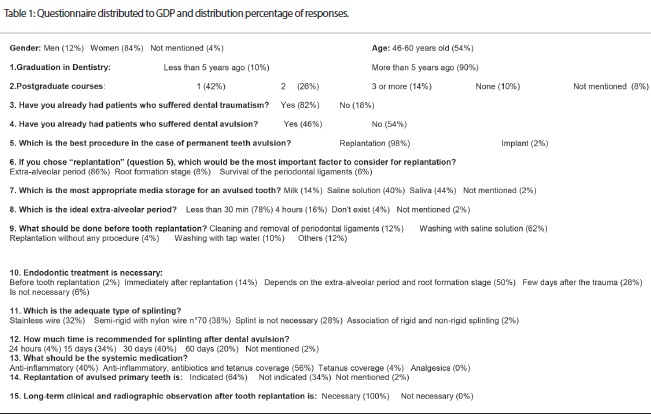
Objective: The purpose of this study was to evaluate dentists' knowledge about how to treat traumatic avulsion of teeth. Materials and methods: Seventy general dental practitioners who work in the public health service in João Pessoa, Brazil were interviewed using a questionnaire about their first-aid knowledge in dental traumatology with a particular focus on the following categories: general knowledge about tooth avulsion, replantation of primary and permanent teeth, how to clean an avulsed tooth before replantation, extra-oral time and storage media for an avulsed tooth. Descriptive statistics were used to describe and analyze the data. Results: Storage media for an avulsed tooth (saliva – 44%), type of splinting (semi-rigid – 38%), time of splinting (30 days – 40%) and replantation for avulsed primary teeth (64%). Conclusion: Strategies must be developed to enhance the level of knowledge general dental practitioners have so proper dental first-aid procedures can be achieved and treatment success rates of tooth avulsion can be increased.
KEYWORDS: Tooth avulsion; Tooth replantation; Tooth injuries.
RESUMO
Objetivo: O propósito deste estudo foi avaliar o conhecimento dos cirurgiões-dentistas de como tratar a avulsão dentária. Materiais e métodos: Setenta cirurgiões-dentistas que trabalham no serviço de saúde pública em João Pessoa, Brasil foram entrevistados usando-se um questionário sobre o conhecimento em tratar a avulsão dentária com um enfoque particular nas seguintes categorias: conhecimento geral da avulsão dentária, reimplante de dentes decíduos e permanentes, como tratar um dente avulsionado antes do reimplante, tempo extra-oral e meio de armazenamento adequado para um dente avulsionado. Os dados obtidos foram submetidos à estatística descritiva. Resultados: Meio de armazenamento adequado para um dente avulsionado (saliva - 44%), tipo de esplintagem (semi-rígido - 38%), tempo de esplintagem (30 dias - 40%) e reimplante de dentes decíduos avulsionados (64%). Conclusão: Estratégias devem ser desenvolvidas para aumentar o nível de conhecimento dos cirurgiões-dentistas com a finalidade de executar o pronto atendimento em procedimentos de primeiros socorros de forma precisa e para melhorar a taxa de sucesso do tratamento do dente avulsionado.
DESCRITORES: Avulsão dentária; Reimplante dentário; Traumatismos dentários.
Introduction
Dental traumatism has increased in recent years and it is related to an increase in sport activities and inadequate rescue protocol of accident victims1. Dental avulsion is the complete displacement of the tooth out of the alveolar socket, which can cause periodontal and pulp damage, such as pulp necrosis, periapical inflammation and root resorption2.
Replantation is the insertion of the tooth into the bony socket in its previous anatomical position. This conservative conduct preserves dental function and aesthetics and also postpones the urgency for prosthetic treatment. Also, it minimizes the psychological impact of dental loss in the patient and family3. However, the success of replantation depends on some factors, such as the extra-alveolar period and the storage media for the avulsed tooth, in order to maintain cell vitality. Additional treatments can be necessary, such as splinting and endodontic treatment3-5.
The purpose of this study was to investigate general dental practitioner (GDP) knowledge of dental avulsion management in João Pessoa, Brazil.
Material and Methods
Seventy GDP who work in public health service in the city of João Pessoa, Brazil were interviewed using a questionnaire about their knowledge about dental traumatology with particular focus on the following categories: general knowledge about tooth avulsion, replantation of primary and permanent teeth, how to clean an avulsed tooth before replantation, extra-oral time and storage media for an avulsed tooth. The questionnaire used in this study (Table 1) was a modified version of the questionnaire elaborated by Westphalen et al.6. The answers were registered at the moment of the interview. Descriptive statistics were used to describe and analyze the data. The study was approved by the Ethical Committee of Federal University of Paraíba, Brazil (Protocol 796/2006).
Results
NA total of 70 dentists answered the questionnaire. All respondents work in public health service in João Pessoa, Brazil. Twelve percent of the respondents were male and 84% female. The most frequent age groups were 46-60 years-old (54%). The results are summarized in Table 1.
Discussion
The study supports that treatment of tooth injuries is a common event in the dental practice. The vast majority of participants (82%) assisted patients with traumatic dental injuries. Tooth replantation has a low success rate (0.5% to 16%)3 and our study showed that most of the GDP had limited knowledge regarding some points in the protocol for avulsed tooth replantation: storage media, splinting techniques, time splint for the avulsed tooth and replantation of the avulsed primary tooth. The extra-alveolar period is the most essential factor to be considered in avulsion treatment3-5. In this study, 86% of the GDP affirmed that the extra-alveolar period was the most important factor when immediate replantation was not possible and saliva was the most appropriate storage media for avulsed teeth (44%), when a specialized medium was not readily available. Some studies have showed that milk, blood, Hank's Balanced Salt Solution (HBSS), Gatorade® and culture medium are other alternatives for storage media4,5,7. Saliva is a lightly hypotonic medium that can allow bacterial penetration into the dental fissures caused by traumatism. Bacterial contamination can cause pulp inflammation and establish root resorption8. HBSS is not available in Brazilian schools, so milk is a suitable storage medium for an avulsed tooth. Only about 14% of GDP opted for milk, which may be a better strategy for transporting the tooth due to composition and osmolality, when immediate replantation is not an option9. Mori et al.10 when assessing the conduct of teachers at Brazilian schools, found that milk would be the most recommended medium (84.61%) for storing the avulsed tooth when immediate replantation was not possible. Milk has physiologic pH, essential nutrients and few toxic components11.
Approximately two-thirds of the GDP (62%) affirmed that the debris should be removed from the dental surface using a physiological saline solution3. França et al.12 showed a different result in the city of Tubarão, in southern Brazil, in cases of a long extra-alveolar period. In our study, half of the GDP (50%) showed knowledge of the endodontic treatment indication, when the extra–oral time period and root stage formation were considered. Revascularization can occur when the avulsed tooth, which presents incomplete tooth formation, is soaked in an antibiotic solution and immediately replanted into the alveolus6,8. Revascularization has a low success rate when the apical foramen diameter is smaller than 1mm4. Thermal and electric pulp vitality tests can be performed after tooth replantation, where Laser Doppler flowmetry is considered the most effective13.
Splinting, systemic medication and follow-up must be observed. Ankylosis can be developed by the use of rigid splinting, which should be used only when there is socket wall fracture3,5,6. Several splinting techniques are recommended for stabilizing the replanted tooth, such as wire-composite, orthodontic bracket, resin splints and Titanium Trauma Splints (TTS)14. In this study, the rigid splint is suggested by 32% of GDP. Sixty percent of the GDP recommended 30 days or more as the appropriate splinting time. For most cases, a flexible splint of short duration, approximately 1 to 2 weeks, is thought to be in the patient's best interest with respect to hygiene and esthetics. Non-rigid fixation allowing physiologic tooth mobility has been shown to be desirable for periodontal healing14.
Patients who present immunological, congenital cardiac and mental disorders, as well as non controlled diabetes and lack of alveolar integrity should not get dental replantation15. Also, avulsed primary teeth should be not replanted because of damage in the permanent successor16. In our study, 64% of GDP recommended replantation of the avulsed primary tooth. Cohenca et al.2 reported that in their study 85.3% of participants did not recommend such a procedure. International Association of Dental Traumatology (IADT)17 guidelines do not recommend replanting avulsed primary teeth. Around 30% of the permanent successors presented some kind of injury after replantation of the avulsed primary tooth, such as discoloration, enamel hypoplasia, dilacerations and interruption of dental maturation18.
There were an estimated 5.9 million episodes of orofacial trauma care in the U.S. private practice sector in 1991. More than 4 million (68%) were seen by general dental practitioners19. Traebert et al.20 found a great number of patients who have already had traumatic dental injuries in Brazil and in our study, 82% of the GDP have already conducted treatment in patients who suffered traumatic dental injuries, where approximately half of the cases (46%) were related to dental avulsion. These results show that dental trauma has been increasing considerably in the recent years, facing it as a health public problem1,20.
Studies were published in an attempt to assess knowledge of dentists and non-dentists regarding diagnosis and therapy of traumatic dental injuries. Walker and Brenchley21 and Cohenca et al.2 showed that patients and their families lack treatment knowledge of avulsed tooth. Hu et al.22 showed that dentists selected from different parts of São Paulo, Brazil, have poor knowledge about dental avulsion and strategies must be developed in order to change this situation. The use of education campaigns has effective results in improving dentist and non-dentist knowledge regarding diagnosis and therapy of traumatic dental injuries. Informative campaigns about tooth avulsion are valid method alternatives, increasing success rates of tooth avulsion treatment and consequently promoting oral health10.
Conclusion
The results of our study show that GDP who work in public services in João Pessoa, Brazil have limited knowledge about tooth avulsion management. Educational campaigns based on Guidelines from the International Association of Dental Traumatism and, Brazilian Association of Dental Traumatism must be developed to improve GDP knowledge levels regarding diagnosis and therapy for tooth avulsion injuries so proper dental first-aid procedures can be appropriate.
References
1. American Association of Endodontists. Recommended guidelines for the treatment of traumatic dental injuries. Chicago: American Association of Endodontists; November 2004:1-6. [ Links ]
2. Cohenca N, Forrest JL, Rotstein I. Knowledge of oral health professionals of treatment of avulsed teeth. Dent Traumatol 2006; 22:296-301.
3. Andreasen JO, Andreasen FM. Textbook and colour atlas of traumatic injuries to the teeth. Copenhagen: Munksgaard; 1994.
4. Krasner P, Rankow H. A new philosophy for the treatment of avulsed teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:616-623.
5. Trope M. Clinical management of the avulsed tooth: Present strategies and future directions. Dent Traumatol 2002;18:1-11.
6. Westphalen VPD, Martins WD, Deonizio MDA, Silva Neto UXda, Cunha CBda, Fariniuk LF. Knowledge of general practitioners dentists about the emergency management of dental avulsion in Curitiba, Brazil. Dent Traumatol 2007;23:6-8.
7. Sigalas E, Regan JD, Kramer PR, Witherspoon DE, Opperman LA. Survival of human periodontal ligament cells in media proposed for transport of avulsed teeth. Dent Traumatol 2004;20:21–8.
8. Yanpiset K,Trope M. Pulp revascularization of replanted immature dog teeth after different treatment methods. Endod Dent Traumatol 2000;16:211-217.
9. Blomlöf L, Lindskog S, Andersson L , Hedstrom KG, Hammarström L. Storage of experimentally avulsed teeth in milk prior to replantation. J Dent Res 1983;62(8):912-916.
10. Mori GG, Castilho LR, Nunes DC, Turcio KHL, Molina RO. Avulsion of permanent teeth: analysis of the efficacy of an informative campaign for professionals from elementary schools. J Appl Oral Sci 2007;15(6):534-8.
11. Lee JY, Vann Júnior WF, Sigurdsson A. Management of avulsed permanent incisors: a decision analysis based on changing concepts. American Academy of Pediatric Dentistry - Pediatric Dentistry 2001;23(3):357-360.
12. França RI, Traebert J, Lacerda JT. Brazilian dentists' knowledge regarding immediate treatment of traumatic dental injuries. Dent Traumatol 2007;23:287-290.
13. Strobl H, Gojer G, Norer B, Emshoff R. Assessing revascularization of avulsed permanent maxillary incisors by laser Doppler flowmetry. J Am Dent Assoc 2003;103:1597-1603.
14. von Arx T, Filippi A, Buser D. Splinting of traumatized teeth with a new device: TTS (Titanium Trauma Splint). Dent Traumatol 2001;17:180-184.
15. American Academy of Pediatric Dentistry. Guideline on management of acute dental trauma. Chicago: American Academy of Pediatric Dentistry; 2005-2006: 135-142.
16. Zamon EL, Kenny DJ. Replantation of avulsed primary incisors:A risk–benefit assessment. J Can Dent Assoc 2001;67(7):386-389.
17. Flores MT, Malmgren B, Andersson L, Andreasen JO, Bakland LK, Barnett F, et al. Guidelines for the management of traumatic dental injuries. III. Primary teeth. Dent Traumatol 2007;23:196–202.
18. Christophersen P, Freund M, Harild L. Avulsion of primary teeth and sequelae on permanent successors. Dent Traumatol 2005;21:320-323.
19. Gift HC, Baht M. Dental visits for orofacial injury: defining the dentist's role. J Am Dent Assoc 1993;124:92–6.
20. Traebert J, Peres MA, Blank V, Böell RS, Pietruza JA. Prevalence of traumatic dental injury and associated factors among12-year-old school children in Florianópolis, Brazil. Dent Traumatol 2003;19:15-18.
21. Walker A, Brenchley J. It's a knockout: survey of the management of avulsed teeth. Accident and Emergency Nursing 2000;8:66-70.
22. Hu LW, Prisco CRD, Bombana AC. Knowledge of Brazilian general dentists and endodontists about the emergency management of dento-alveolar trauma. Dent Traumatol 2006;22:113-117.
 Endereço para correspondência: Julierme Ferreira Rocha
Endereço para correspondência: Julierme Ferreira Rocha
Department of Oral and Maxillofacial Surgery – School of Dentistry
Federal University of Campina Grande Rodovia Patos
Teixeira, km 1 – Santa Cecília Patos/PB Cep: 58700-970
Recebido para publicação: 29/11/11
Aceito para publicação: 08/11/12
