










Serviços Personalizados
Artigo
 pdf em Espanhol
pdf em Espanhol Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.12 no.1 Recife Jan./Mar. 2013
RELATO DE CASO / CASE REPORT
Ectopic eruption of lower lateral incisors: initial treatment with removable appliance – case report
Erupção ectópica de incisivos laterais inferiores: tratamento inicial com aparelho removível – relato de caso
Andressa Milholo CoelhoI
I Cirurgiã-Dentista; Especialista em Ortodontia pela Universidade de Itaúna
ABSTRACT
The aim of this article was to present an alternative to the treatment of lower lateral incisors with ectopic eruption using a removable appliance with digital springs. The treatment showed the efficacy of this appliance in the clinical case reported – early stage of mixed dentition – avoiding the development of a dental transposition and making the final stages with fixed appliance easier.
KEYWORDS: Lower lateral incisor. Ectopic eruption. Mixed dentition. Removable appliance.
RESUMO
O objetivo deste artigo foi apresentar uma alternativa de tratamento para correção de incisivos laterais inferiores com erupção ectópica através do uso de aparelho removível com molas digitais. O artigo demonstrou a eficácia deste tipo de aparelho no caso clinico apresentado – estágio precoce da dentadura mista – evitando o estabelecimento de uma transposição dentária e facilitando a finalização do caso com o uso de aparelho ortodôntico fixo.
DESCRITORES: Incisivo lateral inferior. Erupção ectópica. Dentadura mista. Aparelho removível.
Introduction
During the mixed dentition, significant teeth alterations can be observed. These alterations may affect occlusion development. Ectopic eruption and transposition are some of the disturbances observed in this period. Ectopic eruptions occurs when the natural sequence of eruption is altered, leading to teeth transpositions in extreme cases1.
Transposition is a positional anomaly of the teeth which is described as a positional interchange of two adjacent teeth. Also, a tooth development or eruption in a position normally occupied by a non-adjacent tooth may cause transpositions2,3. Amongst all the possibilities of transpositions, the mandibular lateral incisor-canine transposition is the rarest, affecting only 0.03% of the cases, showing a clear preference to women2,4,5. Unilateral transpositions have been reported more frequently than bilateral transpositions, and the left side has been involved more often than the right side. Interchange in position of the developing tooth buds, lack of the deciduous teeth root resorption, and mechanical interferences to the erupting permanent teeth are commonly correlated with transpositions6,7. Genetic heritage, trauma and bone pathologies are also accepted as etiologic factors in the development of transpositions3,8.
Transposition in the mandible is typically a result of distal migration of the mandibular lateral incisor6,9, and they can be classified as complete or incomplete. In a complete transposition case, both crowns and roots of the involved teeth are in a transposed position, whereas in an incomplete transposition only the crowns are transposed, and the root apices remain in a normal position5,6,7.
Early detection and diagnosis plays an important role in ectopic eruption. When the transposition is prematurely discovered, orthodontic correction can be attempted4, which can also avoid root resorption of adjacent teeth10. The three main clinical findings observed in the early stages of the mandibular lateral incisor ectopic eruption are: distal tipping, coronal displacement and severe mesiolingual rotation. At this point, in order to avoid a mandibular lateral incisor - canine transposition, an interceptive procedure is important to achieve teeth aligning in their correct positions5. However, if the transposition is already present in the beginning of the treatment, simple teeth alignment in their current transposed position is preferred. Dramatic teeth movement carries a higher risk of damaging the teeth and supporting structures5,7.
In the present work, a mandibular lateral incisive canine transposition was avoided by using a removable appliance with digital springs, followed by fixed appliance.
Case Report
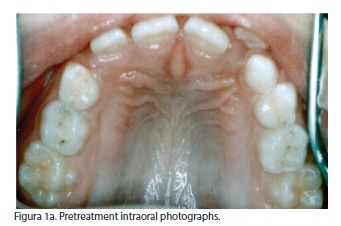
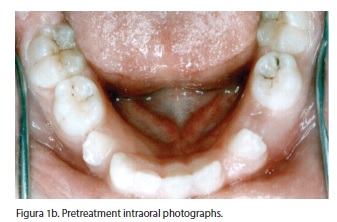
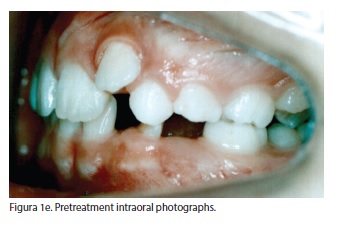
An eight years girl was referred by her clinical dentist to orthodontic treatment due to the ectopic eruption of the permanent mandibular lateral incisors. Clinical examination showed a patient in the early mixed dentition stage with a Class II dental relationship, a 3.0 mm overjet and a 3.5 mm overbite. The mandibular dental midline was deviated 3.5 mm to the left of the maxillary dental and facial midlines. The primary mandibular right canine and lateral incisive were not exfoliated.
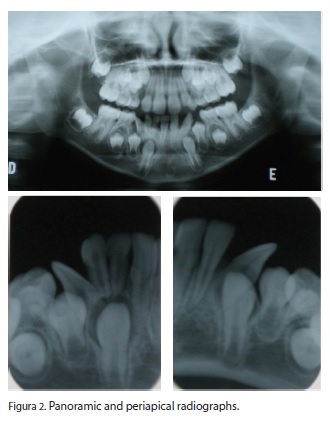
The analyze of dental casts, intraoral photographs (Figures 1a, 1b, 1c, 1d, 1e), panoramic and periapical radiographs (Figure 2) and lateral cephalometric radiograph revealed that first mandibular pre molars and permanent canines were impacted by the severe inclination of the mandibular lateral incisors. According to this, a treatment plan was made to avoid a dental transposition, allowing the eruption of the impacted teeth.


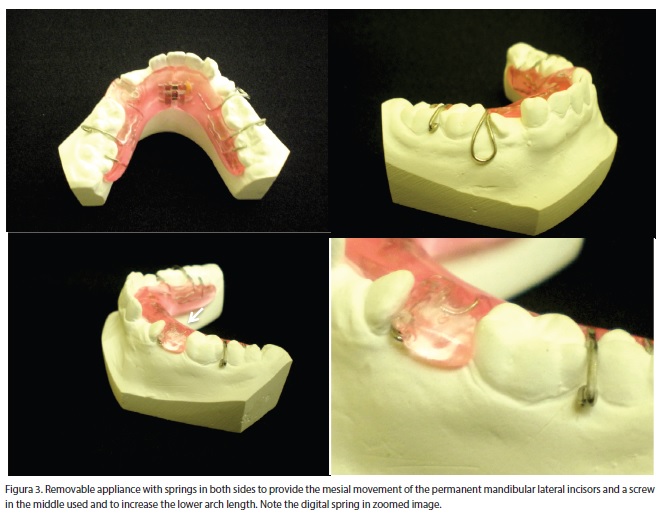
Primary lower right lateral incisor and canine were surgically extracted before the beginning of the treatment in order to increase the space for the alignment of the permanent lateral incisor and to correct the mandibular dental midline. After the extractions, a removable appliance with springs in both sides and a screw in the middle (Figure 3) was used to provide the mesial movement of the permanent mandibular lateral incisors, allowing the eruption of the first mandibular pre molar and canine, bilaterally. The screw was used to increase the lower arch length. The patient was monthly scheduled for recall appointments. Activations of the springs were made for a period of ten months and six activations of ¼ turn were made in the screw.
Concomitant with the use of the removable appliance, the patient used a high-pull headgear appliance. This appliance was used overnight (eight hours/ day), for fifteen months and with a 300g charge in both sides. The headgear was used to correct the dental Class II and to provide enough space for the eruption of the upper permanent canines.
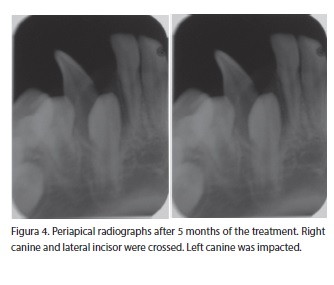
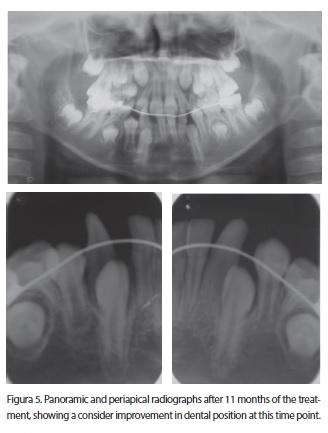
Follow-up periapical and panoramic radiographs were performed to evaluate the movement of the mandibular permanent lateral incisors and their relationship with the adjacent teeth. After five months of treatment, right canine and lateral incisor were still crossed and the left canine was impacted, as shown by periapical radiographs (Figure 4). After ten months using the removable appliance, the permanent lateral incisors were closer to the central incisors. At this time, the treatment with the removable appliance was interrupted and a lingual arch was used to maintain the dimensions of the mandibular arch. After eleven months, follow-up panoramic and periapical radiographs were performed (Figure 5), showing a satisfactory result at this time point. Three months after the installation of the lingual arch, a lower fixed appliance was used to get the proper alignment and leveling and to provide space for the eruption of the lower pre molars and canines.
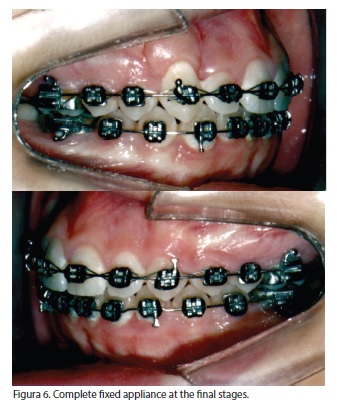
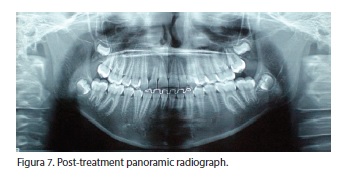
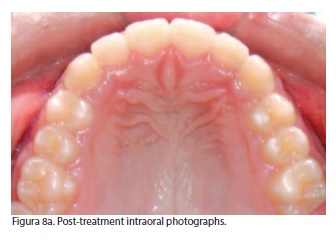
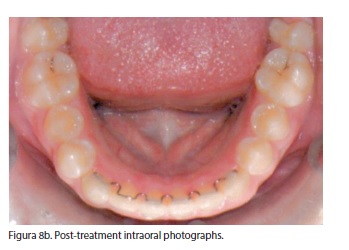
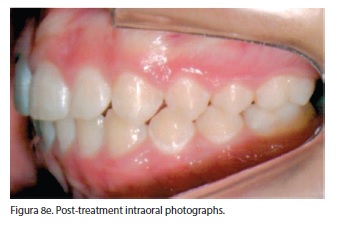
The case was finished with a complete fixed appliance (lower and upper) to get the correct alignment of the teeth and to get a good intercuspidation and occlusion (Figure 6). The final result was functionally (Figure 7) and esthetically (Figures 8a, 8b, 8c, 8d, 8e) satisfactory. Total treatment was completed in 48 months and was followed by placement of a maxillary Hawley retainer and a lingual-bonded canine-to-canine retainer.


Discussion
Lateral incisor-canine transpositions are rare, mainly in the mandible, where the high density of bone might difficult tooth transposition3,4,11,12. When this type of transposition occurs, it is often associated with a distal migration of the mandibular lateral incisor4,13. In this case report, distal migration of the mandibular lateral incisors was presented in both sides, although most studies reported higher frequency of unilateral transpositions2,3,6,14. Here, a bilateral lateral incisor – canine transposition was avoided by early diagnosis and treatment.
Early beginning of the interceptive treatment may have significant impact on malocclusion management. This may be especially important in displaced mandibular permanent lateral incisors cases4,6,9. Treatment is based on removing the retained mandibular primary teeth and guiding the ectopic mandibular lateral incisors to their correct places in the arch9. According to previous studies, primary canines have often been found to be over retained in the majority of the transposition cases, indicating that this might be the main etiological factor for mandibular teeth transpositions2,3,15. In this study, the primary lower lateral incisor and canine, both in the right side, were over retained. Before the beginning of the treatment with the removable appliance, the retained teeth were surgically extracted, with the purpose to get space for the alignment of the permanent lateral incisor and to correct the mandibular dental midline.
There are three main options for the transposition treatment: alignment of the involved teeth in their transposed position, extraction of one of the transposed teeth or a complete orthodontic correction to their normal anatomic positions. In general, for the best esthetics and optimal function, it is preferable to move the transposed teeth into their correct positions in the arch. However, even if the orthodontic approach is possible, treatment may be contraindicated due to time and biological limitations6,7. If the transposition is already present in the beginning of the treatment, simple teeth alignment in their current transposed position is preferred5,9.
In this case report, the interceptive use of a removable appliance with springs prevented the transposition of the mandibular lateral incisors and canines and allowed the eruption of the impacted pre-molar. At the final stages, fixed appliance provided the correct teeth alignment and a functionally and esthetically occlusion.
Conclusions
Early detection and diagnosis plays an important role in ectopic eruption. This patient was diagnosed in the early mixed dentition, and interceptive orthodontic treatment with removable appliance prevented the mandibular lateral incisor and canine transposition. There were benefits of early recognition and treatment of this malocclusion: the mandibular teeth were moved to their correct positions, the symmetry and harmony of the dental arch were achieved and sufficient space for the eruption of the lower pre molars and canine was created. At final stages, by using a fixed appliance, canine guidance was created for lateral mandibular movements in a functional Class I occlusion and a good esthetics was obtained.
References
1. Saldarriaga J R, Patiño M C. Ectopic eruption and severe root resorption. Am J Orthod Dentofacial Orthop, 2003; 123: 259-65. [ Links ]
2. Peck L, Peck S, Attia Y. Maxillary canine - first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod, 1993; 63(2): 99-109.
3. Celikoglu M, Miloglu O, Oztec O. Investigation of tooth transposition in a non-syndromic Turkish anatolian population: Characteristic features and associated dental anomalies. Med Oral Patol Oral Cir Bucal, 2010 Sep 1; 15 (5): e716-20.
4. Doruk C, Babacan H, Biçakçi A. Correction of a mandibular lateral incisor – canine transposition. Am J Orthod Dentofac Ortho, 2006; 129: 65-72.
5. Canoglu E, Kocadereli I, Turgut M D. Alignment of transposed mandibular lateral incisor and canine using removable appliances. Australian Dental Journal; 2009; 54: 266–270.
6. Shapira Y, Kuftinec M M. A unique treatment approach for maxillary canine -lateral incisor transposition. Am J Orthod Dentofac Orthop, 2001; 119: 540-5.
7. Borba D P, Barzotto C L, Orlando F, Woitchunas D. Irrupção ectópica de incisivo lateral inferior - relato de caso. RFO, set/ dez 2008; 13 (3): 78-82.
8. Asensi J. C. Mixed unilateral transposition of a maxillary canine, central incisor, and lateral incisor. Am J Orthod Dentofacial Orthop, 2010; 137: S141-53.
9. Deepti A, Rayen R, Jeevarathan J, Muthu MS, Rathna PV. Management of an impacted and transposed maxillary canine. J Indian Soc Pedod Prev Dent, 2010; 28: 38-41.
10. Becktor K B, Steiniche K, Kjaer I. Association between ectopic eruption of maxillary canines and first molars. European Journal of Orthodontics, 2005; 27: 186-189.
11. Ely N J, Sherriff M, Cobourne M T. Dental transposition as a disorder of genetic origin. European Journal of Orthodontics, 2006; 28: 145-151.
12. Peck S, Peck L, Kataja M. Mandibular lateral incisor canine transposition, concomitant dental anomalies and genetic control. Angle Orhod, 1998; 68(5): 455-66.
13. Shapira Y, Kuftinec MM. Tooth transposition: a review of the literature and treatment considerations. Angle Orthod, 1989; 59: 271-6.
14. Plunkett D J, Dysart P S, Kardos T B, Herbison G P. A study of transposed canines in a sample of orthodontic patients. British Journal of Orthodontics, 1998; 25: 203-208.
15. Yilmaz HH, Türkkahraman H, Sayin MO. Prevalence of tooth transpositions and associated dental anomalies in a Turkish population. Dentomaxillofac Radiol, 2005; 34: 32-5.
 Endereço para correspondência: Universidade Federal de Minas Gerais – UFMG
Endereço para correspondência: Universidade Federal de Minas Gerais – UFMG
Faculdade de Odontologia - Departamento de Odontologia Restauradora
Av. Antônio Carlos, 6627 – Pampulha. CEP: 31270-901
Belo Horizonte – MG – Brasil
e-mail: ortoandressa@oi.com.br
Recebido para publicação: 17/02/11
Aceito para publicação: 30/03/11
