










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.14 no.1 Recife Jan./Mar. 2015
Relatos de Caso / Case Reports
MANAGEMENT AND RADIOGRAPHIC FEATURES OF A RARE CONDITION: REGIONAL ODONTODYSPLASIA IN PRIMARY AND PERMANENT TEETH
Manejo e características radiográficas de condição rara: odontodisplasia regional em dentes decíduos e permanentes
Tatiana Kelly da Silva Fidalgo I; Andrea Quirino II; Paulo Ricardo Barros de Campos III; Laura Salignac Guimarães Primo IV
I PhD student, Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro
II Expert in Pediatric Dentistry, Pediatric Dentistry of Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro
III Expert in Operative dentistry, Department of Clinic, School of Dentistry, Federal University of Rio de Janeiro
IV Adjunct Professor, Pediatric Dentistry of Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro
ABSTRACT
Regional odontodysplasia is a rare and significant dental malformation. The present report describes an unexpected radiographic finding of rare tooth developmental anomaly and conservative management of primary teeth with in a child in mixed dentition. A 5-year-old healthy girl was referred to the Pediatric Dental Clinic due to pain and periapical radiograph exam showed teeth with abnormal large pulp chambers and a thin enamel and dentin of the primary incisors and canine and abnormal germs of the permanent successors teeth, with 'ghost-like' appearance. In addition, no root formation or only an insignificant amount was visible, characterizing regional odontodysplasia. At 10 years old, the treatment plan consisted of rehabilitation with a provisory partial resinous fixed prosthesis until implant surgery. The girl is still being followed up periodically.
Key words: Regional odontodysplasia, Pediatric Dentistry, Pathology.
RESUMO
A odontodisplasia regional é uma importante e rara malformação dental. O presente relato descreve um achado radiográfico inesperado de uma anomalia de desenvolvimento rara e seu manejo conservador em uma criança em dentição mista. Uma menina de 5 anos de idade, saudável, foi encaminhada à Clínica de Odontopediatria devido à dor. O exame radiográfico periapical mostrou os elementos dentários com câmaras pulpares amplas e uma fina camada de esmalte e dentina nos incisivos decíduos e anomalia nos germes dentários dos caninos permanentes sucessores, com aparência de 'dente-fantasma'. Além disso, não havia formação de raízes ou apenas uma quantidade insignificante era visível, caracterizando a odontodisplasia regional. Aos 10 anos, o plano de tratamento consistiu na reabilitação provisória por meio de uma prótese parcial fixa de resina até a cirurgia de implante ser possível. A criança, ainda, se encontra em acompanhamento periódico.
Descritores: Odontodisplasia regional, Odontopediatria, Patologia.
INTRODUCTION
Regional odontodysplasia (RO) is a very uncommon developmental anomaly which affects unilaterally contiguous teeth in both primary and permanent dentition causing severe dental, growing and craniofacial development anomalies.1,2 The etiology of this dental anomaly is unknown, although several factors, such as local trauma or infection, teratogenic drugs, local circulatory disorders, Rh incompatibility, irradiation, neural damage, hyperpyrexia, metabolic and nutritional disorders and vitamin deficiency have been discussed.2 It seems to be non-inherited condition as no cases of affected family members have been described.3 It has been suggested that RO is slightly more frequent in females and its incidence does not tend to be higher in any particular ethnic group.2,3
The criteria for RO diagnosis is based on clinical, radiographic, and sometimes supplemented by histologic findings.4 Clinically, RO can affect the primary and permanent dentition in either the maxilla, the mandible or both.1,5,6 Although the condition usually only affects one quadrant, cases with bilateral or multiquadrant involvement have been also reported.5 The number of affected teeth is variable and they are usually in a continuous series. The most commonly affected teeth are the central and lateral incisors, and canines.7
The treatment is still controversial, most dentists elect to extract the teeth involved immediately and later rehabilitate the patient with a temporary removable partial acrylic dental prosthesis until they reach the ideal age for dental implants.8 Although, an important question to be considered is the management in mixed dentition due to pre-pubertal period.6 The aim of the treatment should include improving function and esthetics, reducing the psychological impact of absent successor permanent teeth and facilitating normal jaw growth. Thus, the present report describes an unexpected radiographic finding of rare tooth developmental anomaly and conservative management of primary teeth with in a child in mixed dentition.
CASE REPORT
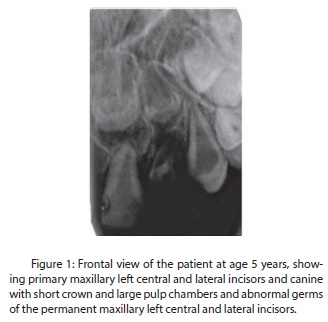
A 5-year-old healthy girl was referred to the Pediatric Dentistry Clinic with a complaint of pain due to a failure in pulp therapy procedure in the primary maxillary left lateral incisor. According to her mother, she had suffered a trauma when she was 2 years old. Intraoral examination revealed a primary dentition period. The periapical radiograph exam (Fig. 1) showed abnormal large pulp chambers and a thin enamel and dentin of the primary maxillary left central and lateral incisors and left canine and abnormal germs of the permanent maxillary left central and lateral incisors and canine, with 'ghost-like' appearance suggesting RO. The treatment plan was the extraction of the primary maxillary left lateral incisor under local anesthesia.
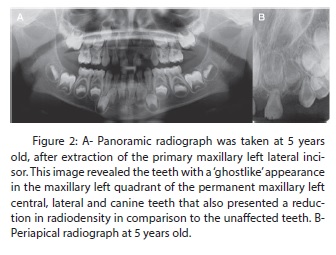
After the diagnostic of the unexpected radiographic finding, other radiographic images were done in order to evaluate the others primary teeth and permanent dental buds. A panoramic radiograph (Fig. 2A) and a new periapical (Fig. 2B) radiography confirmed the abnormalities of the primary teeth and also revealed the formation of anomalous germs of the permanent maxillary left central, lateral and canine teeth. These teeth showed a reduction in radiodensity in comparison to the unaffected ones. All the primary teeth and the germs of the permanent teeth in the right maxillary quadrant and mandible presented normal appearance. The crowns of the affected teeth were surrounded by large radiolucent areas, probably representing enlarged dental follicles. Radiographically there was no root formation or only an insignificant amount was visible of the affected teeth.
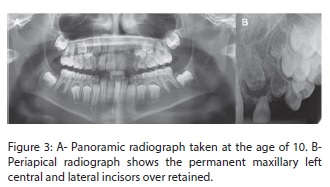
The child was followed-up for 5 years. At 10 years old, a new panoramic radiograph (Fig. 3A) and periapical (Fig. 3B) radiography were done revealing a slight development of permanent buds. The permanent maxillary right central and lateral incisors erupted, she complained about her appearance (Fig. 4A, B). Her mother reported that she presented difficulties in relationship due to the absence of the permanent left central incisor.
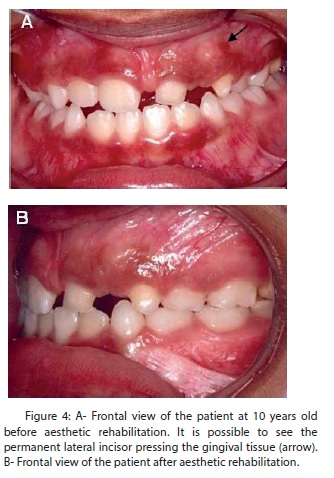
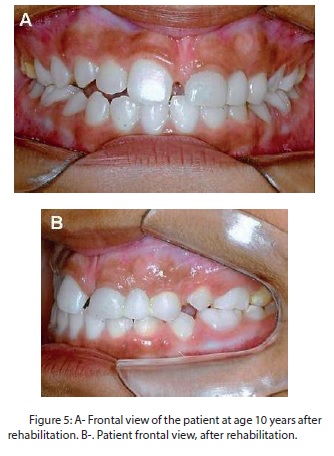
Rehabilitation with a provisory partial resinous fixed prosthesis was made (Fig. 5A, B) on primary left central incisor and canine to improve esthetics, function, and phonation until implant surgery. Since the primary teeth presented reduced measurements and expulsive shape, it was not necessary to use rotary cutting instruments, it was opted for conservative procedures. A complete arch (maxillary and mandibular) impression was made with condensation silicone material (Coltène, Vigodent, Rio de Janeiro, RJ, Brazil) and a master cast was obtained. A retentive metallic substructure was then manufactured. At the initial insertion trial, complete seating of the dental prosthesis, marginal adaptation of each retainer, tissue contact and form of the pontic, and occlusion were assessed. Subsequently, premature contacts of the primary central incisor and canine were eliminated and the shade of the lateral pontic was determined and recorded.
The color selection was carried out under natural light on a sunny day and with wet teeth. After color determination it was performed the laboratorial phase that consisted on application of the laboratorial microhybrid resinous system (SinfonyTM, 3M ESPE, CA, USA). The fixed prosthesis and the teeth were submitted to conditioning procedures, adhesive and dual-polymerizing resin cement (RelyxTM, 3M ESPE, CA, USA) was used.
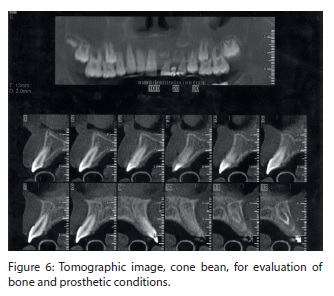
Oral hygiene instructions and dietary advice were given. A tomographic image (cone bean) was also performed (Figure 6) for evaluation bone condition and prostetic procedure. Her mother was informed of the need for an extensive follow-up. The girl has been followed up periodically (each 3 months) to observe if the "affected teeth" will erupt and to monitor the growth and development of the maxillary arch.
DISCUSSION
The etiology of RO is still unknown although some possible causes have been suggested.2,3 No hereditary pattern has been demonstrated; although the etiology is unclear, the dysplasia appears to be a local developmental abnormality that originates in pre-natal life. In the present case, the diagnostic of RO was a radiographic finding, since the main complaint was pain. The local etiologic factors could not be identified and no systemic involvement was seen. Although the child reported a local trauma when she was 2 years old, the primary incisors had already developed anomalously and the periapical infection due to failed pulpectomy was restricted to the primary maxillary left central incisor. For these reasons it was believed that in the present case local trauma and infection were not responsible for the malformation of the teeth. Packota et al1 reported that the disorder most likely occurs in the utero, at birth or in early infancy. Jones and Ford9 proposed that these types of mesoectodermal dysplasias might result from the mutation of a progenitor cell early in embryogenesis. Although in the current case no other disturbances were seen in the mesoectodermal tissue.
Delayed eruption or the non eruption of permanent teeth is a common finding in RO. A prevalence of 75% of the cases exhibit a decreased size of the maxillary sinus and alveolar bone on the affected side.10 The primary teeth present altered root structure with short roots and irregular root resorption. In the present case, the maxillary bone of the affected side was thinner than the other side. Also shorter roots of the primary anomalous teeth were observed.
Treatment of RO has given rise to controversy and there is no general agreement on the best treatment for these patients.4,11 Dentists should consider such factors as the patient's age, medical history, degree of involvement, the presence or absence of pathogenesis and the attitude and expectations of the child and parents.1,4,6 If a decision is made to retain the anomalous teeth, regular reviews are mandatory and an ideal dental treatment plan should be made for the patient. In the present case, the treatment adopted consisted of a partial resinous fixed prosthesis without extraction of the ghost teeth in order to reestablish aesthetics and functions without surgical procedures.1,7 The management adopted here is a temporary treatment, since this patient will be submitted to an implant treatment in the future. The choice of the treatment was based on the esthetic complaint of the adolescent patient.
This work describes a new approach to improve the esthetics of a patient in mixed dentition. Despite RO, the patient presented a harmonious development of teeth and superior and inferior arch relationship that was favorable for the choice of a fixed dental prosthesis. The treatment plan considered the dynamics of mixed dentition, the constant exfoliation and eruption characteristic of this dentition stage, allowing the development of the arches.2,3,11 The management was considered conservative since we preserved both affected primary and permanent successors. The main aim of the treatment was to perform rehabilitation during mixed dentition, recover aesthetics and provide space maintenance and satisfactory condition for future implant rehabilitation.11
Early recognition of the condition will reassure concerned parents and can provide the primary care needed.11 Diagnostic confirmation should be based on clinical and radiographic findings to rule out similar unilateral hyperplasia.12-15 In these cases, the treatment of choice should be personalised. In addition, parents should be made aware of the need for an extensive follow-up.6 The present paper presented a case of conservative management of RO in a child in mixed dentition. The treatment of choice allows the reestablishment of aesthetic and function during mixed dentition without influencing the development of the arches and recovering self-esteem and social reintegration.
REFERENCES
1. Packota GV, Pharoah MJ, Petrikowski CG. Radiographic features of segmental odontomaxillary dysplasia: a study of 12 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:577-584. [ Links ]
2. Pinkham JR, Burkes EJ, Jr. Odontodysplasia. Oral Surg Oral Med Oral Pathol 1973;36:841-850.
3. Crawford PJ, Aldred MJ. Regional odontodysplasia: a bibliography. J Oral Pathol Med 1989;18:251-263.
4. Gallo Cde B, Alves FA, Junior Ddos S, Marques MM, Sugaya NN. Regional odontodysplasia: management of an acute case with a scanning electron microscope. Gen Dent 2011;59:e178-181.
5. Lustmann J, Klein H, Ulmansky M. Odontodysplasia. Report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol 1975;39:781-793.
6. Barberia E, Sanz Coarasa A, Hernandez A, Cardoso-Silva C. Regional Odontodysplasia. A literature review and three case reports. Eur J Paediatr Dent 2012;13:161-166.
7. Gomes MP, Modesto A, Cardoso AS, Hespanhol W. Regional odontodysplasia: report of a case involving two separate affected areas. ASDC J Dent Child 1999;66:203- 207, 155.
8. Kahn MA, Hinson RL. Regional odontodysplasia. Case report with etiologic and treatment considerations. Oral Surg Oral Med Oral Pathol 1991;72:462-467.
9. Jones AC, Ford MJ. Simultaneous occurrence of segmental odontomaxillary dysplasia and Becker's nevus. J Oral Maxillofac Surg 1999;57:1251-1254.
10. Drake DL. Segmental odontomaxillary dysplasia: an unusual orthodontic challenge. Am J Orthod Dentofacial Orthop 2003;123:84-86.
11. Ferguson F, Schlissel E, Kucine A, Alexander S, DeSantis A, Hendricks R et al. Long-term management of a child with regional odontodysplasia: a case report. Pediatr Dent 2009;31:346-349.
12. Ozer L, Cetiner S, Ersoy E. Regional odontodysplasia: report of a case. J Clin Pediatr Dent 2004;29:45-48.
13. Hamdan MA, Sawair FA, Rajab LD, Hamdan AM, Al-Omari IK. Regional odontodysplasia: a review of the literature and report of a case. Int J Paediatr Dent 2004;14:363-370.
14. Cho SY. Conservative management of regional odontodysplasia: case report. J Can Dent Assoc 2006;72:735-738.
15. Cahuana A, Gonzalez Y, Palma C. Clinical management of regional odontodysplasia. Pediatr Dent 2005;27:34-39.
 Endereço para correspondência:
Endereço para correspondência:
Rua Voluntários da Pátria, 190/403
Botafogo - Rio de Janeiro – RJ/Brazil
CEP: 22270-010
e-mail: lprimo@pobox.com
Recebido para publicação: 29/08/2013
Aceito para publicação: 17/07/2015
