










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkOdontologia Clínico-Científica (Online)
versão On-line ISSN 1677-3888
Odontol. Clín.-Cient. (Online) vol.15 no.2 Recife Abr./Jun. 2016
Artigos Originais/ Original Articles
PREVALENCE OF MALOCCLUSIONS IN DECIDUOUS DENTITION AND ITS RELATIONSHIP WITH SOCIOECONOMIC RISK, AGE, AND GENDER: A CROSS-SECTIONAL STUDY
PREVALÊNCIA DE MALOCLUSÕES NA DENTIÇÃO DECÍDUA E SUA RELAÇÃO COM RISCO SOCIOECONÔMICO, IDADE E GÊNERO: UM ESTUDO TRANSVERSAL
Valdeci Elias dos Santos JuniorI; Amistis Vieira Costa e SilvaII; Andrea Gadelha Ribeiro TarginoI; Mônica Vilela HeimerIII; Aronita RosenblattIII
I DDS. MSc PH.D.– Department of Pediatrics, Faculty of Dentistry, University of Pernambuco, Brazil
II DDS. MSc – Department of Pediatric Dentistry, University of Pernambuco, Brazil
III DDS.MSc. Ph.D. Professor of Pediatric Dentistry. Faculty of Dentistry, University of Pernambuco, Brazil
RESUMO
Contexto: um dos problemas bucais mais frequentes no mundo é má oclusão, interferindo no bemestar da população. Objetivo: Este estudo teve como objetivo avaliar a prevalência de maloclusões na dentição decídua das crianças brasileiras e sua relação com a idade, sexo e renda familiar. Métodos: 261 crianças de 3-6 anos de idade foram examinadas de acordo com os critérios estabelecidos pelas diretrizes da Organização Mundial de Saúde e as maloclusões foram avaliadas segundo os critérios de Foster & Hamilton. Um questionário validado foi aplicado para codificar as maloclusões e coletar informações sobre idade e renda familiar. O teste do qui-quadrado de Pearson foi usado para verificar as relações entre maloclusões e as variáveis analisadas. Resultados: A relação entre os caninos do tipo classe I representou 82,8% da amostra, seguido de Classe II com 9,2% e Classe III com 8%. Também foram detectadas sobressaliência (9,6%), mordida cruzada anterior (4,6%), mordida cruzada posterior (9,6%), aberta e mordida profunda (13,4%). No entanto, não foi encontrada associação estatisticamente significativa entre má oclusão e as variáveis analisadas: a idade (p = 0,359), sexo (p = 0,308) ou renda familiar (p = 0,405). Conclusão: A prevalência de má oclusão foi alta e não foi associada com renda familiar, idade ou sexo. É importante enfatizar que a intervenção ortodôntica precoce pode evitar repercussão na dentição permanente evitando tratamentos ortodônticos complexos e dispendiosos.
Palavras-chave: Ortodontia; Maloclusão; Epidemiologia; Saúde pública; Crianças.
ABSTRACT
Background: one of the most frequent oral problems in the world is malocclusion, interfering in the population welfare. Aim: This study aimed to assess the prevalence of malocclusions in deciduous dentition of the Brazilian children and its relationship with age, gender and family income. Methods: 261 children from 3-6 years old were examined according to the criteria established by the World Health Organization guidelines and the malocclusions were assessed following the criteria of Foster & Hamilton. A validated questionnaire was applied to verify the malocclusions and collect information about age and family income. The Pearson's chi-square test was used to verify the relationships between malocclusion and the variables analyzed. Results: Class I canine relationship represented 82.8% of the sample, followed by Class II with 9.2% and Class III with 8%. It was also detected overjet (9.6%), anterior crossbite (4.6%), posterior crossbite (9.6%), open and deep bite (13.4%). However, there was no statistically significant association between malocclusion and variables: age (p = 0.359), sex (p = 0.308) and family income (p = 0.405). Conclusion: The prevalence of malocclusion was high and was no associated with family income, age or gender. It is important emphasize that early orthodontic intervention can prevent repercussion in the permanent dentition avoiding complex and costly orthodontic treatments.
Keywords: Orthodontics; Malocclusion; Epidemiology; Public health; Children.
INTRODUCTION
Malocclusion is one of the problems most frequent oral health in the world, second only to dental caries and periodontal disease1. Due to its high prevalence is considered a public health problem of Brazilian population2. However, is possible to prevent and treat this alteration, avoiding the damage that may cause as a negative social impact by interfering with quality of life of the individuals affected, harming their social interaction and psychological wellbeing3.
The prevalence of malocclusion in Brazilian children is 35%, and there is a variation from one geographical region to another and northeast region has the highest prevalence4. Therefore, it is essential to monitor the distribution and severity of malocclusion in society and assess the relevant risk factors over time. Thus, the present study was designed to evaluate the prevalence of malocclusions in 3-6 year old of Brazilian children, and also establishes the relationship between gender, age and family income.
METHOD
This cross-sectional study was developed in the city of Recife, capital of Pernambuco, one of nine federal units that comprise the northeast region of Brazil. This study was conducted in full accordance with the World Medical Association Declaration of Helsinki. The research project was approved by the Ethics Committee in Research of the Pernambuco State University (Protocol: 044/2006).
The sample size was calculated using the Epi Info 7 and was based on previous data4. A sample error of 5%, and a confidence interval of 90% were adopted. The minimal sample size was determined to be 246 children from 3 to 6 years of age. However, 261 children were examined, exceeding the sample, in order to avoid possible data loss.
The children were examined by three calibrated examiners (Kappa=0.83) at the patio, under natural illumination. The examination followed the World Health Organization guidelines5. For assessing dental occlusion examiners used latex gloves, dental mouth mirrors and millimeter rulers.
The occlusion was assessed following the criteria of Foster & Hamilton6:
• Canine Relationship: Patients were classified according to canine relationship for classes I, II and III. However, children who presented class I were considered like normal occlusion.
• Anterior Open Bite: An AOB was recorded when there was lack of vertical overlap of more than 3 mm between the incisors with the posterior teeth in occlusion.
• Overjet (OJ): The distance from the incisal edge of the most protrusive maxillary central incisor to the most labial surface of the corresponding mandibular incisor, using a millimeter ruler, parallel to the occlusal plane. The overjet was considered increased when it was greater than 3mm.
• Deep bite: It was registered when the maxillary incisors on full closure covered more than two-third of the heights of the mandibular incisors.
• Anterior crossbite: Included subjects with reverse overjet.
• Posterior crossbite: A posterior crossbite was recorded when one or more of the maxillary teeth in the posterior segments occluded palatal to the buccal cusp of the opposing mandibular teeth. Posterior crossbite could be unilateral (right or left) or bilateral. It was considered malocclusion when the children presented at least one of these alterations.
The examiners administered a questionnaire, which was previously validated in a pilot study, to parents and guardians in order to obtain information on family income and age of children.
The data were statistically analyzed using the Statistical Package for Social Sciences Version 15.0 (SPSS Inc., Chicago, Illinois, USA). A descriptive and inferential statistics was performed, using Pearson's chi-square test at the 5% level of significance.
RESULTS
The sample consisted of 261 children, mean age 4.55 (SD = 1.09). The final sample comprised 139 males (53.3%) and 122 females (46.7%).
Class I canine relationship represented 82.8% of the sample, followed by Class II with 9.2% and Class III with 8%. An increased overjet was observed in 25 subjects (9.6%) and 4.6% of children had anterior crossbite. In the cases of open bite and deep bite, the prevalence was 13.4% for both. The posterior crossbite was present in 9.6% of the subjects.
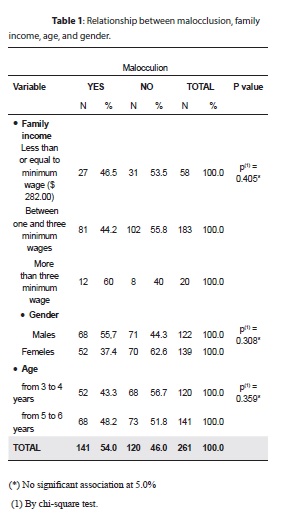
This study revealed that fifty-four percent of the children had at least one type of malocclusion. However, this prevalence was not shown to be related to low family income, age or gender (p > 0.05) (Table 1).
DISCUSSION
Malocclusion incidence seems to have accelerated in modern industrialized societies during the last century. Theories proposed to explain the cause of malocclusion vary widely, embracing concepts such as evolution, heredity and environmental factors7. Dental malocclusion can cause psychosocial problems related to dentofacial aesthetics and disturbances of oral function, such as mastication, swallowing, and speech8, greater susceptibility to trauma9 and periodontal disease10.
The orthodontic features of various populations have been the aim of several investigations in different countries11,12. An epidemiological survey is an essential tool in determining the prevalence and incidence of a given pathogen in a given population, and estimate treatment needs and provide information for planning of health services. The present study investigated children from 3 until 6 years old that are an age frequently considered as an optimal time to treatment of many of dentoesqueletal disharmonies13,14 and, this way, could benefit for early orthodontic intervention.
It was observed that 54% of sample evaluated presented, at least, one malocclusion. These findings are in agreement with the last national oral health survey conducted in Brazil (52.4%). However, it was lower than the date found in the northeast region (69.5%)4. This divergence between regions was reported by previous study15 when reviewed previous studies and found a variation from 40 to 93 per cent in the prevalence of malocclusion. These results suggested that, even those studies conducted in the same population show great variability that may be related to different among ethnic groups, age, diagnostic criteria used to classify malocclusion, differences in determining the boundaries of normal occlusion, and differences in sample sizes.
With regard canine relationship, these finding agree with previous studies that verified canine class I in the most of the sample4,16. However, the prevalence of class II was lower than studies realized in France17, Iran18, Israel19 and Italy20. As in the majority of the studies, canine class III represented the minor prevalence16-20.
Sucking habits, which differ between different populations, has been considered as a risk factor for the presence of posterior crossbite21. Although there is no evidence, at present, to support the routine correction of a posterior crossbite in the primary dentition22, some authors emphasize that spontaneous correction of this malocclusion rarely occurs
Anterior open bite and deep bite had the same prevalence (13.4%) that were similar to the results found in Tanzania and Brazil4,16. The most prevalent malocclusion found in the deciduous dentition is the anterior open bite, which decreases in prevalence with advancing age16-20. It has been shown that the main cause of this decrease is the cessation of a sucking habit during the primary dentition that cause the self-correction of an AOB21,23.
This study observed an increased overjet in 9.6% that was higher than verified in Iran (11.5%)18 and lower than in Italy (14.7%)20 and an epidemiological survey in Brazil (21%)4. Anterior crossbite was less prevalent malocclusion detected in 4.6% of children. This result was lower than found in Iran (8.4%)18 and Italy20 (15%). This result also was not compatible with the last National epidemiological research (3%)4.
In the present study the prevalence of malocclusion was not associated with family income, age or gender. These findings are in agreement with the literature that does not indicate an association between socioeconomic status and malocclusion in the deciduous dentition24.
Considering that the public health system in Brazil has no insufficient support for such demand for orthodontic treatments, sometimes complex, a viable solution would be to prioritize the care with the prevention, through of orientation, beside of early intervention, that show low complexity and lower cost.
CONCLUSIONS
The prevalence of malocclusion was high and was no associated with family income, age or gender. It is important emphasize that early orthodontic intervention can prevent repercussion in the permanent dentition and, this way, to avoid complex orthodontics treatment in the future that will be more expensive and difficult to access for the lowincome population.
COMPETING INTERESTS
For this study, there was no conflict of interest in: (1) the study design; (2) the collection, analysis and interpretation of data; (3) the writing of the report; and (4) the decision to submit the paper for publication.
REFERENCES
1. Marques CR, Couto GB, Orestes Cardoso S. Assessment of orthodontic treatment needs in Brazilian schoolchildren according to the Dental Aesthetic Index (DAI). Community Dent Health. 2007 Sep;24(3):145-8. [ Links ]
2. Marques LS, Pordeus IA, Ramos-Jorge ML, Filogônio CA, Filogônio CB, Pereira LJ, Paiva SM. Factors associated with the desire for orthodontic treatment among Brazilian adolescents and their parents. BMC Oral Health. 2009 Dec 18;9:34.
3. de Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004 Mar;31(1):20-7.
4. Brazil. Ministry of Health, Office of Health Care. Department of Primary Care. National Coordination of Oral Health. SB Brazil 2010 Project - Oral health status of the Brazilian population 2010: main results. Brasília (DF): MS-CNSB; 2010.
5. World Health Organization [homepage]. Geneva: World Health Organization; 2000 [17 Dec 2012]. Available at http://www.who.int/oral_health/strategies/en//
6. Foster TD, Hamilton MC.Occlusion in the primary dentition. Study of children at 2 and one-half to 3 years of age. Br Dent J. 1969 Jan 21;126(2):76-9.
7. Hassan R, Rahimah AK. Occlusion, malocclusion and method of measurements-an overview. Arch Orofac Sci 2007; 2: 3-9.
8. Kenealy P, Frude N, Shaw W. An evaluation of the psychological and social effects of malocclusion: some implications for dental policy making. Soc Sci Med. 1989;28(6):583-91.
9. Grimm S, Frazão P, Antunes JL, Castellanos RA, Narvai PC. Dental injury among Brazilian schoolchildren in the state of São Paulo. Dent Traumatol. 2004 Jun;20(3):134-8.
10. Geiger AM. Malocclusion as an etiologic factor in periodontal disease: a retrospective essay. Am J Orthod Dentofacial Orthop. 2001 Aug;120(2):112-5.
11. Brunelle JA, Bhat M, Lipton JA. Prevalence and distribution of selected occlusal characteristics in the US population, 1988-1991. J Dent Res. 1996 Feb;75 Spec No:706-13.
12. Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthod. 2001 Apr;23(2):153-67.
13. Abu Alhaija ES, Al-Khateeb SN, Al-Nimri KS. Prevalence of malocclusion in 13-15 year-old North Jordanian school children. Community Dent Health. 2005 Dec;22(4):266-71.
14. Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur J Orthod. 2004 Jun;26(3):237-44.
15. Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int J Paediatr Dent. 2004 May;14(3):155-66.
16. Mtaya M, Brudvik P, Astrøm AN. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren. Eur J Orthod. 2009 Oct;31(5):467-76. doi: 10.1093/ejo/cjn125. Epub 2009 Mar 31.
17. Tschill P, Bacon W, Sonko A. Malocclusion in the deciduous dentition of Caucasian children. Eur J Orthod. 1997 Aug;19(4):361-7.
18. Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. Malocclusion and occlusal traits in an urban Iranian population. An epidemiological study of 11- to 14-year-old children. Eur J Orthod. 2009 Oct;31(5):477-84. doi: 10.1093/ ejo/cjp031. Epub 2009 May 28.
19. Ben-Bassat Y, Harari D, Brin I. Occlusal traits in a group of school children in an isolated society in Jerusalem. Br J Orthod. 1997 Aug;24(3):229-35.
20. Perillo L, Masucci C, Ferro F, Apicella D, BacettiTPrevalence of orthodontic treatment need in southern Italian schoolchildren schoolchildren. Eur J Orthod. 2010 Feb; 32(1): 49-53.
21. Heimer MV, Tornisiello Katz CR, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008 Dec;30(6):580-5.
22. Abu Alhaija ES1, Al-Khateeb SN, Al-Nimri KS. Prevalence of malocclusion in 13-15 year-old North Jordanian school children. Community Dent Health. 2005 Dec;22(4):266-71.
23. Katz CR, Rosenblatt A, Gondim PP. Nonnutritive sucking habits in Brazilian children: effects on deciduous dentition and relationship with facial morphology. Am J Orthod Dentofacial Orthop. 2004 Jul;126(1):53-7.
24. Silvestrini-Biavati A, Migliorati M, Demarziani E, Tecco S, Silvestrini-Biavati P, Polimeni A, Saccucci M. Clinical association between teeth malocclusions, wrong posture and ocular convergence disorders: an epidemiological investigation on primary school children. BMC Pediatr. 2013 Jan 23;13:12. doi: 10.1186/1471-2431-13-12.
 Correspondência para:
Correspondência para:
Valdeci Elias dos Santos Junior
Rua São Sebastião 417 #101
CEP 54410500
Jaboatão dos Guararapes
PE Brazil
e-mail: valdeciodonto@gmail.com
Recebido: 27/07/2015
Aceito: 02/09/2016
