










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista da ABENO
versão impressa ISSN 1679-5954
Rev. ABENO vol.15 no.1 Londrina Jan./Jun. 2015
Dental students' performance and perceptions on canal preparation: a mixed methods study
Performance e percepções de estudantes de odontologia no preparo de canais: um estudo de métodos mistos
Alexandre Azevedo SallesI; Renata Grazziotin-SoaresII; Diego Machado ArdenghiIII; Rossano André Dal-FarraIV; Fernando Branco BarlettaI
I Professor, Department of Endodontics, School of Dentistry, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
II Professor, Department of Endodontics, School of Dentistry, Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil
III Clinical Assistant Professor, Department of Preventive and Restorative Dental Sciences, School of Dentistry, University of California at San Francisco (UCSF), San Francisco, CA, US
IV Professor, Department of Education, Universidade Luterana do Brasil (ULBRA), Canoas, RS, Brazil
ABSTRACT
This study explored dental students' performance (quantitative data) and perceptions (qualitative data) on canal preparation with Ni-Ti rotary vs. hand instruments and discussed interactions between technical findings and students' insights. A mixed methods design was used. Each student (n=20) instrumented two canals using hand K-files and two canals using ProTaper Universal® rotary Ni-Ti instruments. Participants had no previous experience with rotary instrumentation but were familiar with hand instrumentation. Quantitative data: apical transportation, working time for instrumentation and procedural errors were statistically analyzed. Qualitative data (students' perceptions) were collected and perceptions were identified from interview contents using thematic analysis. Lower level of apical transportation, fewer procedural errors (ledge/perforation/blockage), and a longer working time were associated with rotary instrumentation. Working time was shorter in the second canal instrumented with both techniques. Perceptions associated with hand in-strumentation were: better domain and practice/confidence due to the students being used to the hand technique. Ni-Ti rotary instrumentation perceptions were: good initial expectations before its use, perceptions of doubts and difficulties concerning workability right after its first use, and increase in confidence after its second use in a second canal. It was concluded that: (i) students show a cautious attitude towards rotary instrumentation; (ii) confidence increases after rotary instrumentation of the second canal; (iii) students show good expectations in terms of optimizing root canal treatment with rotary instrumentation and they think it would be possible after some training; and (iv) Ni-Ti rotary instrumentation should be included in the undergraduate curriculum of dental schools.
Descriptors: Dental education. Students' perception. Mixed methods research. Endodontics. Root canal shaping.
RESUMO
Este estudo explorou o desempenho dos estudantes de odontologia (dados quantitativos) e percepções (dados qualitativos) em relação ao preparo do canal com instrumentos rotatórios de Ni-Ti versus instrumentos manuais e discutiu interações entre os achados técnicos e os insights dos estudantes. O delineamento usado foi o de métodos mistos. Cada estudante (n=20) instrumentou dois canais usando instrumentos manuais e dois canais usando instrumentos rotatórios de Ni-Ti (ProTaper Universal®). Os participantes não tinham experiência com instrumentação rotatória, mas estavam familiarizados com instrumentação manual. Dados quantitativos, tais como transporte apical, tempo de trabalho para a instrumentação e erros de procedimento foram estatisticamente analisados. Dados qualitativos (percepções dos estudantes) foram coletados, sendo que as percepções foram identificadas a partir do conteúdo das entrevistas utilizando a análise temática. Baixos valores de transporte apical, poucos erros de procedimento (desvio/perfuração/bloqueio), e tempo de trabalho mais longo foram associados à instrumentação rotatória. O tempo de trabalho foi mais curto no segundo canal instrumentado por ambas as técnicas. Percepções associadas com instrumentação manual foram: melhor domínio e prática/segurança em virtude de os estudantes estarem acostumados com a técnica. Percepções para a instrumentação rotatória: boas expectativas iniciais, antes de utilizar; percepção de dúvidas e dificuldades em relação ao manejo do instrumento logo antes de utilizar; e, aumento da segurança na utilização depois do segundo uso, no segundo canal. A combinação dos achados quantitativos e qualitativos levou às seguintes conclusões: (i) os estudantes mostraram uma atitude de precaução frente à instrumentação rotatória de Ni-Ti; (ii) a segurança amentou depois da instrumentação do segundo canal; (iii) os estudantes mostraram expectativas boas em termos da otimização do tratamento de canal radicular com a instrumentação rotatória e pensam que isso será possível após algum treinamento; e (iv) a instrumentação rotatória com Ni-Ti deveria ser incluído no currículo de graduação das escolas de odontologia.
Descritores: Ensino odontológico. Percepção de estudantes. Métodos mistos de pesquisa. Endodontia. Preparo do canal radicular.
1 INTRODUCTION
Despite the proven superiority of nickel-titanium (Ni-Ti) rotary instruments in relation to the stainless steel hand technique to clean and shape root canals1,2, traditionally endodontic treatment has been performed with stainless steel hand files.3 Some authors have suggested that this gap between research and clinical practice probably reflects the fact that, very often, manual techniques continue to be taught at some dental undergraduate programs.4 Paradoxically, the well-known limitations of stainless steel hand endodontic instruments may contribute to the technical difficulties faced by students in the academic setting 5 and negatively impact their success rate in treating root canals during their practice both as students6 and also after graduation7.
Especially in developing countries, the unfavorable arguments against hand instrumentation techniques, added to a high demand of patients requiring root canal treatment8, should stimulate a solid incorporation of new technologies at the dental undergraduate level, aiming to improve student knowledge and consequently benefit the population. As reported by Molander et al.9, we can hypothesize that Ni-Ti rotary instruments could be safely prioritized in the undergraduate dental curriculum and could substantially improve the quality of root canal preparation, particularly when performed by inexperienced students. In this regard, authors have claimed that the scientific evidence available is not sufficient to justify the still prevailing opinion that dental students should become competent in the use of hand files before they start to use rotary files.10
The contributions of the literature focusing on Ni-Ti rotary root canal preparation are strongly based on anatomical considerations. The majority of scientific publications are in vitro studies that have described, for example, reduced levels of apical transportation11, as a result of the improved properties of Ni-Ti instruments12. In addition, some authors have addressed the relationship between the shaping ability of Ni-Ti instruments and operator's technical experience. In particular, over the past few years, a number of studies have shown that, when using Ni-Ti instruments, even novice operators can shape root canals at a lower risk of procedural errors, greater preservation of tooth structure, and a shorter working time when compared with hand instrumentation3,10,13,14. Despite the relevance of these data for the teaching-learning process in endodontics, the low level of evidence generated by in vitro studies precludes a direct ex-trapolation of findings to the clinical patient care setting. In addition, in the field of Ni-Ti rotary instruments, there is an evident disre-gard of dental students' opinions, neglecting their role as key elements in the construction of knowledge and in academic discussions15,16. In an attempt to give voice to students' views about academic topics, some studies have used the mixed methods approach17. This methodology is relatively new in dentistry, and it aims to combine quantitative and qualitative analyses to shed light on issues that cannot be unveiled using only statistical analysis. In qualitative research, the investigator has the possibility to interpret human subjectivity, trying to understand the subjects' expectations and feelings18. In this sense, the mixed methods approach provides strengths that offset the weaknesses of quantitative and qualitative research used alone19.
To date, the assessment of students' perceptions in relation to canal preparation performed with Ni-Ti instruments has been lacking5,13. In particular, to our knowledge, no mixed methods research has been published on the topic. Therefore, the aims of the present study were to assess instrumentation variables (students' performance, quantitative phase) and to explore students' perceptions (qualitative phase) on canal preparation with Ni-Ti rotary instruments in comparison with hand stainless steel instruments, using a mixed methods approach. Interactions between quantitative and qualitative data are discussed, with a focus on potential improvements for undergraduate dental education.
2 METHODS
2.1 Subject selection and study design
The study was approved by the local ethics committee. All subjects signed an informed consent form before their inclusion in the study. As part of the informed consent process, students were assured that their identities would remain anonymous, that participation was voluntary, and that participation or refusal at any time would not have any effect on their undergraduate dental program or grades.
All last-year dental students enrolled at a Brazilian Dental School were considered eligible and invited to participate. Among these, 20 students were randomly selected (from July to December 2012) to comprise the final sample. Student selection was performed as follows: each student who agreed to participate in the study received a number; these numbers were placed in an opaque, sealed envelope; 20 numbers were drawn and the correspondent student was contacted to participate in the study.
The present investigation used a mixed methods design. Quantitative data (apical transportation, working time required for instrumentation, and procedural errors) were collected after analysis of resin blocks simulating root canals that had been instrumented by the students. Qualitative data were collected through individual semi structured interviews conducted with the same students who participated in the quantitative phase.
The students attended a 1-hour theoretical lecture, delivered by the main investigator, where the study objectives were explained and the use of the electrical motor and Ni-Ti rotary instruments was taught. The participants had never been in contact with rotary instrumentation before. A demonstration of how to instrument the resin blocks simulating canals was conducted by the main investigator soon after the theoretical lecture, and the instrumentation protocol was given to each student in print. Hand instrumentation was not addressed in this lecture because all students were familiar with it, i.e., they had training with resin plastic blocks, extracted human teeth, as well as, working with patients in the clinical practice. Each student had completed the root canal treatment in 5 teeth, on average, previously to be included in this study.
2.2 Quantitative phase
The simulated canals used in this study had 40 degrees of curvature, 8 mm of radius and 18 mm of total length (10 mm straight and 8 mm curved). Each participant (n=20), individually, instrumented four simulated canals: two using manual stainless steel K-files (namely first and second-hand) and two using ProTaper Universal® rotary Ni-Ti instruments (namely first and second - Ni-Ti rotary). Firstly, two canals were instrumented with hand files and, after an interval of 20 minutes the two canals remaining were instrumented with rotary Ni-Ti instruments.
As a result, a total of 80 simulated canals were instrumented (40 hand and 40 Ni-Ti rotary). Sample size was based on a previous study that investigated anatomical features of root canals in vitro.11
Canal Instrumentation
Plastic blocks canals were instrumented under constant irrigation/aspiration with 2.5% sodium hypochlorite. Canal negotiation was performed using a #10 manual K-file. Working length was determined using the visual method, i.e., 1 mm shorter of the end of the canal. For hand instrumentation, the crown-down technique was adopted, starting with a #45 hand K-file on the cervical third and preparing the canal to working length up to a #30 K-file (master file), according to the technique proposed and currently used in the university's curriculum. Rotary instrumentation was performed using the ProTaper Universal® system. Ni-Ti instruments were mounted on an E6AR handpiece (NSK, Tokyo, Japan) attached to an Endo Pro-Torque motor (Driller, São Paulo, Brazil) at 300 rpm and 2 N.cm torque. ProTaper Universal® S1 and Sx instruments were advanced into the straight part of the canal. Subsequently, root canals were instrumented to working length using the ProTaper Universal® instruments in the following sequence: S1, S2, F1, F2, and F3.
Apical Transportation
Plastic blocks canals were photographed before and after instrumentation. To ensure consistent photographs, an L-shaped wooden platform was manufactured and allowed positioning the canal perpendicular to the camera (Canon XS 1000D, Melville, NY, USA). Images were obtained in both buccolingual (BL) and mesiodistal (MD) projections for each canal, resulting in a total of 320 images (160 before and 160 after instrumentation). Each image received a code containing information on instrumentation status (before or after instrumentation), student number (from 1 to 20), instrumentation technique (hand or Ni-Ti rotary), and preparation sequence (first or second canal instrumented). Images were transferred to a computer and stored in JPEG format.
Pairs of images of the same canal were superimposed using Adobe Photoshop version 7.0 (Adobe Systems, Seatlle, USA). Layers were created, the image corresponding to the instrumented canal was colored, and its opacity reduced. At 1, 2, 3, and 4 mm from the end of the canal, the ruler tool was used to measure the distance, in millimeters, between the two outer limits of the canal wall, in both BL and MD projections. Apical transportation was measured independently by two examiners blind to instrumentation technique and was defined as the difference in mm between the instrumented canal and the anatomical canal for each side of the curvature. A zero value meant absence of transportation.
Working Time Required for Instrumentation
Time required to complete instrumenta-tion was recorded for each simulated canal by the main investigator. Time required for instrument change and irrigation was also included in the total time.
Procedural Errors
Procedural incidents, such as ledges, blockages, perforations, and instrument fractures, were independently recorded by the same examiners who assessed apical transpor-tation.
2.3 Qualitative phase
Before the beginning of this phase, guiding interview questions were created and applied to two dental students to assess the convenience and applicability of the questions and to validate them. Following this pilot test, one-on-one, face-to-face semi-structured interviews (n=20) were conducted by the main investigator, lasting for about 45 minutes each. A semi-structured interview guide, containing questions about the students' perceptions on the use of Ni-Ti rotary instrumentation, was developed and used to conduct the interviews. Interviews were conducted right after each student had finished instrumentation of the four simulated canals (quantitative phase). The importance of the true expression of perceptions, without fear or embarrassment, was emphasized to the students. All interviews were audio-recorded and transcribed verbatim for analysis. Transcription was done within a 10-day period aiming to recall the atmosphere of the interview and avoid interpretation bias.
2.4 Data analysis
Students' performance on both techniques was assessed based on apical transportation, time required to complete instrumentation and procedural errors. These features were assessed twice by each examiner, and intra and inter-examiner agreement data were analyzed using intraclass correlation coefficient. Apical transportation associated with each instrumentation technique (hand and Ni-Ti rotary) was compared using Mann-Whitney's test. Because of the normal distribution of data, the Student t test was used to compare working time required for instrumentation with each technique. The Student t test for paired samples was used to compare the working time between the first and second canal instrumented by the same operator. Finally, Fisher's exact test was used to assess statistical associations between procedural errors and hand vs. Ni-Ti rotary instrumentation. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 10.0 (LEAD Technologies, Inc., Chi-cago, IL, USA). Significance was set at p < 0.05.
Students' perceptions identified in the interviews were analyzed using thematic analysis as proposed by Bardin20. The analysis comprised the following steps: i) pre-analysis; ii) content encoding (codes); iii) classification of codes into categories; and iv) inference. In other words, first, repeated readings allowed the creation of pre-thematic groups; afterwards codes were isolated from the text. Code is defined as a sentence or word that specifically explained the coded fragment. Subsequently, the codes were organized into a more general level named categories. Categories are sentences using words that provide meaning for the event being narrated into a more general level. Secondly, codes and categories were quantified and clustered into the two previously created broader pre-thematic groups; these groups were refined and gave the emergence of two themes (namely, hand and Ni-Ti rotary instrumentation). Lastly, the interpretation phase included searching, in all data corpus, for convergences and divergences among codes and categories to extract the students' perceptions on instrumentation with both techniques.
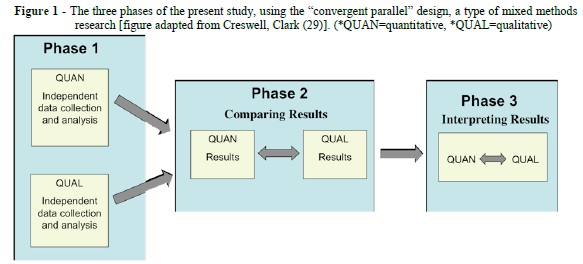
Interpretation of the study findings was based on the results of quantitative and qualitative strands, i.e., both statistical and textual analyses. Interactions between the two types of data are discussed. That is, our study followed a "convergent parallel" design: a type of mixed methods design where quantitative and qualitative data collection and analysis are independent, yet they are conducted concurrently at the same study phase19. The results were then compared and related to each other to provide a better understanding regarding the use of endodontic instruments by the students. Figure 1, adapted from Creswell, Clark19, shows the three phases of the study.
3 RESULTS
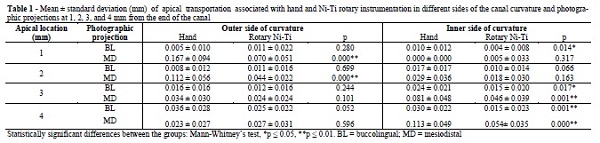
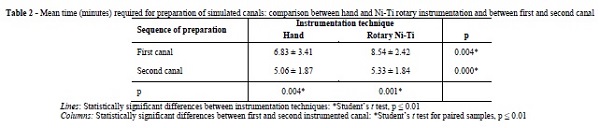
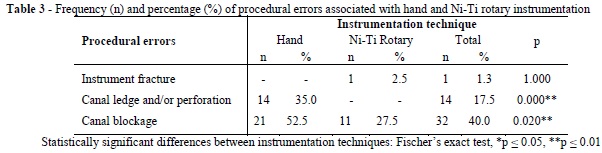
Analysis of apical transportation and procedural errors revealed adequate intra and inter-examiner agreement rates (intraclass correlation coefficient, p > 0.05). Overall, quantitative data showed a lower level of apical transportation and a longer working time associated with Ni-Ti rotary instrumentation when compared with hand instrumentation. Working time was shorter in the second canal instrumented with both techniques. Table 1, 2, and 3 show the results obtained for apical transportation, mean time required for preparation, and procedural errors associated with hand and Ni-Ti rotary instrumentation.
When assessing the data retrieved from the interviews, it was possible to distinguish two different perceptions regarding the workability of Ni-Ti rotary instruments, namely before and after using them. Before the experi-ment, the majority of the students (n=16, 80%) thought that Ni-Ti rotary instrumentation would be easier and faster. After the experience, however, there was an inversion in the students' opinions: 75% (n=15) reported that the hand technique had been easier.
Therefore, when focusing on the students' perceptions regarding the canal instrumentation experience, two thematic groups were extracted from the interviews: 1) perceptions regarding their experience soon after preparation of the first canal with the Ni-Ti rotary system; and 2) perceptions emerging later in the interviews, i.e., regarding the whole experience.
The former thematic group was expressed by two utterances: 1a) hand instru-mentation is easier (codes: training and cognition; categories: training improves tactile feeling/sensitivity and confidence, better feeling about what she/he is doing, more used to the technique, better domain of mental cognitive map due to daily practice); and 1b) there are technical difficulties of using Ni-Ti rotary instrumentation in relation to hand instrumentation (codes: training, cognition, and equipment; categories: lack of confidence, lack of practice, lack of cognition, lack of synesthesia, interposition of the motor handpiece during instrumentation, treadle-controlled torque re-versal).
These perceptions can be observed in the following utterances:
"Hand instrumentation is easier, because I have had the theory in my mind for a long time already..."
"I think you can only have that tactile feeling when you are in direct contact with the file, when you can feel it, touch it."
"When you use the rotary system, it moves by itself, all you need is to hold it, that's how I felt it."
"I did not have much... much tactile feeling... I did not have the same feeling that I had with the hand instrument."
"It slides through, goes by itself, gives you a strange tactile sensation, you know."
"Not being able to feel where the instrument was going… I had the impression that it was going to perforate the canal, go straight ahead, not making the curvature; at this point I was afraid of using ro-tary instrumentation, afraid that it wouldn't work out.
A cognitive and psychomotor conflict (uncertainty) on the part of the students was observed by the inquirer. This qualitative find-ing is addressed by one student in the utterance below:
"Even though I felt better during hand instrumentation, I think the Ni-Ti rotary system may lead to a better result... I can't tell... It seems that the rotary system moves on its own, perhaps it will result better... No, I can't tell yet."
The second thematic group was also expressed by the two following utterances: 2a) there are many advantages of using Ni-Ti rotary technique in relation to the hand technique (codes: training and technique; categories: confidence, stress reduction, fatigue reduction, speed, simplicity, flexibility, no need to prebend instruments); and 2b) we are aware of technical difficulties of Ni-Ti rotary instrumentation in relation to hand instrumentation (codes: theoretical knowledge, equipment, and simulated canals; categories: ignorance of instrument sequence, lack of equipment domain, difficulty determining the amount of pressure applied to handpiece, high degree of canal curvature, friction on the acrylic resin of simulated canals).
Even though the students thought that the Ni-Ti rotary technique was simpler, they were aware of the challenge associated with the use of a new technique. Interestingly, an increase in confidence was identified soon after Ni-Ti rotary instrumentation of the second canal. These perceptions were manifested as follows:
"The equipment does it all for you, you know, you don't have to do the quarterturn movement, for example, the pressure… it seems that the rotary system gives you more freedom, you know, you just have to let it do its job."
"In the beginning I felt a lot of difficulty with the Ni-Ti rotary system. But after I got the hang of it, my tactile sensitivity was so much improved! ... and you do not have to be changing instruments all the time!"
"I believe that, after training, Ni-Ti rotary instrumentation will result better than hand instrumentation."
"With a little training, the benefits of rotary instrumentation will exceed those of hand instrumentation, based on my first experience."
"... but the second canal instrumented using the rotary system... I think it looks good!"
"The second simulated canal that I instrumented with the rotary system was a little easier. I believe that practice progressively makes Ni-Ti rotary instrumen-tation easier in comparison with hand ins trumentation."
"Now, in the second canal, the rotary system became easier. Maybe if I had the chance to instrument a third canal, it would be faster... Using it has made me feel more confident."
"But if it were possible to take two people with the same expertise in both the hand and the rotary techniques, I think the rotary system would result better." "It seems that with practice it will become simpler, easier, and faster!"
Other perceptions identified in the interviews included a wish to have learned and used Ni-Ti rotary instrumentation since the beginning of their educational clinical activities, and good expectations regarding the final anatomical quality of the canal prepared and a shorter working time.
"We were remembering that when we were in the preclinic discipline (laboratory) we needed a whole semester to instrument four teeth, and today we did the same number of canals in two or three hours… "
"The cost of rotary instrumentation is compensated by the time saved while using the technique."
"The rotary technique should be introduced as part of the undergraduate program, not only in theory, but perhaps as an optional discipline." "It is not for 100% of the students, but for those with a different tactile sensitivity, for those who like endodontics, I think it would be really useful."
"All universities should offer this type of technology to their students. ... If I had not used rotary instrumentation here [in this study], I would graduate without learning it... And, if someone asked me about it, I would have no idea about what it was. It's an absurd, in fact."
4 DISCUSSION
Considering that every effort is welcome to improve the teaching-learning process in the academic setting, we claim that students' perceptions are a key element in the construction of that improvement. The present study was motivated by the view that there is room for pedagogical improvement in dental schools, and also by the current absence of a mixed methods research designed to explore interactions between findings resulting from canal instrumentation in vitro and students' insights.
Our main findings can be summarized as follows: 1) there was a lower amount of apical transportation at 1, 2, 3, and 4 mm from apex and fewer procedural errors (ledge/perforation/blockage) with Ni-Ti rotary instrumentation when compared to hand instrumentation; 2) working time was longer in canals instrumented with the Ni-Ti rotary technique; 3) working time was shorter during instrumentation of the second canal in each group; 4) hand instrumentation was referred to be easier and associated with better domain, practice, and confidence, due to the students being used to the technique; 5) Ni-Ti rotary instrumentation was associated with good initial expectations, but rose perceptions of doubts and difficulties concerning workability soon after its first use, because of lack of cognition and synesthesia, lack of equipment domain, and, especially, lack of practical training; 6) confidence increased after instrumentation of the second canal with the Ni-Ti rotary system, as expressed in the following expressions: stress reduction, speed, simplicity, practical training as a way to improve confidence; and 7) students felt an urgent need to include Ni-Ti rotary instrumentation in the undergraduate curriculum.
Results from the quantitative strand and perceptions identified in the qualitative strand will now be taken together and discussed based on the premise that the combined use of numerical data and open-ended approaches can provide a better understanding of research problems than the use of either approach alone19.
Interestingly, the perceptions identified soon after preparation of the first canal with Ni-Ti rotary instrumentation indicated that the students preferred the hand technique. This finding reveals a conflict between the existence of a well-established mental cognitive map in relation to the hand technique (which is traditionally performed by students as part of their academic program over a 2-year period), and an alteration of their kinesthetic sense while working with Ni-Ti rotary instruments (it was their first contact with this technique). The students' lack of theoretical and practical background in Ni-Ti rotary instrumentation led to uncertainty, which is understandable as they were dealing with a totally new situation.
Despite this confidence in hand instrumentation, hand-instrumented canals had worse quality than those shaped using Ni-Ti rotary instruments. The students' familiarity with the stainless steel hand technique did not avoid procedural errors, resulting in a higher amount of apical transportation at the four locations analyzed, 35% of ledge and/or perforations, and 52.5% of canal blockage, values significantly higher than those obtained with Ni-Ti rotary instrumentation. The better results found in canals instrumented with the rotary system are, at least in part, supported by the improved properties of Ni-Ti alloys, which result in anatomical advantages during root canal preparation1,2,12. From a different standpoint, it is important to note that the amounts of apical transportation found with both techniques are probably insignificant from a clinical point of view. Also, in our study, only one ProTaper Universal® F2 instrument fractured, similarly to the report by Tu et al.21 Therefore, the low frequency of instrument fracture, one of the main reasons why rotary systems are not indicated for novice students3,13, does not seem to be a reasonable ar-gument against the use of Ni-Ti rotary instruments at the preclinical or clinical undergraduate level in dental education.
Another finding of our analysis refers to the longer time required to complete rotary instrumentation when compared to the hand technique; these differences were statistically significant for both the first and the second canals (first - hand: 6.83 min, first - Ni-Ti rotary: 8.54 min; second - hand: 5.06 min, second - Ni-Ti rotary: 5.33 min). This result contrasts with other studies that have reported shorter preparation times with rotary instruments among novice dental students10,13,14. This difference can probably be explained by several methodological differences between the studies. First of all, those previous studies assessed different groups of operators and systems/techniques. Peru et al.10, for example, assessed three groups of students, each using a different system/technique (hand: 17.3 min, GT system: 5.29 min, ProTa-per: 6.1 min). Gluskin et al.14, in turn, assessed the same group of students using hand files (23.2 ± 9.0 min) in one mesial canal of mandibular molars and the GT™ rotary technique (5.9 ± 3.1 min) in the other. Our result of a longer time associated with Ni-Ti rotary instruments is also likely to reflect the feelings of uncertainty expressed in some categories (lack of confidence, lack of equipment domain, friction on the acrylic resin of simulated canal, etc.).
Finally, the longer time required to use Ni-Ti rotary instrumentation seems to reveal a cautious, prudent attitude towards the new tech-nique. Students mentioned many advantages of Ni-Ti rotary instruments, including simplicity, smooth handling, stress reduction, as well as potential improvements in canal anatomical features and canal cleaning. However, despite these advantages, they were conscious of the challenges and difficulties that were going to be faced, e.g., the need to have a deep theoretical understanding of the Ni-Ti rotary system chosen for use in clinical practice and extensive practical training. The feeling that arose was of responsibility. Such a behavior is in line with the opinion of Spångberg22 who reported that the apparent technical simplicity of Ni-Ti rotary instruments invites ignorance. That author stated that mechanical instrumentation alone will not improve endodontic outcomes; a thorough understanding of anatomy and pathology is also necessary.
A relevant result in our study was the reduced time required to instrument the second canal vs. the first, significantly lower with both techniques, hand and rotary. Some facts that could have influenced on this result are presumably the sense of adaptation to the environment (i.e., the presence of the researcher, the understanding about the procedures to be followed etc). In other words, the students felt more con-fortable, regardless the technique.
Specifically in relation to the rotary technique the great time reduction observed for Ni-Ti rotary instrumentation of the second canal (5.33 ± 1.84 min) in relation to the first one (8.54 ± 2.42 min) should be noted. It is general-ly accepted that repeated practice is necessary to develop clinical skills 23, and clinicians develop personal practical knowledge from their past and present experiences24. Based on this result and on the students' belief that practice progressively makes Ni-Ti rotary easier, we can hypothesize that, for Ni-Ti rotary instrumentation, perhaps a lower number of repetitions is necessary for students to improve performance and make the procedure less difficult when compared to the hand instrumentation technique.
Therefore, it is plausible to speculate that the learning curve for clinical skills with Ni-Ti rotary instrumentation may be shorter, i.e., that less practice may improve competence when compared to the hand technique. According to Chambers23, in dentistry, practice improves competence, but usually at a diminishing rate; eventually, additional practice ceases to add new skills. Although studying learning curves was not an objective of our study, data on learning curves for canal preparation can be found in the study of Mesgouez et al.25, who have shown that the time required for canal preparation tends to be inversely related to operator experience. In those authors' study, inexperienced operators showed progressively shorter working times as they instrumented more canals (each operator instrumented 25 canals); experienced operators, in turn, did not present working time reduction in the last 13 canals prepared.
Finally, taking into consideration the better anatomical results and the significant reduction in working time observed for the second canal instrumented with the rotary system, added to the students' perceptions regarding the need to learn Ni-Ti rotary instrumentation to improve knowledge, we could argue that academic institutions should consider to include Ni-Ti rotary instrumentation in the undergraduate dental curriculum as earlier as possible.
In sum, the quantitative data of our study, combined with the students' perceptions, allow us to draw the following overall conclusions: (i) students show a cautious, prudent attitude towards rotary instrumentation; (ii) confidence increases after rotary instrumentation of the second canal; (iii) students show good expectations in terms of optimizing root canal treatment with rotary instrumentation and they think it would be possible after some training; and (iv) Ni-Ti rotary instrumentation should be included in the undergraduate curriculum of dental schools.
REFERENCES
1. Peters OA, Paque F. Current developments in rotary root canal instrument technology and clinical use: a review. Quintessence Int. 2010;41:479-88. [ Links ]
2. Schäfer E, Bürklein S. Impact of nickel-titanium instrumentation of the root canal on clinical outcomes: a focused review. Odontology 2012;100:130-6.
3. Muñoz E, Forner L, Llena C. Influence of Operator's Experience on Root Canal Shaping Ability with a Rotary Nickel-Titanium Single-File Reciprocating Motion System. J Endod. 2014; 40:547-50.
4. Pécora JD, Capelli A. Shock of paradigms on the instrumentation of curved root canals. Braz Dent J. 2006;17: 3-5.
5. Martins RC, Seijo MO, Ferreira EF, Paiva SM, Ribeiro Sobrinho AP. Dental students' perceptions about the endodontic treatments performed using NiTi rotary instruments and hand stainless steel files. Braz Dent J. 2012;23:729-36.
6. De Quadros I, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ. Evaluation of endodontic treatments performed by students in a Brazilian Dental School. J Dent Educ. 2005;69:1161-70.
7. Pinchi V, Pradella F, Gasparetto L, Norelli GA. Trends in endodontic claims in Italy. Int Dent J. 2013; 63:43-8.
8. Paes da Silva Ramos Fernandes LM, Ordinola-Zapata R, Húngaro Duarte MA, Alvares Capelozza AL. Prevalence of apical periodontitis detected in cone beam CT images of a Brazilian subpopulation. Dentomaxillo-fac Rad. 2013;42:80179163.
9. Molander A, Caplan D, Bergenholtz G, Reit C. Improved quality of root fillings provided by general dental practitioners educated in nickel-titanium rotary instrumentation. Int Endod J. 2007;40:254-60.
10. Peru M, Peru C, Mannocci F, Sherriff M, Buchanan LS, Pitt Ford TR. Hand and nickel-titanium root canal instrumentation performed by dental students: a micro-computed tomographic study. Eur J Dent Educ. 2006;10:52-9.
11. Zanette F, Grazziotin-Soares R, Flores ME, Camargo Fontanella VR, Gavini G, Barletta FB. Apical Root Canal Trans portation and Remaining Dentin Thickness Associated with ProTaper Universal with and without PathFile. J Endod. 2014;40:688-93.
12. Grazziotin-Soares R, Barato Filho F, Vanni JR, Almeida S, Oliveira EP, Barletta FB, Limongi O. Flexibility of K3 and ProTaper universal instruments. Braz Dent J. 2011;22:218-22.
13. Sonntag D, Delschen S, Stachniss V. Root canal shaping with manual and rotary Ni-Ti files performed by students. Int Endod J. 2003;36:715–23.
14. Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84.
15. Henzi D, Davis E, Jasinevicius R, Hendricson W. In the students' own words: what are the strengths and weaknesses of the dental school curriculum? J Dent Educ. 2007;71:632-45.
16. Seijo MO, Ferreira EF, Ribeiro Sobrinho AP, Paiva SM, Martins RC. Learning experience in endodontics: Brazilian students' perceptions. J Dent Educ. 2013;77:648-55.
17. Elani HW, Bedos C, Allison PJ. Sources of stress in Canadian dental students: A prospective mixed methods study. J Dent Educ. 2013;77:1488-97.
18. Flick U. An introduction to qualitative research. 4th ed. London, U.K.: Sage Publica-tions Inc.: 2009.
19. Creswell JW, Clark VLP. Designing and conducting mixed methods research. 2nd ed. Thousand Oaks, California, USA: SAGE Publications Inc.: 2011.
20. Bardin L. L' analyse de content. 2nd ed. Paris: Puf Presses Universitaires de France Le Psychologue: 2013 [in French].
21. Tu MG, Chen SY, Huang HL, Tsai CC. Endodontic shaping performance using nickel-titanium hand and motor ProTaper systems by novice dental students. J Formos Med Assoc. 2008;107:381-8.
22. Spångberg L. The wonderful world of rotary root canal preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:479.
23. Chambers D. Learning curves: what do dental students learn from repeated practice of clinical procedures? J Dent Educ. 2012;76:291-302.
24. Ardenghi DM. Dentists' ethical practical knowledge: a critical issue for dental education. Eur J Dent Educ. 2009;13:69-72.
25. Mesgouez C, Rilliard F, Matossian L, Nassiri K, Mandel E. Influence of operator experience on canal preparation time when using the rotary Ni-Ti ProFile system in simulated curved canals. Int Endod J. 2003;36:161-5.
 Correspondencia para:
Correspondencia para:
Alexandre Azevedo Salles
Curso de Odontologia ULBRA
Av. Farroupilha, 8001 São José
92425-900 - Canoas/RS
E-mail: endosalles@gmail.com
