










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkIJD. International Journal of Dentistry
versão On-line ISSN 1806-146X
IJD, Int. j. dent. vol.9 no.2 Recife Abr./Jun. 2010
REVIEW ARTICLE REVISÃO DE LITERATURA
Auxiliary devices for management of special needs patients during in-office dental treatment or at-home oral care
Métodos alternativos para manejo do paciente com necessidades especiais durante o atendimento odontológico no consultório e a higiene bucal domiciliar
Iza Teixeira Alves PeixotoI; Cristiane Tomaz RochaII; Patrícia Motta FernandesI; Paulo Nelson-FilhoIII; Alexandra Mussolino de QueirozIV
IDDS, MSc, Department of Pediatric Clinics, Preventive and Community Dentistry, Dental School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil
IIDDS, MSc, PhD Student, Department of Pediatric Clinics, Preventive and Community Dentistry, Dental School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil
IIIDDS, MSc, PhD, Chairman, Department of Pediatric Clinics, Preventive and Community Dentistry, Dental School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil
IVDDS, MSc, PhD, Associate Professor, Department of Pediatric Clinics, Preventive and Community Dentistry, Dental School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil
ABSTRACT
Special needs patients often have features or limitations that limit their cooperation with in-office dental treatment or at-home oral care. This paper addresses the use of some auxiliary devices, such as physical restraint bands, Godoy's device, "Grandma's pants", "The Worm" and mouth gags and mouth props. These auxiliary devices are intended to aid the dental treatment in office and outpatient settings with increased comfort for both the patient and the professional and the oral homecare provided by parents/caregivers. Pediatric dentists should have knowledge of auxiliary devices that might be helpful during dental treatment of special needs patients and instruct the use these resources to parents/caregivers for maintaining a good-quality oral homecare of these patients.
Key-words: oral hygiene, dental care, disabled children
RESUMO
Os pacientes especiais geralmente apresentam características que, muitas vezes, podem torná-los incapazes de colaborar com a realização do atendimento odontológico e com a higiene bucal domiciliar. Esse trabalho se propõe a apresentar métodos alternativos, como faixas de contenção física, dispositivo de Godoy, a "calça da vovó" e a "minhoca", além de abridores de boca, que permitem viabilizar o tratamento odontológico desses pacientes em ambiente ambulatorial, promovendo conforto ao paciente e ao profissional. Estes dispositivos também permitem que os responsáveis consigam realizar uma higiene bucal satisfatória no domicílio.
Palavras-chave: hygiene bucal, assistência odontológica, crianças com deficiência
INTRODUCTION
Special needs patients are considered as those who have some kind of physical, mental and/or behavioral deficiency or limiting condition, and who therefore require either short-term or lifelong medical assistance and/or specialized health care1.
Dental care of these patents is usually complicated due to a combination of factors that include uncontrolled involuntary body movements, lack of motor ability, intellectual deficit and limited mouth opening. Low-quality oral hygiene (with a consequent great accumulation of dental biofilm) allied to a liquid/pasty diet, malocclusions, reduced salivary flow and chronic use of medication make these patients potential candidates to high caries risk and activity2-6.
Oral hearth promoters are not usually familiarized with the disease-specific medical features or with the implications and demands involved in treating special needs individuals3-6. Because of this, most dentists feel unprepared to deal with these patients and prefer to refer them to dental schools or public services7. Having access to professional dental care is often an additional challenge to these patients8-9.
Several devices have been developed to facilitate the dental treatment in office and outpatient settings. Theses resources are intended to accommodate the patient's body more properly in the dental chair and increase the comfort for both the patient and the dentist during clinical sessions3,10,12. Currently available examples of these resources include physical restrain bands, Godoy's device and foam or fabric rolls called "Grandma's Pants" and "The Worm"12. Mouth gags and mouth props are also a major aid to maintain an adequate mouth opening. All these adjunctive elements can also be of great help for the oral homecare provided by parents and/or caregivers12.
This paper describes the use of these auxiliary devices in special need patients for both in-office dental treatment and at-home oral care.
LITERATURE REVIEW
Restraint Bands
Physical restraint resources are indicated for patients with continuous, uncontrolled, involuntary movements, individuals with severe cerebral palsy, who are unable to understand the need of dental care and uncooperative, aggressive patients, who may accidentally cause injuries to themselves or to the dental staff during the clinical sessions.
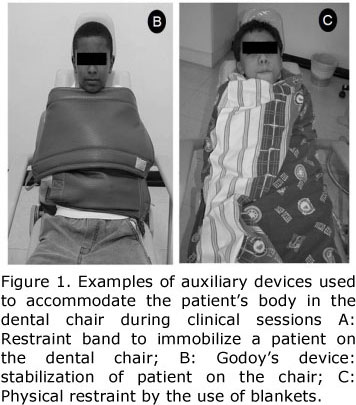
Restraint bands are a good option to stabilize the patient in the dental chair during treatment (Figure 1A). Whenever needed, the technique should be first explained to the patient and the parents/caregivers and written informed consent should be obtained. The bands should be made of a washable, smooth cloth and Velcro, and tied up firmly, though not tightly, in order to avoid hurting the patient during his/her attempts to move. Two standard sizes may be used: 145 cm x 35 cm for the legs and chest and 37cm x 13.5 cm for the arms.

Restraint bands have the advantage of being inexpensive, reusable, simple to attach, adaptable to any dental equipment, applicable to patients of all ages and easily borne or transported, which is a positive point in case of home dental appointments.
Godoy's Device
Godoy's device is a type of physical restraint developed to provide immobilization of patients with uncontrolled movements or aggressive behavior during treatment. According to the manufacturer, this device may be used by children over 4 years of age and adults13.
Godoy's device is composed by two shirts (upper and lower) that are used to secure the arms. The lower shirt stabilizes the patient in a comfortable position, allowing the arms to bend up to the chest, but retraining movements that could disturb the treatment. The upper shirt is used only if necessary (Figure 1B). The device has also a cervical collar that can be used in patients with uncontrolled involuntary head movements and can be regulated according to the patient's body size. A silicone thimble accompanies the product kit and is employed to keep the patient's mouth open during the procedures as well as to stabilize the patient's head against the chair. For individuals with spinal lesions, the manufacturer recommends the use of a rigid triangle, which will maintain the cervical spine straight and immobilized patient's body in a firmer and safer manner13.
Blanket
Physical restraint of children up to 10 years of age can be done with blankets (Figure 1C). After this age, the use of blankets is usually no longer effective because of the child's size and strength. For an adequate immobilization, the patient must be put with the arms crossed over the chest, in such a way that the legs can also be immobilized.
"Grandma's Pants"and "The Worm"
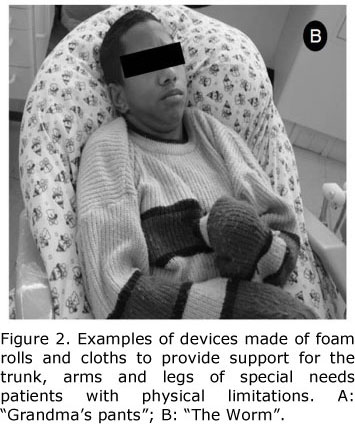
"Grandma's pants" (Figure 2A) and "The Worm" (Figure 2B) are easy-to-make and easy-to-use devices made of foam rolls and cloth, which have been developed by occupational therapists to provide support for the trunk, arms and legs of special needs patients with physical limitations. These devices provide comfort to the patient during treatment and a good working position to the dentist, which directly contribute to shorter and less fatiguing clinical sessions with consequently better treatment outcomes12. However, the "Grandma's pants" and "The Worm" are not intended to provide patient immobilization and so other resources should be used in association whenever physical restraint is required.

Mouth Opening Techniques
Patents with uncoordinated involuntary muscle movements and intellectual deficit are not able to keep the mouth open during in-office dental treatment or at-home oral care. To overcome this problem, dentists and parents/caregivers of special needs individuals can use devices specifically developed to help maintaining a good access to the oral cavity during cleaning or interventional procedures14,15. The most frequently used mouth openers are metallic mouth gags, which consist of reverse "C" shaped frames with an adjustable tongue depressor (Figure 3A), and rubber mouth props, which are usually found as trapezoidal (Figure 3B) or cork-shaped (Figure 3C and 3D) devices. These types of mouth openers are commercially available in the market and can be autoclaved.

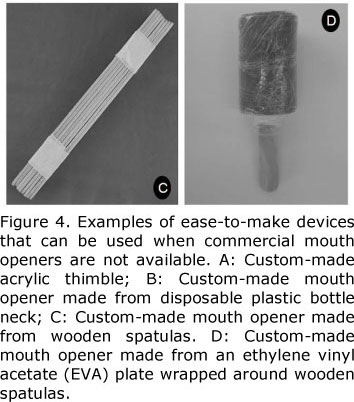
When commercial devices are not available, custom-made resources can be prepared by the dentist or caregiver. An acrylic thimble can be easily fabricated by casting the dentist's or caregiver's forefinger and duplicating the cast in acrylic resin (Figure 4A). Low-cost mouth openers can also be prepared with the neck of disposable plastic bottles (Figure 4B), wooden sticks (Figure 4C) and ethylene vinyl acetate (EVA) plates wrapped around two or three wooden spatulas (Figure 4D). According to a previous study15, PVC tubing can also be used for keeping the mouth open.

It has been demonstrated the action of cryotherapy on the masseter muscle produced a temporary reduction of spasticity and a significant increase of the inter-incisal distance after cold application to the masseter, facilitating the access to the occlusal and palatal surfaces of the maxillary molars16. This better access can be highly useful during dental treatment and oral hygiene.
DISCUSSION
Dental care of special needs patents is usually challenging because of their lack of motor ability, intellectual deficit and difficult to open the mouth or inability to maintain a sufficient interincisal space to permit adequate hygiene or treatment. Dental professionals dealing with these patents should have knowledge of commercial and custom-made auxiliary devices that might be helpful during treatment of these individuals, such as those presented herein. We agree with a previous study15 that parents/caregivers must be instructed on the use of these resources and work together with the dentist, maintaining a good-quality oral homecare. Families should be motivated to realize that positive atitudes towards oral health may reduce the likelihood and/or severity of caries disease. Health professionals should discuss the importance of maintaining a good oral health status for patients who usually present with a complex medical history and systemic fragility.
Coping with the problems of parenting and treating patients with debilitating and even life-threatening disorders is a challenging, lifelong experience. The physical disabilities, limitations and medical problems of these patients are so demanding that, sometimes, oral health care is excusably not regarded as a priority. However, adequate oral hygiene habits allied to an efficient in-office preventive support can avoid dental problems that would bring additional pain, discomfort and complications to these individuals.
CONCLUSION
In conclusion, the knowledge and use of auxiliary devices are of great help for during in-office dental treatment or at-home oral care of special needs patients.
REFERENCES
1. Original Council., 2004. Definition of persons with special health care needs. Reference Manual, 15. [ Links ]
2. Francis JR, Addy M, Hunter B. A comparison of three delivery methods of chlorhexidine in special needs children. II. Parent and house-parents preference. J Periodontol 1987; 58(7):456-9. [ Links ]
3. Miller C, Glassman P. Beyond brushing: training dental students to asses and create oral hearth plans for people with disabilities. J Dent Educ 1995; 59(2):368. [ Links ]
4. Levy-Polack MP, Sebelli P, Polack NL. Incidence of oral complications and application of a preventive protocol in children with acute leukemia. Spec Care Dentist 1998; 18(5):189-93. [ Links ]
5. Santos MTBR, Masieiro D, Simionato MRL. Risk factors for dental caries in children with cerebral palsy. Spec Care Dentist 2002; 22(3):103-7. [ Links ]
6. Glassman P, Miller C. Dental disease prevention and people with special needs. J Calif Dent Assoc 2003; 31(2):149-60. [ Links ]
7. McDermott RE, El Badrawy HE. A survey of parents' perception of the dental needs of their handicapped child. J Can Dent Assoc 1986; 52(5):425-57. [ Links ]
8. Thornton JB, Al-Zahid S, Campbell VA, Marchetti A, Bradley EL Jr. Oral hygiene levels and periodontal disease prevalence among residents with mental retardation at various residential settings. Spec Care Dentist 1989; 9(6):186-90. [ Links ]
9. Glassman P, Anderson M, Jacobsen P, Schonfeld S, Weintraub J, White A, Gall T, Hammersmark S, Isman R, Miller CE, Noel D, Silverstein S, Young D. Practical protocols for the prevention of dental disease in community settings for people with special needs: the protocols. Spec Care Dentist 2003; 23(5):160-4. [ Links ]
10. Dane JN. The Missouri Elks mobile dental program. Dental care for developmental disabled persons. J Public Hearth Dent 1990; 50(1):42-7. [ Links ]
11. Reichard A, Turnbull H, Turnbull A. Perspectives of dentists, families and case managers on dental care for individuals with developmental disabilities in Kansas. Ment Retard 2001; 39(4):268-85. [ Links ]
12. Reis F, Tannous GS, Macerou RTP, Belchior RS, Siebra MP. Alternativas de recursos posturais utilizados no manejo odontológico do paciente infantil paralisado cerebral. Revista Ibero-Americana de Odontopediatria e Odontologia do Bebê 2005; 8(41): 30. [ Links ]
13. Godoy, M.R. Sentidos. Visão. Available at: "http://sentidos.uol.com.br/canais/materia.asp?codpag=1702&codtipo=2&subcat=31&canal=opiniao." Accessed Mar 09, 2010. [ Links ]
14. Williams JN, Schuman NJ. The curved-bristle toothbrush: an aid for special needs population. J Dent Child 1988; 55(4):291-3. [ Links ]
15. Ferguson FS, Cinotti D. Home oral health practice: the foundation for desensitization and dental care for special needs. Dent Clin N Am 2009; 53:375-387. [ Links ]
16. Santos MTBR, Oliveira LM. Use of cryotherapy to enhance mouth opening in patients with cerebral palsy. Spec Care Dentist 2004; 24(2):232-34. [ Links ]
 Correspondence:
Correspondence:
Alexandra Mussolino de Queiroz
Faculdade de Odontologia de Ribeirão Preto, USP
Avenida do Café, S/N, CEP: 14040-904
Ribeirão Preto, SP, Brasil
Phone: +55-16-3602-4116
Fax: + 55-16-633-0999
e-mail: amqueiroz@forp.usp.br
Recebido em 11/03/2010
Aprovado em 26/04/2010
