










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista de Cirurgia e Traumatologia Buco-maxilo-facial
versão On-line ISSN 1808-5210
Rev. cir. traumatol. buco-maxilo-fac. vol.12 no.2 Camaragibe Abr./Jun. 2012
Symptomatology of fractures of the zygomatic complex. Analysis of a series of patients
Sintomatologia das fraturas do complexo zigomático. Análise de uma casuística de pacientes
Leonardo Toledo AguiarI; Rogério Bonfante MoraesII; João Gualberto de Cerqueira LuzIII
I Graduate student, Physiopathology Department, School of Medicine, University of São Paulo.
II Graduate student, Department of Oral and Maxillofacial Surgery, School of Dentistry, University of São Paulo.
III Department of Oral and Maxillofacial Surgery, School of Dentistry, University of São Paulo.
ABSTRACT
The purpose of this study was to evaluate signs and symptoms presented by a series of patients attended in a hospital clinic with a diagnosis of fracture of the zygomatic complex. Fifty consecutive patients with a diagnosis of unilateral fractures of the zygomatic complex were studied. Demographic data and symptomatology were obtained. Patients were asked about the presence of any symptoms. a subsequent physical examination included visual inspection and bimanual palpation of the face for the presence of specific signs. The data obtained were statistically analyzed and possible correlations among factors were evaluated. The most frequent signs were: step deformity of bone margin (100%), flattening of cheek (94%), periorbital ecchymosis (90%), facial asymmetry (86%), oedema (82%), epistaxis (68%), and subconjuntival ecchymosis (52%). The most frequent symptoms were: pain (82%), infraorbital anesthesia (70%), and pain on mouth opening (58%). There were few correlations between personal data or classification of the fractures and specific signs or symptoms. Statistical analyses showed a correlation only for subconjunctival ecchymosis with gender (p=0.032), and for diplopia with fracture of the orbital floor (p=0.031). It was concluded that there are signs and symptoms that can be considered typical of fractures of the zygomatic complex and that there are few correlations between the factors studied.
Keywords: zygomatic fractures, signs and symptoms, facial trauma, facial injuries.
RESUMO
a proposta deste estudo foi avaliar os sinais e sintomas apresentados por uma série de pacientes atendidos em uma clínica hospitalar, com diagnóstico de fratura do complexo zigomático. Cinquenta pacientes consecutivos com diagnóstico de fraturas unilaterais do complexo zigomático foram estudados. Dados demográficos e a sintomatologia foram obtidos. os pacientes foram questionados sobre a presença de algum sintoma. a seguir, o exame físico incluiu a inspeção visual e a palpação bimanual da face na pesquisa por sinais específicos. os dados obtidos foram analisados estatisticamente, e possíveis correlações entre fatores foram avaliadas. os sinais mais frequentes foram: degrau na margem óssea (100%), afundamento da região jugal (94%), equimose periorbitária (90%), assimetria facial (86%), edema (82%), epistaxe (68%) e equimose subconjuntival (52%). os sintomas mais frequentes foram: dor (82%), parestesia infraorbitária (70%) e dor na abertura da boca (58%). Houve poucas correlações entre dados pessoais ou classificação das fraturas e sinais ou sintomas específicos. as análises estatísticas mostraram correlação somente para equimose subconjuntival com gênero (p=0,032) e diplopia com fratura do assoalho de órbita (p=0,031). Foi concluído que existem sinais e sintomas que podem ser considerados característicos para fraturas do complexo zigomático, havendo poucas correlações entre os fatores estudados.
Descritores: Fraturas zigomáticas; Sinais e sintomas; Traumatismos faciais; Lesões faciais.
INTRODUCTION
Fractures of the zygomatic complex are frequent and often associated with facial lacerations or swelling from soft tissue injury1,2. Signs and symptoms of the fracture of the zygomatic complex are closely related to the surgical anatomy of the part1. It has been reported that more complex fractures, such as a tripod fracture with a distracted frontozygomatic suture, have more signs and symptoms associated with them3. However, no study has correlated signs and symptoms with demographic data or the classification of these fractures.
Some signs and symptoms, such as flattening of the malar prominence, ecchymosis of the lids and conjunctiva, diplopia, anesthesia in the distribution of the infraorbital nerve, and mandibular trismus, have been described as characteristic of zygomatic complex fractures4,5. On the other hand, some of these signs and symptoms are not specific to zygomatic complex fractures, and may occur with maxillary or nasal fractures. Although a significant improvement in imaging techniques has occurred over the last few years, the plan of treatment should be established based on the clinical and radiographic findings. Thus, it is important that the professional be able to recognize signs and symptoms characteristic of these fractures.
The purpose of this study was to evaluate signs and symptoms presented by a series of patients room with a diagnosis of fracture of the zygomatic complex attended in a hospital emergency unit.
MATERIAL AND METHODS
Fifty consecutive patients with a diagnosis of unilateral fractures of the zygomatic complex were studied. These were selected from facial trauma patients admitted to the Oral and Maxillofacial Surgery Clinic at Dr. Arthur R. de Saboya Hospital. The study was approved by the local committee on ethics in research.
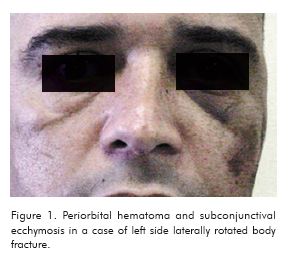
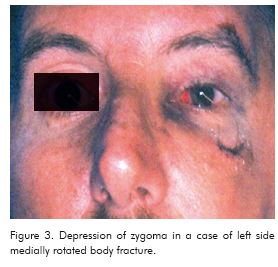
Demographic data and symptomatology were obtained. All the patients were attended by the authors. The occurrence of symptoms was recorded through direct conversation with the patient. Patients were asked about the presence of the following symptoms: pain, anesthesia or abnormal sensibility in the distribution of the infraorbital nerve, pain on mouth opening, diplopia or double vision, and visual impairment. Later, physical examination included an examination of the eyes and bimanual palpation of the face for the presence of the following signs: facial asymmetry, facial lacerations or abrasions, oedema, hematoma (Figure 1), epistaxis, subconjunctival ecchymosis (Figure 2), limitation of eye mobility, step deformity of bone margin, alteration of the eye globe position, and depression of the zygoma or zygomatic arch (Figure 3). The interincisal distance was measured during mouth opening, and cases were considered to have limitation when this value was < 40mm. A diagnosis of orbital fracture was confirmed by computed tomography when there was clinical evidence of the condition.
Radiographic evaluation included two or more of the following projections: Waters, postero-anterior, submentovertex axial, and computed tomography. No radiograph were taken for the purpose of this study. On the basis of the radiographic data, fractures were classified according to the system described by Knight and North6: I- No significant displacement; II- Zygomatic arch fractures; III- Unrotated body fractures; IV- Medially rotated body fractures; V- Laterally rotated body fractures; VI- Complex fractures. After clinical evaluation, all the patients except those with nondisplaced fractures underwent surgical reduction of their fractures, and the surgical findings were used to help in the classification.

In order to analyze the statistically obtained data in the comparison of two categories of a nonparametric variable, the Mann-Whitney test was used, while the Kruskal-Wallis test was employed in the comparison of three or more categories of a non-parametric variable,. When significance was observed, a cross-tabulation between factors was created and the Spearman correlation test performed. The level of significance was p≤0.050 in all the statistical analyses.
Radiographic evaluation included two or more of the following projections: Waters, postero-anterior, submentovertex axial, and computed tomography. No radiograph was taken with the purpose of this study. With the use of radiographic data, fractures were classified according to the system described by Knight and North6: I- No significant displacement; II- Zygomatic arch fractures; III- Unrotated body fractures; IV- Medially rotated body fractures; V- Laterally rotated body fractures; VI- Complex fractures. After clinical evaluation, all the patients but those with non displaced fractures underwent surgical reduction of fractures, and findings during surgery were used to help the classification.
In order to analyze statistically obtained data, in the comparison of two categories of a nonparametric variable, Mann-Whitney test was used, while in the comparison of three or more categories of a non-parametric variable, Kruskal-Wallis test was used. When there was a significance, a crossed tabulation between factors was made, and Spearman correlation test performed. The level of significance was p≤0.050 in all the statistical analyses.
RESULTS
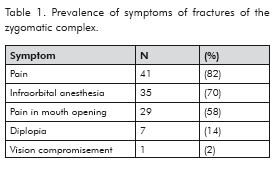
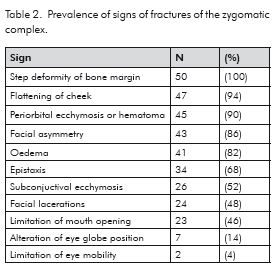
The majority of patients were males (86% of the cases), with the peak incidence occurring in the 21 to 30-year age group (34% of the cases). The distribution of the fractures according to the classification system adopted was as follows: I = 2 (4% ); II = 7 (14%); III = 4 (8%); IV = 24 (48%); V = 3 (6%); VI = 8 (16%); I + II = 1 (2%); II + IV = 1 (2%). Fracture of the orbital floor occurred in 4 cases (8%). The prevalence of symptoms is presented in Table 1 and that of signs in Table 2. Findings such as visual impairment, limitation of eye mobility, step deformity of bone margin, and flattening of cheek were not used for comparisons or correlation because they were either very rare or very frequent.
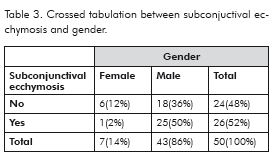
In the comparison between gender and signs and symptoms, with the application of the Mann-Whitney test, there was significance only with subconjunctival ecchymosis (p=0.033). Cross-tabulation between these factors is shown in Table 3. A correlation between gender and subconjunctival ecchymosis was confirmed (p=0.032).
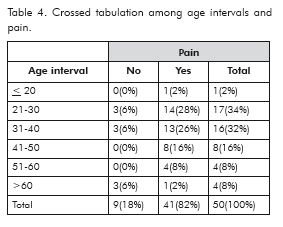
In the comparison between age intervals and signs and symptoms, with the application of the Kruskall-Wallis test, there was significance only with the occurrence of pain (p=0.043). Cross-tabulation between these factors is shown in Table 4. However, a correlation between age group and pain was not confirmed (p=0.508).
In the comparison between classes of fractures and signs and symptoms, using the Kruskal-Wallis test, there was no significance.
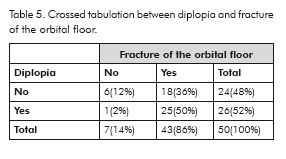
In the comparison between fracture of the orbital floor and signs and symptoms, using the Mann-Whitney test, there was significance only with diplopia (p=0.032). Cross-tabulation between these factors is shown in Table 5. A correlation between diplopia and orbital fracture was confirmed (p=0.031).
DISCUSSION
In this study, the signs and symptoms presented by patients with fractures of the zygomatic complex were evaluated. Also, possible correlations between symptomatology and the demographic data or classification of the fractures were analyzed. In order to avoid bias due to incomplete records, as well as differing criteria among consultants, all the patients were attended by the authors. The findings of this survey have corroborated previous reports regarding certain demographic data of zygomatic complex fractures. There was a higher frequency of males among the patients studied, confirming many studies3,5,8,9-11. The most affected age group was 21-30 years, thus corroborating previous studies3,10-12.
Fractures with displacement and medial rotation constituted the majority of cases in this study. This finding is at odds with previous studies6,11,13. A classification based on plain radiographs probably contains imprecisions, which are subject to personal interpretations, and depends on good radiographic techniques14. Imaging from computed tomography affords more details, and may have influenced the results2,8,15-17 , and this may also be the case with the surgical data.
Associated fractures of the orbital floor were infrequent, and this finding is similar to those of other studies. Such fractures should be confirmed with the use of computed tomography8,15-19. It is important to note that this involvement is associated with much of the morbidity related to zygomatic complex fractures2.
Pain, the most frequent symptom of these fractures, was found in our study with a high frequency, particularly in the fracture line areas, corresponding to the junctions of the zygomatic bone. However, its presence is seldom discussed in the literature20. Pain on mouth opening was found in more than half of the cases, being present mainly in the zygomatic arch and medially rotated body fractures. This symptom may be due to impingement of the coronoid process by the displaced zygomatic fragment, and can be slow to resolve postoperatively2.
Anesthesia in the distribution of the infraorbital nerve was often present, as has been reported by other authors3,5,20, except in fractures of the zygomatic arch. This symptom has been considered as characteristic of fractures of the zygomatic complex, although it is less frequent than pain – a nonspecific symptom in the trauma patient. Infraorbital anesthesia is usually temporary, except when there is compression or the nerve is torn5,10. In many cases it may persist, even after the reduction of zygomatic fractures20. Many patients do not complain of infraorbital abnormal sensibility, and it is important that this evaluation be brought to their attention, thus lessening the likelihood of postoperative concerns2.
Diplopia was found in some of the cases, corroborating previous studies that have reported an occurrence in 14.2 to 21% of cases5,6. Diplopia may be due to contusion of the extraocular muscles or swelling, as well as to entrapment of the muscles or orbital fat in the orbital fracture2,5. This symptom may resolve over time or require surgery2. Computed tomographic imaging is essential in identifying such orbital lesions2,7. Visual impairment, represented by a case with visual field loss, is a kind of severe ophtalmic disorder8. Comminuted zygomatic and blow-out fractures are most frequently associated with ocular injuries4,7. An ophtalmological evaluation of difficulties with vision or cases of extraocular motion is important to prevent the condition being interpreted as a postoperative complication2,7.
Step deformity of bone margin – the most frequent sign of these fractures - was present in all the patients, occurring in one or more fracture line areas. It has been considered the most frequent sign of zygomatic complex fracture1,5. Flattening of the cheek was observed in most of the patients, corroborating a previous study3. Loss of the normal prominence of the malar eminence is considered characteristic of zygomatic complex fractures5. However, this feature may be concealed by swelling1,2. This depression was better elicited by an axial view of the face. Facial asymmetry was verified in many patients. This finding can represent evidence of these fractures, while eye globe sinking may or may not be associated with them5,10.
Periorbital ecchymosis or hematoma occurred in a large number of cases. Although considered a typical sign of these fractures, it can sometimes make examination difficult2,5. Oedema was frequent, mainly in periorbital and cheek areas, and may also interfere with the clinical examination.
Homolateral epistaxis occurred in more than two thirds of the cases. This sign is more frequent in complex fractures, and of short duration3,5. Subconjunctival ecchymosis was present in more than half the cases. This finding may indicate an orbital wall fracture, but its absence does not exclude a fracture1. Facial lacerations occurred in almost half the cases. Although reported as frequent1, this sign is seldom mentioned in series of zygomatic fractures.
Limitation of mouth opening occurred in less than half the cases. This finding is associated with impingement of the coronoid process by the displaced fragment of the zygoma or zygomatic arch. Although trismus may be the chief complaint in zygomatic arch fracture5,10, in many cases this sign should be brought to the attention of the patient in order to minimize postoperative concerns2.
Alteration of eye globe position was verified in a few cases, particularly enophtalmus. This occurs due to downward displacement of the fractured zygoma or orbital wall fracture1,8,16. Although of great significance, the frequency of this sign has not been reported in zygomatic fracture series. Limitation of eye mobility was the least frequent sign and may be associated with a lesion of the orbital floor, with entrapment of inferior muscles or orbital fat, requiring surgery1,2.
When the statistical analyses were made, surprisingly few correlations were found between symptoms or signs and the factors studied. There was a correlation between diplopia and orbital floor fracture. This finding indicates that diplopia, though a possible cause of contusion of extraocular muscles or swelling, may signify an orbital floor fracture. An exploration with computed tomography is therefore mandatory in such a case8,15,17. The other correlation was between subconjunctival ecchymosis and gender. However, to the best of our knowledge no studies have demonstrated this finding. Despite the possible influence of other factors, further studies are necessary to shed light on this clinical event.
The analysis of the symptomatology of a series of patients showed that there are signs and symptoms that can be considered typical of fractures of the zygomatic complex. Step deformity of bone margin, flattening of cheek, periorbital ecchymosis, facial asymmetry, oedema, epistaxis, and subconjuntival ecchymosis were the most frequent signs. Pain, infraorbital anesthesia, and pain on mouth opening were the most frequent symptoms. However there were few correlations between the factors studied, such as age groups, gender or classification of the fractures, and specific signs or symptoms.
REFERENCES
1. Banks P, Brown A. Fractures of the facial skeleton. Wright, Oxford, 2002. [ Links ]
2. Hollier L H, Thornton J, Pazmino P, Stal S. The management of orbitozygomatic fractures. Plast Reconstr Surg. 2003; 111:2386-2392.
3. Ellis E, El-Attar A, Moss K F. An analysis of 2,067 cases of zygomatico-orbital fracture. J Oral Maxillofac Surg. 1985; 43:417-428.
4. Man K D, Bax W A. The influence of the mode of treatment of zygomatic bone fractures on the healing process of the infra-orbital nerve. Br J Oral Maxillofac Surg. 1988; 26:419-425.
5. Shroeder H G, Albanese S I. Fractures of the zygoma. Facial Plast Surg. 1990; 7:167-175.
6. Knight J S, North J F. The classification of malar fractures: an analysis of displacement as a guide to treatment. Brit J Plast Surg. 1961; 13:325-339.
7. Al-Qurainy A, Stassen L F A, Dutton G N, Moss K F, El-Attar A. The characteristcs of midfacial fractures and the association with ocular injury: a prospective study. Br J Oral Maxillofac Surg. 1991; 29:291-301.
8. Ellis E, Kittidumkerng W. Analyses of treatment for isolated zygomaticomaxilary complex fractures. J Oral Maxillofac Surg. 1996;13:386-400.
9. Khalil A F, Shaldi O A. Fractures of the facial bones in the eastern region of Líbia. Br J Oral Surg. 1981; 19:300-304.
10. Baldin C, Beltrane M, Dazzi P, Musola L. Contributo clinico-casistico su 370 casi di fratture C.O.M.Z," Minerva Stomatol. 1984; 33:729- 735.
11. Haug T A, Prather J, Indresano A T. An epidemiologic surgery of facial fractures and concomitant injuries. J Oral Maxillofac Surg. 1990;48:926- 932.
12. Turvey T A. Midfacial fractures: a retrospective of 593 cases. J Oral Surg. 1977; 35:887-891.
13. Pozatec Z W, Kaban L B, Guralnik W C. Fractures of the zygomatic complex: an evolution of surgical management with special emphasis on the eyebrow approach. J Oral Surg. 1973; 131:141.
14. Gerlock A J, Sinn D P. Anatomic, clinical, surgical, and radiographic correlation of the zygomatic complex fracture. Amer J Roentgenol. 1977; 128:235-238.
15. Manson P N, Grivas A, Rosenbaum A, Vannier M, Zinreich J, Iliff N. Studies on enophtalmos: II. The measurement of orbital injuries and their treatment by quantitative computed tomography. Plast Reconstr Surg. 1986; 77:203-214.
16. Lahbabi M, Lockhart R, Fleuridas G, Chikhani L, Bertrand J C, Guilbert F. Post-traumatic enophthalmos. Physiopathologic considerations and current therapeutics. Rev Stomatol Chir Maxillofac. 1999; 100:165-174.
17. Ellis E, Reddy L. Status of the internal orbit after reduction of zygomaticomaxillary complex fractures. J Oral Maxillofac Surg. 2004; 62:275-283.
18. Huet P, Gayet M, Aldegheri A, Mounios- Perchenet A S, Ferri J, Piot B, Mercier J. Les cinq incidences radiographiques conventionnelles nécessaires et suffisantes pour l'exploration de l'os zygomatique. Rev Stomatol Chir Maxillofac. 1996; 97:352-364.
19. Nkenke E, Maier T, Benz M, Wiltfang J, Holback L M, Kramer M, Hausler G, Neukam F W. Hertel exophthalmometry versus computed tomography and optical 3D imaging for the determination of the globe position in zygomatic fractures. Int J Oral Maxillofac Surg. 2004; 33:125-133.
20. Fogaça W C, Ferreira M C, Dellon A L. Infraorbital nerve injury associated with zygoma fractures: documentation with neurosensory testing. Plast Reconstr Surg. 2004; 113: 834-838.
 CORRESPONDING AUTHOR
CORRESPONDING AUTHOR
Prof. Dr. João Gualberto C. Luz
Rua Duarte de Azevedo 248, s.22.
02036-021 São Paulo-SP, Brazil.
e-mail: jgcluz@usp.br
