










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Odonto Ciência (Online)
versão On-line ISSN 1980-6523
Rev. odonto ciênc. (Online) vol.25 no.3 Porto Alegre Jul./Set. 2010
ORIGINAL ARTICLE
Dental caries in adolescents and its association with excess weight and sociodemographic factors in Londrina, Paraná, Brazil
Cárie dentária entre adolescentes e sua relação com o excesso de peso e fatores sociodemográficos em Londrina, PR, Brasil
Carlos Alberto TambeliniI; Denise Maimone RamosI; Regina Célia Poli-FredericoII; Cristina Simões de Carvalho TomasettiIII; Terezinha de Jesus Esteves BarataII; Sandra Mara MacielII,IV
ICurso de Mestrado em Dentística Preventiva e Restauradora, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brasil
IIDepartamento de Odontologia, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brasil
IIICurso de Nutrição, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brasil
IVDepartamento de Odontologia da Universidade Estadual de Maringá, Maringá, PR, Brasil
ABSTRACT
PURPOSE: To evaluate the prevalence of dental caries and investigate its association with sociodemographic factors and excess weight in adolescents.
METHODS: This is a cross-sectional study with a sample of 424 adolescents between 15 and 19 years of age. The prevalence of dental caries was assessed according to criteria defined by the WHO (1997); sociodemographic characteristics were obtained through interviews with the adolescents, and nutritional status was determined by the body mass index. Statistical analysis was based on the Chi-square, Mann-Whitney, and Kruskal-Wallis tests using a 5% significance level.
RESULTS: The prevalence of dental caries was 72.9% with an average DMFT (decayed, missing and filled teeth) index of 2.93. Excess weight was diagnosed in 22.4% of the adolescents. Factors that were associated with a greater severity included residence/school on the west side of the city (P<0.0001), 17 years of age (P=0.026), dark skin (P=0.005), lower education level (P<0.0001), higher maternal age (P=0.050), and lower family income (P=0.033). Despite an absence of statistical significance, the greatest dental caries severity was found among overweight adolescents and the lowest severity was found among obese adolescents.
CONCLUSION: Sociodemographic factors have an important influence on the prevalence of dental caries in the study population. Greater excess weight was not associated with dental caries.
Key words: Dental caries; obesity; overweight; demographic indicators; socioeconomic factors; adolescent
RESUMO
OBJETIVO: Avaliar a prevalência da cárie dentária e investigar sua associação com fatores sociodemográficos e o excesso de peso em adolescentes.
METODOLOGIA: Trata-se de estudo transversal com amostra composta por 424 adolescentes entre 15 e 19 anos de idade. A prevalência de cárie foi avaliada segundo critérios definidos pela OMS (1997); as características sociodemográficas, obtidas em entrevistas com os adolescentes; e, o estado nutricional, determinado pelo Índice de Massa Corpórea. A análise estatística compreendeu o uso dos testes Qui-quadrado, Mann Whitney e Kruskall Wallis, com nível de significância de 5%.
RESULTADOS: A prevalência de cárie foi de 72,9%, com o índice CPO-D médio de 2,93. O excesso de peso foi diagnosticado em 22,4% dos adolescentes. Os fatores associados à maior severidade de cárie foram: residir/estudar na região oeste da cidade (P<0,0001), ter 17 anos de idade (P=0,026) e ter cor de pele negra (P=0,005); a menor escolaridade (P<0,0001) e idade mais avançada da mãe (P=0,050); e, a menor renda familiar (P=0,033). Apesar da ausência de associação estatística, a maior severidade de cárie foi registrada entre adolescentes com sobrepeso e a menor, entre os obesos.
CONCLUSÕES: Os indicadores sociodemográficos exerceram importante influência na prevalência de cárie na população estudada, a qual não se associou às altas taxas de excesso de peso observadas.
Palavras-chave: Cárie dentária; obesidade; sobrepeso; indicadores demográficos; fatores socioeconômicos; adolescente
Introduction
Despite a significant decrease in the prevalence of dental caries, this disease is still the primary threat to oral health, in both developed and underdeveloped countries (1). This fact is especially attributed to the dichotomy between the oral health condition of children and adults (1). On the one hand, approximately 70% of countries have achieved the World Health Organization (WHO) goal for the year 2000 of a DMFT value < 3.0 at 12 years of age (1). On the other hand, dental caries affects approximately 100% of adults worldwide (1).I It can be inferred from the literature that there is a gap in oral health care during adolescence due to the paucity of epidemiological studies in this age group (2).
In Brazil, the most recent epidemiological study of oral health that had national coverage revealed that among individuals 15 to 19 years of age, about 90% presented with dental caries, with an average DMFT value of 6.2 (3). Additionally, that epidemiological study revealed that 14.4% of adolescents already presented loss of at least one tooth, and 13.5% of the adolescents had never had a dental appointment (3). This scenario is severe considering the fact that the DMFT index among young people can increase with age, leading to increased tooth loss (2).
According to Zero (4), among the multiple factors associated with the progression of dental caries, diet plays an unquestionable role with nutritional habits being a common risk factor for caries, as well as obesity and the diseases associated with it. The relationship between the ingestion of refined carbohydrates, especially sugars, and the prevalence of dental caries is well documented in the literature. However, studies addressing the relationship between obesity and dental caries in adolescents are scarce (5).
In addition to biological processes, socioeconomic conditions may influence the incidence of dental caries, disproportionately affecting disadvantaged groups in terms of both disease frequency and severity (6). The association between social deprivation and dental caries was highlighted in a study with adolescents in São Paulo, Brazil (7).
The present study aimed to evaluate the prevalence of dental caries and to investigate its association with sociodemographic factors and excess weight in adolescents of Londrina, in the state of Paraná, Brazil.
Methods
The study design was cross-sectional. The research was approved by the Research Ethics Committee of the Universidade Norte do Paraná (PP/0012/08).
The study population was composed of school-age adolescents of both genders enrolled in high schools of the Londrina (Paraná, Brazil) public school system. According to the school census reported by the Regional Education Nucleus in early 2008, the size of this population was 18,273. From this population, a minimum sample size of 391 was defined based on the formula proposed by Barbetta (8), with a 95% confidence interval and a 5% acceptable error margin.
To compensate for potential losses, we added 20% to that sample size (N=469). Inclusion and exclusion criteria were, respectively, age of 15 to 19 years and failure to present an informed consent form signed by the participant's parents or guardians.
Prior to the selection of participants, the municipality was divided into strata based on five geographical areas (North, South, East, West, and Central). In each of these areas, schools were classified as either large or small, based on the number of students enrolled. The next step consisted of randomly selecting one small and one large school in each region. A total of 10 schools were randomly selected. Next, two additional random selections were performed among 9th to 11th grade students in the target age group.
To evaluate the exposure and severity of dental caries, we used the decayed/missing/filled teeth (DFMT) index according to the criteria defined by the World Health Organization (WHO) (9). The clinical assessment was performed at the schools, under natural indirect light, with the examiner and the subject seated, using a flat oral mirror and a CPI probe after removing food remains with gauze. Standard biosafety measures were followed to protect the research staff and the study subjects. Data were collected in individualized records by adequately trained data entry personnel.
Staff training and calibration, as well as methodological adjustments, were performed in a pilot study that involved 30 adolescents who were not included in the final sample. The intra-examiner agreement was assessed by the Kappa statistic, and excellent agreement was found (Kappa=0.97).
The demographic (gender, age, skin color, residence area, and maternal age) and social characteristics (mother's education and family income) were obtained through personal interviews with the adolescents using a previously validated semi-structured form. Nutritional status was determined by the body mass index (BMI) using the BMI percentile curves defined by the Centers for Disease Control and Prevention (10).
Data were processed and analyzed by the Statistical Package for Social Science – SPSS, version 15.0. Univariate analysis was performed to identify potential associations between independent (sociodemographic characteristics and nutritional status) and dependent variables (history/severity of dental caries). For this analysis, the following tests were used: Chi-square, Mann-Whitney, and Kruskal-Wallis. The significance level was set at 5%.
Results
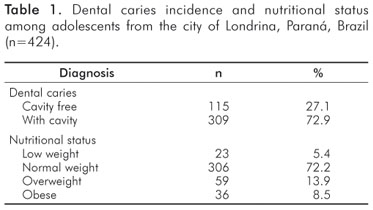
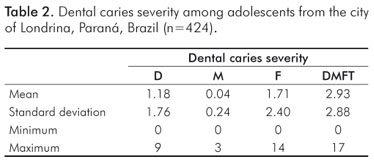
Of 469 consent forms sent to parents or guardians, 424 were signed (response rate = 90.4%). There was a predominance of females (66.7%) and participants 15 years of age (35.6%). The prevalence of caries was 72.9%, and excess weight (overweight and obese) was diagnosed in 22.4% of the evaluated adolescents (Table 1). Among those with a history of dental caries (Table 2), the average DMFT value was 2.93±2.88. Notably, the "decayed" (D) component accounted for 40% of the index.
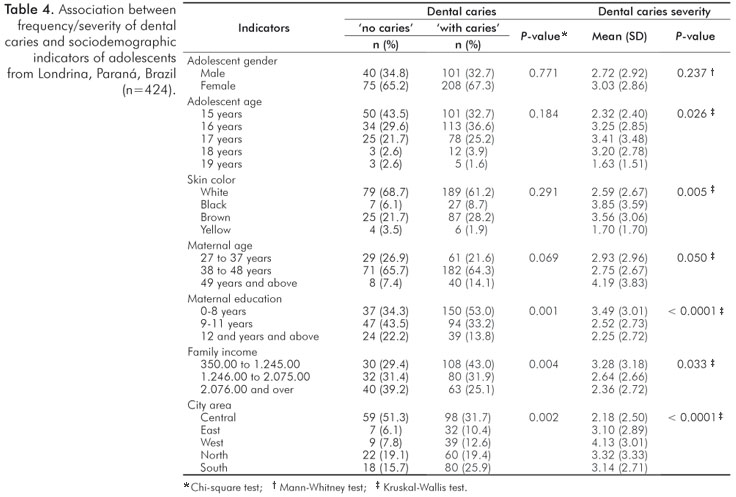
The prevalence of caries was not associated with the nutritional status of the population (Table 3). Similar percentages of adolescents who were free of dental caries and those with dental caries were observed in both normal and low weight groups. When focusing on the groups with excess weight (overweight and obese), the greatest caries level was found among participants who were overweight (15.5%). Similarly, the greatest severity of dental caries was found among overweight adolescents (DMFT = 3.46±3.01) and the lowest severity among obese adolescents (DMFT = 2.39±3.14). An analysis of the association between cavities and sociodemographic factors revealed correlations between the former and maternal education, family income and residence/ school area of the adolescents (Table 4). Adolescents with cavities had a higher rate of less educated mothers (P=0.001) and lower income families (P=0.004). Of note, of the adolescents who were cavity-free, 51.3% resided in the central area of the city. Furthermore, there was a tendency towards an association between maternal age and cavities in the adolescents with a higher cavity-free rate and with mothers in the 38 to 48 year age group (65.7%).
The severity of dental caries was associated with age, skin color, and residence/school area of the adolescents (Table 4). The mean DMFTvalue was higher in the West area (DMFT= 4.13±3.01), in the 17 year age group (DMFT=3.41±3.48), and among dark skin adolescents (DMFT =3.85±3.59). In addition, the severity of dental caries was associated with maternal age, education and family income. The most severe index was found among adolescents whose mothers: had little education (DMFT = 3.49±3.01), were older than 49 years of age (DMFT=4.19±3.83), and belonged to lower income families (DMFT=3.28±3.18).
Discussion
In the present study, the percentage of cavity-free adolescents was 27.1% and the DMFT was 2.93. These values denote better oral health conditions in the evaluated sample when compared to the results of local and regional studies in the same age group (7,11-13) as well as results of the most recent national study, which registered a 12.8% cavity-free rate and a 5.77 severity for the Southern macro-region of the country (3).
Among the factors that can explain the observed improved oral health condition, it is worth mentioning the fact that Londrina has had fluoridated water since 1972 and a Baby Clinic program since 1986, linked to the Universidade Estadual de Londrina. Remarkably, this program was a first experience with babies' oral health in Latin America and since then has been considered a referral center in the area. Therefore, it can be speculated that the improved oral health conditions observed in the study sample were, in part, a result of the participation of adolescents in this program.
Notably, the present study showed a tendency for the DMFT index values to increase with age, which is consistent with the literature (3,7,11,13,14). This finding must be carefully analyzed. Particularly during adolescence, selfcare, including oral health, is neglected (15). Therefore, oral health promotion should be focused on the family and household environment (16). Furthermore, oral health policies traditionally do not prioritize adolescence (17).
Considering these facts, it is essential for administrators and health professionals to formulate public policies that are not limited to clinical and preventive care, but rather promote equitable access to services and develop a collective management of health actions.
The finding that adolescents with dark skin presented the highest caries index is also consistent with the findings of previous work (19). The inequality among ethnic groups in regards to the risk of dental caries has been attributed to the fact that the socioeconomic conditions of black and mulatto individuals are than white individuals because an association with other biological factors has not been found (20).
In this study, the investigated socioeconomic factors demonstrated a direct association with both the incidence and severity of dental caries in adolescents. The greatest prevalence of the disease was found among those who belonged to low-income families and whose mothers had little education. These findings are consistent with those reported by another study that also noted that social inequity is associated with a higher prevalence of caries (21). These findings also reinforce the results of "SB-Brazil 2003," the most recent national oral health survey, which showed that the incidence of caries was more severe in populations with greater social deprivation (3).
According to Baldani et al. (21), in Brazil, there is a correlation between higher income and education and access to information and dental treatment. Likewise, Frias et al. (18) commented that the higher chance of caries in certain groups of adolescents demonstrates their higher vulnerability to the disease and reveals the reduced utilization of oral health care services for both educational/preventative and therapeutic actions.
A possible limitation of the present study was the sample selection, which involved only adolescents who were enrolled in the Brazilian public education system. However, it must be noted that this education system serves 78.7% of high school students in Londrina. Moreover, the city area stratification strategy was important because it allowed groups with greater dental needs to be identified. Thus, while establishing curative-preventative actions for oral health focused on adolescents, public health service administrators should prioritize those who live/study in the West area of the city.
Another interesting factor in the present study was maternal age. Adolescents whose mothers were older than 49 years of age demonstrated higher levels of caries in comparison to those whose mothers were younger, which may be a result of a paradigm change in dental practice. In recent years, health promotion actions have been more valued and more widely implemented.
Studies focusing on the relationship between dental caries and excess weight (overweight and obese) have presented controversial results. On the one hand, Moreira et al. (22) reported the absence of an association between dental caries and obesity in Brazilian adolescents between 12 and 15 years of age. On the other hand, Macek and Mitola (23) found that BMI was inversely associated with the severity of dental caries in permanent teeth in American children and adolescents between 2 and 17 years of age; i.e., those with excess weight had a lower DMFT value than those with normal weight. However, a significant association with caries severity and obesity in elementary school children and adolescents was reported in another study (24) that found a higher caries index among the obese.
Although a direct comparison among these studies cannot be performed due to the different age group investigated in the present study, our findings are consistent with the findings of Moreira et al. (22) because there was no statistically significant association between the caries severity and the nutritional status of adolescents. However, adolescents with lower rates of caries belonged to the low weight and obese groups. Additionally, the highest severity of dental caries was in the overweight group, while the lowest rate was in the obese group. According to Zardetto (11), being overweight may be considered a risk factor for higher caries severity. The analysis of adolescent nutritional status in the present study revealed an alarming proportion of overweight adolescents (22.4%), confirming the results of a similar Brazilian study (25). The high rates of dental caries and overweight adolescents in this study emphasize the need for interventions that focus on healthy eating habits, including the restriction of sugar consumption, and aim at preventing and controlling chronic diseases.
Conclusions
Socioeconomic indicators such as age, skin color, and area of residence/study, maternal age and education and family income were important determinants of caries prevalence in adolescents in the study population. Despite the lack of an association between caries prevalence and nutritional status, the greatest severity of caries was found in overweight adolescents and was lowest among obese adolescents.
References
1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiyae C. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization 2005;83:661-9. [ Links ]
2. Frias AC, Antunes JLF, Junqueira SR, Narvai PC. Determinantes individuais e contextuais da prevalência de cárie dentária não tratada no Brasil. Rev Panam Salud Publica/Pan Am J Public Health 2007;22: 279-85. [ Links ]
3. Ministério da Saúde (Brasil). Projeto SB Brasil: condições de saúde bucal da população brasileira 2002-2003: resultados principais. Brasília; 2004. [ Links ]
4. Zero DT. Sugars: the arch criminal? Caries Res 2004;38:277-85. [ Links ]
5. Willershausen B, Haas G, Krummenauer F, Hohenfellner K. Relationship between high weight and caries frequency in German elementary school children. Eur J Med Res 2004;9:400-4. [ Links ]
6. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cárie dentária no Brasil: declínio, iniqüidade e exclusão social. Rev Panam Salud Publica 2006;19:385-93. [ Links ]
7. Gushi LL, Soares MC, Forni TIB, Vieira V, Wada RS, Sousa MLR. Cárie dentária em adolescentes de 15 a 19 anos de idade no Estado de São Paulo, Brasil, 2002. Cad. Saúde Pública 2005;21:1383-91. [ Links ]
8. Barbeta PA. Fórmula para o cálculo do tamanho mínimo da amostra. Estatística aplicada às Ciências Sociais. 7.ed. Florianópolis: Ed. UFSC, 2007. p.315. [ Links ]
9. World Health Organization. Oral health surveys: basic methods. 4th ed. Geneva: World Health Organization; 1997. [ Links ]
10. Center for Disease Control and Prevention, National Center for Health Statistics CDC growth charts, United States NCHS. BMI Growth charts: 2000. [Acessed on 2008 July 27]. Available at http://www.cdc.gov/growthcharts. [ Links ]
11. Zardetto CGDC. Prevalência de cárie dentária em adolescentes residentes no município de São Paulo: indicadores de risco e gravidade. [tese]. São Paulo: Faculdade de Odontologia da Universidade de São Paulo; 2004. [ Links ]
12. Moimaz SAS, Saliba NA, Martins RJ, Murakawa AC. Influência da luz artificial na prevalência do índice CPOD em adolescentes institucionalizados. Rev odonto ciênc 2008;23:120-4. [ Links ]
13. Noro LRA, Roncalli AG, Mendes Junior FIR, Lima KC. Incidência de cárie dentária em adolescentes em município do Nordeste brasileiro, 2006. Cad. Saúde Pública 2009;25:783-90. [ Links ]
14. Moura C, Cavalcanti AL, Bezerra PKM. Prevalência de cárie dentária em escolares de 12 anos de idade, Campina Grande, Paraíba, Brasil: enfoque socioeconômico. Rev odonto ciênc 2008;23: 256-62. [ Links ]
15. Knishkowy B, Sgan-Cohen HD. Oral health practices among adolescents: a study from family practice clinics in Israel. Int J Adolesc Med 2005;17:99-104. [ Links ]
16. Polk DE, Weyant RJ, Manz MC. Socioeconomic factors in adolescents' oral health: are they mediated by oral hygiene behaviors or preventive interventions? Community Dent Oral Epidemiol 2010;38:1-9. [ Links ]
17. Nickel DA, Lima F G, Silva, BB. Modelos assistenciais em saúde bucal no Brasil. Cad. Saúde Pública 2008;24:241-6. [ Links ]
18. Frias AC, Antunes JLF, Junqueira SR, Narvai PC. Determinantes individuais e contextuais da prevalência de cárie dentária não tratada no Brasil. Rev Panam Salud Publica 2007;22:279-85. [ Links ]
19. Antunes JL, Peres MA, de Campos Mello TR, Waldman EA. Multilevel assessment of determinants of dental caries experience in Brazil. Community Dent Oral Epidemiol 2006;34:146-52. [ Links ]
20. Mendes LGA, Biazevic MGH, Michel-Crosato E, Mendes MOA. Dental caries and associated factors among brazilian adolescents: a longitudinal study. Braz J Oral Sci 2008;7:1614-9. [ Links ]
21. Baldani MH, Vasconcelos AGG, Antunes JLF. Associação do índice CPO-D com indicadores socioeconômicos e de provisão de serviços odontológicos no Estado do Paraná, Brasil. Cad Saúde Pública 2004;20:143-52. [ Links ]
22. Moreira PVL, Severo AMR, Rosenblatt A. Prevalence of dental caries in obese and normal weight Brazilian adolescents attending state and private schools. Community Dent Health 2006;23: 251-3. [ Links ]
23. Macek MD, Mitola DJ. Exploring the association between overweight and dental caries among US children. Pediatr Dent 2006;28: 375-80. [ Links ]
24. Willerhausen B, Blettner M, Kasaj A, Hohenfellner K. Association between body mass index and dental health in 1,290 children of elementary schools in a German city. Clin Oral Investig 2007; 11:195-200. [ Links ]
25. Toral N, Slater B, Silva MV. Consumo alimentar e excesso de peso de adolescentes de Piracicaba, São Paulo. Rev Nutr 2007;20: 449-59. [ Links ]
 Correspondence:
Correspondence:
Sandra Mara Maciel
Mestrado em Dentística Preventiva e Restauradora da UNOPAR
Rua Marselha, 183, Jardim Piza
Londrina, PR – Brasil
86041-100
E-mail: sanmaciel@sercomtel.com.br
Received: November 26, 2009
Accepted: April 9, 2010
Conflict of Interest Statement: The authors state that there are no financial and personal conflicts of interest that could have inappropriately influenced their work.

{kind=link}
{kind=link}