










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Odonto Ciência (Online)
versão On-line ISSN 1980-6523
Rev. odonto ciênc. (Online) vol.25 no.3 Porto Alegre Jul./Set. 2010
ORIGINAL ARTICLE
Patient's perception on mini-screws used for molar distalization
Percepção dos pacientes quanto ao uso de mini-implantes para distalização de molares
Micéli Guimarães BlayaI; Diego Segatto BlayaI; Magáli Beck GuimarãesI; Luciana M. HirakataI; Marcela MarquezanII
IPontifical Catholic University of Rio Grande do Sul, Porto Alegre, RS, Brazil
IIFederal University of Santa Maria, Santa Maria, RS, Brazil
ABSTRACT
PURPOSE: The objective of this study was to evaluate and compare the perceived pain intensity, side effects and discomfort related to the moment of placement, during mechanics and removal of a mini-screw for molar distalization in orthodontic treatment.
METHODS: The sample consisted of 30 adult patients with a mean age of 30 years old, with class II malocclusion subdivision right or left. A mini-screw was installed in each patient, in the maxillary arch to provide a molar distalization. The patients answered a questionnaire to assess their opinions on the treatment.
RESULTS: Ninety percent of the patients chose mini-screws over pre-molar extraction (orthodontic camouflage), or the use of an extra-oral appliance (Kloehn cervical traction) or another non-compliance treatment to class II. Aphthous ulcer was the side effect most frequent after placement of the mini-screw (30%). The greatest discomfort was felt during infiltration anesthesia (27%), though 23% reported no discomfort during placement. Eighty-three percent of the patients reported no pain during placement, which may be associated with the degree of satisfaction with the treatment (100%) and recommendation of the procedure to other patients (100%).
CONCLUSION: Mini-screws were well accepted by the patients and were efficient for molar distalization when utilized in association with orthodontic treatment for Class II malocclusion.
Key words: Orthodontics; Angle Class II malocclusion; orthodontic anchorage procedures
RESUMO
OBJETIVO: O objetivo desse estudo foi avaliar e comparar a intensidade de dor, os efeitos colaterais e o desconforto sentido pelo paciente relacionado à colocação do mini-implante, durante a mecânica e na remoção do mesmo, durante a distalização de molares no tratamento ortodôntico.
MÉTODOS: A amostra foi composta por 30 pacientes adultos com uma média de idade de 30 anos, com maloclusão Classe II subdivisão direita ou esquerda. Um mini-implante foi instalado em cada paciente, no arco superior para conseguir a distalização de molar. Os pacientes receberam um questionário a respeito de sua opinião sobre o tratamento.
RESULTADOS: Noventa por cento dos pacientes escolheram colocar os mini-implantes ao invés de realizar extração de molares (camuflagem ortodôntica), fazer o uso de um aparelho extraoral (Aparelho extraoral de Kloehn) ou fazer uso de qualquer outro tratamento alternativo para classe II. A úlcera aftosa foi o efeito colateral com a maior incidência após a inserção do mini-implante (30%). O maior desconforto foi sentido durante a infiltração anestésica (27%), embora 23% relataram não ter sentido desconforto durante o tratamento. Um total de 83% dos pacientes não relatou dor durante o tratamento, o que pode ser associado com o grau de satisfação com o tratamento (100%) e a recomendação desse procedimento a outros pacientes (100%).
CONCLUSÃO: Os mini-implantes foram bem aceitos pelos pacientes e foram eficientes para a distalização de molares quando utilizados em associação com o tratamento ortodôntico para correção da maloclusão de Classe II.
Palavras-chave: Ortodontia; maloclusão Class II de Angle; ancoragem ortodôntica
Introduction
The use of mini-screws to obtain absolute anchorage has recently become very popular in clinical orthodontic approaches (1). Mini-screws can be used either as direct anchorage units, when clinical forces are applied to the mini-screw, or as indirect anchorage units, when the forces are applied to dental units that are stabilized by the mini-screw (2).
During the past few years, the application of mini-screws include a wide array of cases, including: the correction of deep overbites (3-5), closure of extraction spaces (6,7) correction of canted occlusal plane (4), extrusion and uprighting of impacted molars (8,9), molar mesialization (10,11), alignment of dental midlines (4), extrusion of impacted canines (12,13), molar intrusion (14,15), intermaxillary anchorage for the correction of sagittal discrepancies (12,16,17), en-masse retraction of anterior teeth (17), maxillary molar distalization (9,16), and correction of vertical skeletal discrepancies that would otherwise require orthognathic surgical procedure (18,19).
For class II malocclusion assimetries, the mini-screw is an ideal dispositive to assist the orthodontic treatment because the professional thus does not depend on patient collaboration in the use of orthodontic rubber bands, or of an appliance of Kloehn cervical traction, for example, in order to achieve successful treatment (1). In addition, these implements make it possible to avoid pre-molar extractions in the case of Class II camouflage and laboratory procedures in the case of non-compliance alternatives treatment (e.g., distal jet).
These temporary accessories for orthodontic anchorage offer a number of advantages, including: easy placement and removal which does not require any particular surgical procedure, low cost, small size, variety of locations that can be inserted, patient collaboration is limited to maintaining good oral hygiene, and immediate orthodontic force/pressure reducing the total treatment time (2,6,20,21). The literature on mini-screw implants is diverse, however, the majority of studies is limited to the clinical application, success rate, properties, osseointegration and loading. Nonetheless, their use is still questioned in terms of apprehension, intolerance and psychological factors involved with this procedure (22).
This study aimed to verify the patient's perception on mini-screws for molar distalization during orthodontic treatment as well as the pain felt by patients during placement and the occurrence of unforeseen events during their utilization as orthodontic anchorage. In addition, this study assessed the patient's opinion on the treatment procedure.
Methodology
This study was approved by the Committee of Ethics and Research of the Pontifical Catholic University of Rio Grande do Sul (PUCRS/ Brazil), in accordance with the national and international standards for research in human beings.
Thirty consecutive patients who were undergoing ortho- dontic treatment between 6 to 8 months were included in the sample. All of them had class II malocclusion with left or right subdivision, that is, they had malocclusion Class I on one side and Class II on the counter-lateral side. These patients, therefore, needed correction for maxillary arch asymmetry, which was achieved through molar distalization with the use of mini-screw as orthodontic anchorage in the maxillary arch, interdentally between the roots of the first molar and second pre-molars.
Patients were undergoing orthodontic treatment in a private clinic. All patients were treated by the same orthodontist (M.B.) and mini-screws were placed by the same oral and maxillofacial surgeon (D.B.) with the same surgical technique. Before the treatment, all patients signed an informed consent form regarding the research protocol and the treatment plan, which consisted of implantation of one mini-screw in the maxillary arch. Those patients that chose not to accept the treatment with mini-screw and chose another treatment to correct the malocclusion were excluded from the study without any disruption to their treatment.
A surgical guide made of orthodontic wire was used in all patients to verify the receptor site (Fig. 1). Periapical radiographs were made before the mini-screw implantation in order to verify the mini-screw site without damage to the teeth or anatomic structures.
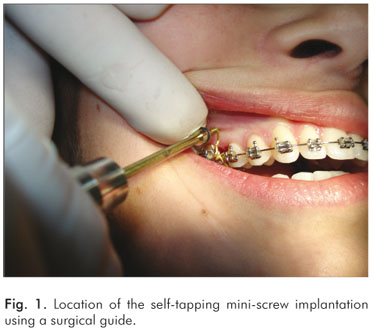
Mini-screws were installed under local anesthesia of the soft tissues at the implant receptor site. The entire procedure was carried out under sterile conditions. The mini-screw was inserted with a manual handpiece screwdriver (Sin Implant Systems, São Paulo,SP, Brazil) and considered immobile and stable at the moment of placement. Self-tapping mini-screws with total length of 10 mm, screw head of 3 mm and 1.2 mm of diameter, were obtained from Sin Implant Systems (Sin Implant Systems, São Paulo, SP, Brazil). After installation, a periapical radiograph was taken to evaluate the position of the mini-screw. After the surgical procedure, oral hygiene with an extra-soft toothbrush and the use of a 0.12% chlorhexidine mouth rinse were prescribed. No medications were prescribed.
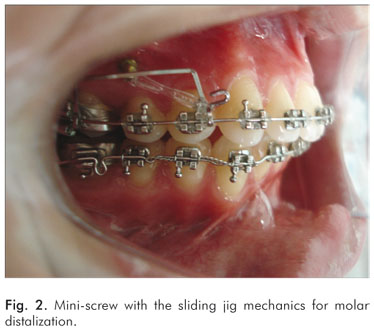
The mini-screws were used in the maxilla and were loaded two weeks after placement. The force applied to the mini-screw with the sliding jig mechanics was on average 300 g (Fig. 2). No medication or anesthesia was used for removal of the mini-screws. The mini-screw was grasped using a handpiece screwdriver and removed by anticlockwise rotation, with no lateral movement.
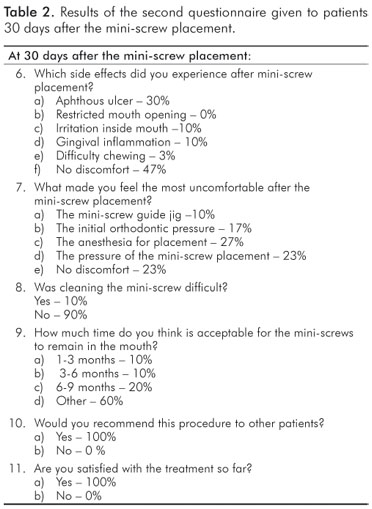
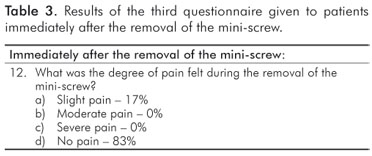
All patients responded to a questionnaire (Tables 1, 2 and 3) at three different time points: immediately after the mini-screw placement (T1), 30 days after placement (T2) and immediately after the mini-screw removal (T3). The questionnaire contained questions about patient acceptance including psychological aspects, degree of acceptance, pain, discomfort, tolerance and side effects.

Results
Thirty patients between 21 and 39 years of age (mean age = 30 years), 19 females and 11 males, were treated. A total of 30 mini-screws was installed. The mini-screws were removed after molar distalization (Table 1, 2 and 3) after 6 to 9 months (mean time = 7.5 months).
There were no failures, i.e., all mini-screws remained stable as an anchorage unit for the appliance during the orthodontic treatment.
Discussion
The questionnaire used in this study was useful to verify some aspects related to patient adaptation, side effects and degree of patient sensitivity at different times of the proposed treatment. The results can be used as a reference for future interventions, planning and questionnaires about experiences with these temporary accessories for orthodontic anchorage, especially in the treatment of Class II malocclusion.
As for the choice of orthodontic treatment for the correction of malocclusion (bilateral class II malocclusion), 90% of the patients selected the placement of 2 mini-screws rather than extraction of 2 pre-molars (3%), the use of an extra-oral appliance (3%) or another non-compliance treatment as distal jet, pendulum or jasper jumper (4%). This corroborates that the mini-screw is a practical appliance as patient cooperation is not necessary for its utilization, and in most cases it allows for treatment without extractions and results in successful treatment of the patient's type of malocclusion (22).
The patients were questioned about previous extractions and restorations in order to determine the number of patients that had undergone dental procedures for which they retained a memory of pain. Of the total sample, 83% had undergone some type of extraction, and 67% had had some type of dental restoration. These dental procedures are more common to happen in an dental office.
Pain affects quality of life and treatment cooperation (23), and the feeling of pain is a subjective parameter (24). When asked about pain felt during placement of the mini-screw, 77% of the patients were unable to compare it to pain from extraction or restoration, and 25% of those reported pain similar to that felt during anesthesia, 12.5% reported fear, 12.5% reported dental pressure on the first day after placement and 50% reported "nothing to compare". Although these alternatives were not included in the questionnaire, these patient reports are important as many expressed the same feeling about mini-screw placement. The remaining 17% reported pain similar to that felt during restoration, and 7% reported pain similar to that of extraction.
Despite the attempt to compare the pain felt to some previous dental procedure, 83% of the patients classified mini-screw placement as "without pain". This confirms the previous findings by Cornelis et al. (24), who reported that 82% of their patients said that the surgical experience was better than expected, with little or no pain. However, the perception of pain intensity is subjective and influenced by many other factors such as anxiety levels and motivational attitude (25).
Thirty days after the procedure, the patients were questioned about side effects and 30% reported aphthous ulcers, 20% gingival inflammation, 3% difficulty chewing and 47% reported no side effects. This is in accordance with the study by Tseng et al. (1), who reported that 40% of patients had no side effects (inflammation or ulcers) after placement of mini-screws.
The greatest discomfort related to the technique was the application of anesthesia during placement of the mini-screw (27%), followed by discomfort during mini-screw placement (pressure) (23%), the initial orthodontic force applied by the mini-screw (17%), and the mini-screw guide jig (10%). Nevertheless, 23% reported no discomfort whatsoever associated with the treatment alternative. However, all patients reported that while they attempted to choose the most suitable question alternative, they did not feel discomfort that would lead them to remove the mini-screw.
Forces of 300 g were reported for distalization maxillary molars with a lever-arm (4). In our study, the forces of 300 g (measured with a Richmond gauge) were used for molar distalization and did not cause much discomfort to the patient (17%). In general, the mini-screws were well tolerated by the patients (1,25). No patient requested to have the mini-screw removed and after 30 days, they did not mind having the mini-screw in place (60%). Twenty percent expressed the desire to have the mini-screw removed after 6-9 months, 10% after 3-6 months and 10% after 1-3 months. These patients expressed mildly negative comments such as "no one likes to have a foreign body in their mouth".
Almost all of the individuals had no difficulty in cleaning the mini-screw (90%), would recommend the procedure to a friend (100%) and were satisfied with the treatment (100%). No medication or anesthesia was used for the mini-screw removal. However, 83% of the patients felt no pain during removal, indicating no need for medication or anesthesia, as the application of anesthesia would cause a greater sensation of pain than the mini-screw removal itself.
Conclusions
Based on the present results, it can be concluded that:
-
90% of the patients prefer the utilization of mini-screws rather than premolar extraction (orthodontic camouflage), the use of an extra-oral appliance (Kloehn cervical traction) or another non-compliance treatment (distal jet, jasper jumper or pendulum);
-
For the side effects felt after mini-screw placement, aphthous ulcer was the most frequent followed by gingival inflammation. More than 40% of the patients reported no side effects.
-
The greatest discomfort felt during placement was that of infiltration anesthesia followed by the pressure during mini-screw placement.
-
The majority of the patients reported no pain during mini-screw placement or removal, which may be associated with the degree of satisfaction with the treatment and the willingness to recommend the procedure to a friend.
-
Mini-screws were well accepted by the patients.
References
1. Papadoulos MA, Tarawneh BDS. The use of mini-screw implants for temporary skeletal anchorage in orthodontics: A comprehensive review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:e6-e15. [ Links ]
2. Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod 1997:31;763-7. [ Links ]
3. Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Clin Orthod 1983;17:266-9. [ Links ]
4. Carano A, Velo S, Leone P, Siciliani G. Clinical applications of the mini-screw anchorage system. J Clin Orthod 2005;39:9-24. [ Links ]
5. Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini-implant for orthodontic anchorage in a deep overbite case. Angle Orthod 2005;75:444-52. [ Links ]
6. Park H, Bae S, Kyung H, Sung J. Micro-implant anchorage for treatment of skeletal Class I bialveolar protrusion. J Clin Orthod 2001;35:417-28. [ Links ]
7. Yun S, Lim W, Chun Y. Molar control using indirect mini-screw anchorage. J Clin Orthod 2005;39:661-4. [ Links ]
8. Park H, Kyung H, Sung J. A simple method of molar uprighting with micro-implant anchorage. J Clin Orthod 2002;36:592-6. [ Links ]
9. Bae S, Park H, Kyung H. Clinical application of micro-implant anchorage. J Clin Orthod 2002;36:298-302. [ Links ]
10. Giancotti A, Greco M, Mampieri G, Arcuri C. The use of titanium mini-screws for molar protraction in extraction sites. J Clin Orthod 2003;37:575-9. [ Links ]
11. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic microimplants of intraoral anchorage. J Clin Orthod 2003;37:321-8. [ Links ]
12. Papadoulos MA. Overview of the intra-maxillary non-compliance appliances with absolute anchorage. In: Papadoulos MA (ed.). Orthodontic treatment for the Class II non-compliant patient: current principles and techniques. Edinburgh: Elsevier, Mowby; 2006. p.341-4. [ Links ]
13. Park HS, Kwon OW, Sung JH. Micro-implant anchorage for forced eruption of impacted canines. J Clin Orthod 2004;38:297-302. [ Links ]
14. Bae SM, Kyung HM. Mandibular molar intrusion with mini-screw anchorage. J Clin Orthod 2006;40:107-8. [ Links ]
15. Yao CC, Lee JJ, Chen HY, Chang ZC, Chan Hf, Chen YJ. Maxillary molar intrusion with fixed appliances and mini-implant anchorage studied in three dimensions. Angle Orthod 2005; 75:754-60. [ Links ]
16. Chung K, Kim SH, Kook YC. Orthodontic microimplant for distalization of mandibular dentition in class III correction. Angle Orthod 2005;75:119-28. [ Links ]
17. Kyung SH, Choi JH Park YC. Mini-screw anchorage used to protract lower second molars into first molar extraction sites. J Clin Orthod 2003;37:575-9. [ Links ]
18. Kuroda S, Katayama A, Takano-Yamamoto T. Severe anterior open- bite case treated using titanium screw anchorage. Angle Orthod 2004;74:558-67. [ Links ]
19. Park HS, Kwon TG, Kwon OW. Treatment of open bite with microscrew implant anchorage. Am J Orthod Dentofacial Orthop 2004;126:627-36. [ Links ]
20. Kuroda S, Sugawara Y, Deguchi T, Kyung HM, Takano-Yamamoto T. Clinical use of mini-screw implants as orthodontic anchorage: Success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop 2007:131; 9-15. [ Links ]
21. Liou EJ, Pai BC, Lin JC. Do mini-screws remain stationary under orthodontic forces? Am J Orthod Dentofacial Orthop 2004:126;42-7. [ Links ]
22. Feldmann I, List T, Feldmann H, Bondemark L. Pain intensity and discomfort following surgical placement of orthodontic anchoring units and premolar extraction. Angle Orthodont 2007:77; 578-85. [ Links ]
23. Krukemeyer AM, Arruda AO, Inglehart MR. Pain and orthodontic treatment. Angle Orthod 2009;79:1175-81. [ Links ]
24. Cornelis MA, Scheffler NR, Nyssen-Behets C, De Clerk Hj, Tulloch JFC. Patient's and orthodontist's perceptions of miniplates used for temporary skeletal anchorage: A prospective study. Am J Orthod Dentofacial Orthop 2008;133:18-24. [ Links ]
25. Justens E, De Bruyn H. Clinical outcome of mini-screws used as orthodontic anchorage. Clin Impl Dent Relat Res 2008;10: 174-80. [ Links ]
 Correspondence:
Correspondence:
Micéli Guimarães Blaya
Av. Ipiranga, 6681 – Building 6
Porto Alegre, RS – Brazil
90619-900
E-mail: miceliblaya@gmail.com
Received: Jan 20, 2010
Accepted: April 4, 2010
Conflict of Interest Statement: The authors state that there are no financial and personal conflicts of interest that could have inappropriately influenced their work.
