










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRevista Odonto Ciência (Online)
versão On-line ISSN 1980-6523
Rev. odonto ciênc. (Online) vol.25 no.3 Porto Alegre Jul./Set. 2010
CASE REPORT
Desmoplastic ameloblastoma mimicking a periapical lesion
Ameloblastoma desmoplásico mimetizando lesão periapical
Esaú Pinheiro dos SantosI; Francisco Emanuel N. AraújoI; Daisy Pereira ValidoII; Sônia Oliveira LimaIII; Ricardo Luiz C. de Albuquerque-JúniorIII; Andrea Ferreira SoaresIV
ISchool of Dentistry, University Tiradentes, Aracaju, SE, Brazil
IIPost-graduate Program in Health and Environment, University Tiradentes, Aracaju, SE, Brazil
IIILaboratory of Morphology and Structural Pathology, Science and Technology Institute, Aracaju, SE, Brazil
IVDepartment of Morphology, Federal University of Sergipe, Aracaju, SE, Brazil
ABSTRACT
PURPOSE: Desmoplastic Ameloblastoma (DA) is a rare variant of ameloblastoma, with specific clinical, imaginological and histopathological features. The biologic profile of this tumor is not fully understood because of the limited number of reported cases. The purpose of this paper is to report a case of DA mimicking a periapical lesion.
CASE DESCRIPTION: This tumour appeared in the anterior region of the left upper jaw of a 24-year-old female, between left lateral incisor and canine. The lesion was painless and only a slight swelling of the hard palate mucosa was noted. Radiographically, a well-delimited peak-like radiolucent area promoting root divergence was observed. The lateral incisor failed in responding positively to the pulp tests. Provisional diagnosis of radicular cyst versus fissural cyst was established and surgical enucleation followed by curettage was carried out. Histological examination of the specimens revealed proliferation of nests and cords of compressed odontogenic epithelium immersed in a densely collagenized stroma, associated to a few irregular bone trabeculae.
CONCLUSION: These features were consistent with DA. The presence of a pulpally necrotic incisor and the atypical radiographic appearance obscured the disease. Despite the high rates of recurrence, no clinical or radiographic sign of reincidence of the tumor was detected one year later.
Key words: Desmoplastic ameloblastoma; odontogenic tumor; periapical lesion
RESUMO
OBJETIVO: Ameloblastoma desmoplásico (AD) é uma rara variante do ameloblastoma, com características clínicas, imaginológicas e histopatológicas específicas. O perfil biológico deste tumor não é totalmente compreendido, devido ao número limitado de casos notificados. O objetivo deste trabalho é relatar um caso de AD simulando uma lesão periapical.
DESCRIÇÃO DO CASO: Este tumor apareceu na região anterior da maxila esquerda numa paciente do gênero feminino de 24 anos de idade, entre o incisivo lateral esquerdo e o canino. A lesão era indolor e apresentava apenas um ligeiro inchaço da mucosa do palato duro. Radiograficamente, uma área radiolúcida bem delimitada que promovia a divergência radicular foi observada. O incisivo lateral respondeu negativamente aos testes pulpares. Diagnóstico provisório de cisto radicular versus cisto fissural foi estabelecido e enucleação cirúrgica seguida de curetagem foi realizada. O exame histológico das amostras revelou a proliferação dos ninhos e cordões de epitélio odontogênico comprimidos imersos em um estroma densamente colagenizado, associada a um trabeculado ósseo levemente irregular.
CONCLUSÃO: Estas características eram consistentes com AD. A necrose pulpar do incisivo e o aparecimento radiográfico atípico mascararam a real natureza da doença. Apesar das altas taxas de recorrência, nenhum sinal clínico ou radiográfico de recidiva do tumor foi detectado um ano mais tarde.
Palavras-chave: Ameloblastoma desmoplásico; tumor odontogênico; lesão periapical
Introduction
Some cases of benign and malignant lesions mimicking radiographically periapical lesions, such as keratocystic odontogenic tumors, cysts of the nasopalatine canal, periapical cemental dysplasia, benign tumors and locally aggressive or malignant neoplasias, have been described in the litera- ture (1). Therefore, histological study of the periapical lesions is mandatory in order to confirm the diagnosis and distinguish it from a non-inflammatory lesion (2).
Desmoplastic ameloblastoma (DA) was first described in 1984 by Eversole et al. (3) as a tumor presenting extensive stromal desmoplasia with small nests, cords and strands of tumoral odontogenic epithelium. It has been classified by WHO (World Health Organization) in 1992 as a variant of ameloblastoma with typical clinical, imaging and histological features (4). It occurs mainly in the anterior region of the jaws and appears radiographically as an unilocular or multilocular radiolucency, or as mixed radiolucent/radiopaque areas with either well-defined or poorly defined borders which resembles a fibroosseous lesion (5). Even though DA seems to present an aggressive behavior, similarly to the conventional ameloblastomas, only about one-hundred and fifty cases have been reported, so that the true biologic profile is yet to be fully understood (6).
The purpose of this paper is to report a unique case of desmoplastic ameloblastoma that was initially misdiagnosed as a periapical lesion.
Case Description
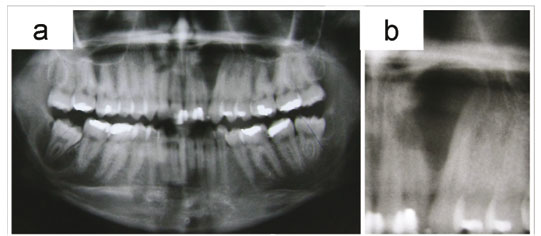
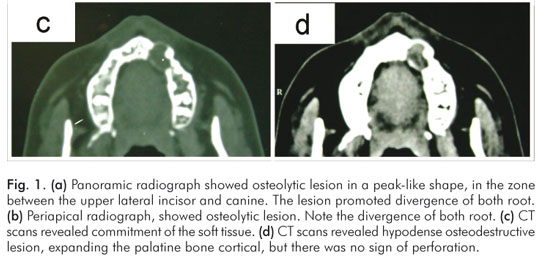
A 24-year-old female patient was referred to the Endodontic Service complaining of a "cystic lesion" in the anterior region of the maxilla, which had been present for about two months. The assessment of the previous medical history was no contributory. On the oral examination, all teeth on the left side of the maxilla were present, and only a very slight painless swelling of the right side of the hard palate was observed, although the bucal cortex felt to be intact, and normal in color and appearance. A panoramic radiograph showed an osteolytic lesion in a peak-like shape, with well-defined borders, in the zone between the upper lateral incisor and canine, promoting divergence of both roots. Maxillary sinus was not involved and there was no evidence of root resorption. A radiopaque image was seen in the mesial portion of the lateral incisor crown, consistent with resin restoration. CT scans revealed hypodense osteodestructive lesion, expanding the palatine bone cortical, but there was no sign of perforation (Fig. 1). Pulp vitality tests were performed, and only the lateral incisor showed to be unresponsive to electrical and thermal stimuli. Face the clinical and imaginological findings, provisional diagnosis of radicular cyst versus fissural cyst were established, and the excisional biopsy of the lesion was performed. The surgical specimen was sent to pathological examination.
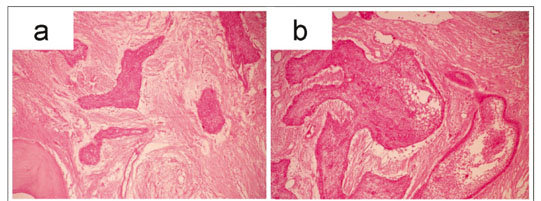
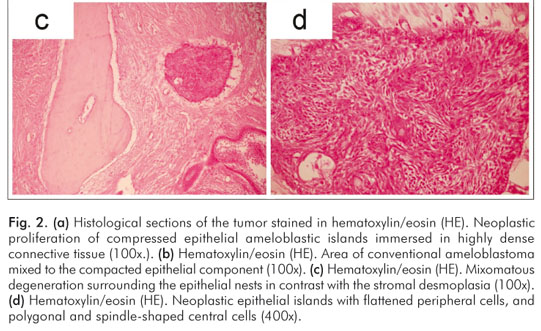
Microscopic examination of the histological slices revealed proliferation of compressed epithelial islands with flattened peripheral cells, and polygonal and spindle-shaped central cells compactly arranged. Columnar ameloblastic cells in a peripheral palisade pattern, and central loosely arranged cells resembling the stellate reticulum, could be observed in some areas. In addition, foci of cystic degeneration and squamous metaplasia were also verified within the epithelial nests. The tumor epithelium component was immersed in an extremely dense collagenous stroma, along with irregular trabecular bone formation in a few areas. In addition, mixomatous degeneration could be seen around some epithelial nests (Fig. 2). These findings were consistent with desmoplastic ameloblastoma. Despite the final diagnosis, the patient refused to submit for additional treatment, refuting the advices of the surgeon team, but agreed to keep under rigorous follow-up. One year later, however, no sign of recurrence has been noted yet.
Despite the final diagnosis, the patient refused to submit for additional treatment, refuting the advices of the surgeon team, but agreed to keep under rigorous follow-up. One year later, however, no sign of recurrence has been noted yet.
Discussion
DA is an unusual variant of ameloblastoma, which has a low occurrence rate and is characterized by marked stromal desmoplasia (7). Since it was first described in 1984 (3), a few more than one-hundred cases were reported in the lite- rature (5). Furthermore, there are also some rare reports of peripheral odontogenic lesions consistent with DAs (8,9).
Although DAs are similar to conventional solid amelo- blastomas regarding the age and gender distribution, studies have demonstrated that these tumors present a strong predilection for the anterior region of the jaws, just as presented in this study, occurring equally in the maxilla and mandible (6,7). In the current case, the age of the patient was 24 years-old, quite under the mean of about 42 years verified by Shashikanth et al. (5). Nevertheless, cases of DAs in younger patients have already been reported (6,10), so that further analysis of longer series are necessary in order to assure the real range of incidence of these lesions.
Huge predilection of occurrence of DAs in the anterior region of either maxilla or mandible has been reported (11), as observed in the current case. Maxillary lesions are expected to be more insidious than mandibular tumors owing to the proximity of vital structures. Also, the very thin cortical bone of the maxilla represents a weak barrier for the spread of tumors, so that maxillary ameloblastomas may spread earlier than mandibular neoplasms (12,13).
Histopathologically, the typical palisade pattern observed in the nests and cords of odontogenic epithelium in solid ameloblastomas may be absent in DAs. Hence, the adequate differential diagnosis from other odontogenic lesions, such as ameloblastic fibroma, odontogenic fibroma and squamous odontogenic tumour must be established (12). In this vein, the compressed appearance of the nests, the extremely dense collagenous stroma and the presence of variable mature lamellar bone may be helpful in distinguishing this tumor (5-7,10,13,14).
The main histological feature of DAs is definitely the intense stromal collagenization. Immunohistochemical studies have suggested that the desmoplasia might be a result of overexpression of transforming growth factor beta (TGF-β), one of the most potent local factors for modulating extracellular matrix formation (15). Furthermore, it has been proposed that this phenomenon has its origin from a new protein synthesis that comes from the extracellular matrix where such components play a fundamental role in supporting, adhering, proliferating, migrating and differing tumoral cells, interfering in the behavior and modulation of the tumoral cells (7). Moreover, it has also been proposed that this again synthesis of extracellular matrix proteins involved in the support, adhesion, proliferation, migration and differentiation of tumoral cells might be related to the phenomenon of desmoplasia (15).
The majority of reports of DAs describe a radiographic appearance of a mixed radiolucent/radiopaque lesion, with diffuse borders, similarly to a fibroosseous lesion or even malignant tumor (5-7,10,14). In this case, however, the radiolucent peak-like appearance was strongly suggestive of periapical lesion, particularly a radicular cyst, mainly when the imaginological features were associated with the pulp tests results. Most studies about periradicular lesions have focused on radicular cysts and granulomas, periapical lesions associated with pulpally necrosis and infection, owing to their high prevalence However, non-inflammatory lesions of different nature and biological behavior mimicking inflammatory periapical disorders have been reported (1). Therefore, pathoses located in the periradicular area, such as developmental odontogenic cysts, lymphomas, periapical cemento-osseous dysplasias, central giant cell lesions and ameloblastomas, among others, despite being rare, should always be considered in differential diagnosis. Variants of ameloblastoma, including DAs, are particular concerns due to their aggressive clinical behavior and high rates of recurrence. Furthermore, misdiagnosis might lead to inappropriate management of the lesion, like root canal treatment or tooth extraction, so that the delay in performing the adequate surgery could seriously complicate the prognosis of the tumor.
Since DAs tend to infiltrate the surround bone trabeculae, curettage is considered an inappropriate treatment for ameloblastomas, including DAs. Therefore, block excision is the most widely accepted form of treatment for such lesions of the maxilla, particularly because recurrence is almost inevitable and difficult to treat (12). Notwithstanding, owing to the clinical and imaginological features of the current case, it was treated by curettage, without previous incisional biopsy. As long as the recurrence rate of ameloblastomas treated by curettage ranges from 33.3% to 90%, additional surgical approach was required. Unexpectedly, the patient refused to submit to a new surgical procedure, although she had agreed in keeping under rigorous follow-up. Despite no sign of recurrence had been evidenced one year later yet, the lack of incisional biopsy may have jeopardized the prognosis of the tumor, so that a longer-term follow-up is clearly mandatory in order to assure the success of the treatment.
In the current case, a case of DA presenting clinically and imaginologically misdiagnosed as periapical lesion, leading to an inappropriate surgical approach, was presented. It is suggested that DA should be included in the differential diagnosis of periradicular lesions involving the anterior region of the jaws. Besides, it shows the relevance of performing incisional biopsies of bone lesions in order to provide subsidies for the suitable management of oral and maxillofacial pathoses.
References
1. García CC, Sempere FV, Diago MP, Bowen EM. The post-endodontic periapical lesion: histologic and etiopathogenic aspects. Med Oral Pathol Oral Cir Bucal 2007;12:585-90. [ Links ]
2. Ricucci D, Bergenholtz G. Histologic features of apical periodontitis in human biopsies. Endod Topics 2004;8:68-87. [ Links ]
3. Eversole LR, Leider AS, Hansen LS. Ameloblastomas with pronounced desmoplasia. J Oral Maxillofac Surg 1984;42:735-40. [ Links ]
4. Kramer IR, Pindborg JJ, Shear M. The WHO histological typing of odontogenic tumours. A commentary on the second edition. Cancer 1992;70:2988-94. [ Links ]
5. Shashikanth MC, Neetha MC, Ali IM, Shambulingappa P. Desmoplastic ameloblastoma in the maxilla: a case report and review of literature. Indian J Dent Res 2007;18:214-7. [ Links ]
6. Sivapathasundharam B, Einstein A, Syed RI. Desmoplastic ameloblastoma in Indians: report of five cases and review of literature. Indian J Dent Res 2007;18:218-21. [ Links ]
7. Desai H, Sood R, Shah R, Cawda J, Pandya H. Desmoplastic ameloblastoma: report of a unique case and review of literature. Indian J Dent Res 2006;17:45-9. [ Links ]
8. Curran AE, Byerly PD. Peripheral desmoplastic ameloblastoma: report of a rare case. J Oral Maxillofac Surg 2008;66:820-5. [ Links ]
9. Smullin SE, Faquin W, Susarla SM, Kaban LB. Peripheral desmoplastic ameloblastoma: report of a case and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:37-40. [ Links ]
10. Hirota M, Aoki S, Kawabe R, Fujita K. Desmoplastic ameloblastoma featuring basal cell ameloblastoma: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:160-4. [ Links ]
11. Kishino M, Murakami S, Fukuda Y, Ishida T. Pathology of the desmoplastic ameloblastoma. J Oral Pathol Med 2001;30: 35-40. [ Links ]
12. Pillai RS, Ongole R, Ahsan A, Radhakrishnan RA, Pai KM. Recurrent desmoplastic ameloblastoma of the maxilla: a case report. J Can Dent Assoc 2004;70:100-4. [ Links ]
13. Rastogi R, Jain H. Case report: desmoplastic ameloblastoma. Indian J Radiol Imaging 2008;18:53-5. [ Links ]
14. Mintz S, Velez I. Desmoplastic variant of ameloblastoma: report of two cases and review of the literature. J Am Dent Assoc 2002;133:1072-5. [ Links ]
15. Takata T, Miyauchi M, Ogawa I, Kudo Y, Takekoshi T, Zhao M et al. Immunoexpression of transforming growth factor beta in desmoplastic ameloblastoma. Virchows Arch 2000;436: 319-23. [ Links ]
 Correspondence:
Correspondence:
Esaú Pinheiro dos Santos
Instituto de Tecnologia e Pesquisa
Av. Murilo Dantas, 300 – Prédio do ITP
Bairro Farolândia
Aracaju, SE – Brasil 49032-490
Email: esau_pinheiro@hotmail.com
Received: December 28, 2009
Accepted: May 22, 2010
Conflict of Interest Statement: The authors state that there are no financial and personal conflicts of interest that could have inappropriately influenced their work.
