










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.58 no.3 Porto Alegre Jul./Set. 2010
ORIGINAL ORIGINAL
Cost-effectiveness ratio of public oral care in the perspective of service and society
Razão de custo-efetividade em saúde bucal na área pública sob a perspectiva do serviço e da sociedade
Christiane Alves Ferreira*; Carlos Alfredo Loureiro
Clínica Integrada de Odontologia - Ciodonto (Apoio Estação Ensino). Rua Santa Fé, 73, Sion, 30320-130, Belo Horizonte, MG, Brasil
ABSTRACT
OBJECTIVE: The objective of this study was to evaluate the cost-effectiveness ratios and the economic burden of oral care in the public health service from both the service and the society's perspective.
METHOD: Longitudinal data were collected from 7.825 patients treated by 13 dentists and two hygienists during one year. The completed treatment was considered the outcome. All costs were included, such as overhead, capital and operational costs. Two cost components were taken into account: cost opportunity and depreciation. Furthermore, the refresh rate of the initial capital was calculated and a sensitivity analysis was done.
RESULTS: From the perspective of service, the best cost-effectiveness ratios were for emergencies in all specialties ($10.99 to $12.98), followed by prevention, operative dentistry, endodontics and prosthesis. From the perspective of society, the best cost-effectiveness ratios were for emergencies in all specialties ($1.43 to $2.31), followed by endodontics, prevention, prosthesis and operative dentistry.
CONCLUSION: Priority differs both from the perspective of service and of society. From the perspective of service, the costs for elective care, including prevention, were close to the costs seen in high-income countries. From the perspective of society, the cost-effectiveness ratios for prevention in a clinical setting were unfavorable to be recommended for low-income populations. The perspective of society is an essential approach for decision-makers who need to allocate their resources.
Indexing terms: cost-effectiveness evaluation; fees and charges; oral health.
RESUMO
OBJETIVO: Avaliar a razão de custo-efetividade e o peso econômico dos cuidados com saúde bucal na área pública, sob a perspectiva do serviço odontológico e da sociedade.
MÉTODOS: Foram coletados dados de 7.825 pacientes tratados por 13 dentistas e 2 higienistas, durante o ano de 2004, em Sabará, Minas Gerais. O tratamento completado foi considerado como desfecho. Foram levantados custos de capital e custos operacionais. Dois componentes foram considerados: custo-oportunidade e depreciação. Além disso, foi calculada uma taxa de atualização do capital inicial e realizada uma análise de sensibilidade.
RESULTADOS: Sob a perspectiva do servi ço odontológico a melhor razão de custo- efetividade foi a consulta de emergência em todas as especialidades ($10,99 para $12,98), seguida por prevenção, dentística, endodontia e prótese. Sob o ponto de vista da sociedade a melhor razão de custo-efetividade foi a consulta de emergência para todas as especialidades ($1,43 para $2,31), seguida de endodontia, prevenção, prótese e dentística.
CONCLUSÃO: A prioridade difere dependendo da perspectiva da sociedade ou do serviço. Para o serviço, os custos dos cuidados eletivos, incluindo prevenção foram muito próximos dos custos de países de alta renda. Sob a perspectiva da sociedade, a razão de custo-efetividade para prevenção em ambiente clínico foi desfavorável para ser recomendado para uma população de baixa renda. A perspectiva da sociedade constitui-se numa abordagem essencial para tomadores de decisão que necessitam alocar seus recursos financeiros.
Termos de indexação: avaliação de custo-efetividade; honorários e preços; saúde bucal.
INTRODUCTION
The national healthcare systems of middle-income countries, where the needs are many and the resources are scarce, face a great and constant challenge between what can be offered to the population and the kind of services people would like to have. In Brazil, a middle-income country with a governmental budget of $96.48 per capita/year (2001), managing the resources carefully is necessary to meet all the healthcare needs1.
Economic assessment of health care is a useful tool to determine how scarce resources can be used to best benefit the community. This concerns the opportunity cost. When resources are used in a program, the opportunity to use them elsewhere is lost2. This is a good reason to incentivize economic assessments in middle- and low-income countries. However, Iglesias et al.3 found that it is not a common practice in Latin America to use economic assessments to support government decision-making. A recent systematic literature review confirmed that good quality studies on economic assessments of oral healthcare in Brazil have not yet been published4.
In Brazil, oral health services are universal and free of charge for the population, and sponsored by the three levels of government: federal, state and municipal, each being autonomous. Approximately 30% (56,995 in 2002) of Brazilian dentists work part-time or full-time in the public sector, and the services are manned mostly by paid personnel who follow national guidelines and operational norms. In practice, due to income barriers, poor people use public services, and the middle and high classes use private services either because they can afford to pay or have health insurance5. Nevertheless, government spending with public oral health care for low-income individuals can be considerable because of the high demand.
In 2004, the federal government introduced guidelines to redirect the national oral healthcare policy, expanding primary care and providing significant resources to implement a comprehensive program in secondary care6. Federal expenditure with oral healthcare in Brazil, including investments, was approximately $20 millions in 2002, increasing to $58 millions in 20047.
The expansion of secondary health care raises a concern: when resources are scarce, prioritization of a vertical equity with expansion of specialties always implies in forgoing primary care, pointing to a greater horizontal equity. The Brazilian population has very little access to healthcare services. In 2003, 15, 9% or 27, 9 million people, or worse, 31% of the poorest people, had never been to a dentist5. Without knowing the costs and effectiveness of oral care, both for the services and community, one concern is whether there are resources to finance an essential and extensive package of oral healthcare services, plus additional secondary services.
The present article intends to verify the cost-effectiveness ratios of a basic package and specialized care in public dental clinics, in the perspective of the service and society, using an oral public clinic in a Brazilian municipality as example.
METHODS
The present study was approved on March 18, 2003, by the Research Ethics Committee of Centro de Pesquisa da São Leopoldo Mandic, protocol number 995. The chosen clinic is located in the municipality of Sabará, state of Minas Gerais, Brazil. The clientele consisted of low-income individuals with an annual per capita income of $1,781.24, who typically live in the outskirts of large metropolitan areas with a Human Development Index of 0.77 (year 2000), ranking 1.253 among the 5.521 Brazilian municipalities. The clinic offered preventive care (two hygienists), operative dentistry (11 dentists), specialized care (one endodontist, one prosthesist) and emergencies in all specialties. Payment of personnel consisted of a mixed system, where 60% of their income was fixed and 40% was commission, determined by productivity and client satisfaction. The number of people per public dentist was 2,348.
Data from 8,178 patients were longitudinally collected during one year. The instruments had been previously validated8 and mistakes or inconsistencies were corrected by a researcher (F, CA). The effective working period of the personnel was taken down daily, discounting the losses due to inefficiency, and the results were converted to time units of 20 minutes each, named SCTU (standardized clinical time unit). The amount of effective SCTU per year and per specialty was used as overhead cost driver.
The following data were collected: time spent and number of visits to each specialty to complete a treatment, and the results were changed into SCTU. Completed treatment status was defined as conclusion of all care services provided by each specialty. The results were consolidated by type of care (elective or emergency) and by specialty.
Service cost was divided into capital and operational. Cost of capital included: building, furniture, dental equipment (chair, dental unit, etc.), peripherals (amalgamator, etc.), infection control, instruments and support equipment, such as computers. Market prices given by three independent evaluators were collected for deterministic costs. When possible, the costs were taken from public auction invoices. Capital cost was depreciated according to the life of the product and a 5% discount rate was applied. Depreciation and discount were combined using a table factor that supplies the equivalent annual cost (E)9. The life of the products ranged from thirty years (factor 15.3725) for the building, ten years (factor 7.7217) for dental equipment and furniture, and five years (factor 4.3225) for peripherals, support and instruments.
Operational costs included: salaries, incentives, dental supplies, suppliers (prosthesis laboratory, equipment maintenance), water, telephone, stationary, folders, consulting services, sanitary surveillance reports, specialized articles, cleaning material, meals and overhead costs.
Costs for patients and families included: treatment duration and transportation. For treatment cost, the amount equivalent to the amount of resources that would be paid by an employer to a minimum wage worker was used ($82.86 per month, plus labor benefits) relative to one hour overtime, added to the regular working hours, which in Brazil is 44 hours a week. The cost of overtime has been adjusted for differences in the treatment period. For transportation costs, a convenience sampling, standardized interview of 1453 patients was carried out to determine the means of transportation used (car, bus, walking or other) and the time spent on transportation to the clinic. The results indicated that 97% reached the healthcare facility by bus or walking. For the walking cost, the same method used for the treatment cost was used, since those two costs were coincidental; a single amount equal to $ 0.43/SCTU was used. For transportation costs, this amount was doubled and multiplied by the number of visits of each patient. For cost of the time spent with treatment, the amount of SCTU per patient was obtained and multiplied by that amount for each patient. All costs and consequences were adjusted with a discount rate of 5%9.
A simplified approach was adopted to share capital, operational and overhead costs (central administration, storage, public auction, transportation, etc). Initially, direct costs related to each specialty and activity were identified. The costs that were not directly attributable were allocated using the amount of SCTU spent per activity as a cost driver.
The economic analysis method was the cost-effectiveness ratio (CER) that requires ratio calculations for each intervention; these ratios are ordered from the best to the worst CER. This method differs from the incremental cost-effectiveness ratio method (ICER) in which the interventions are mutually excluding. In CER, independent interventions, all of them necessary, are compared, and the costs and effects of an intervention are not affected by the introduction or superposition of another one. The results are useful to support the policy decision among the types of health care services or programs that should be prioritized, according to the available budget10. This method allows the evaluation of oral care alternatives that maximize the use of limited resources.
Stochastic data from which the mean, standard deviation and confidence interval were obtained were used to reduce uncertainty. To test all the assumed decisions about costs for deterministic data, which are punctual estimates with a higher degree of uncertainty, a sensitivity analysis was done. The worst and the best scenario were compared varying the data in plus or minus 20 percent, with all the calculations being redone to verify whether they changed the direction or the magnitude of the obtained endpoints, compared with the original ones. To make the comparisons easier, all costs, as well as those from other reviewed studies, were converted into US dollars using the exchange rate of the date the study.
RESULTS
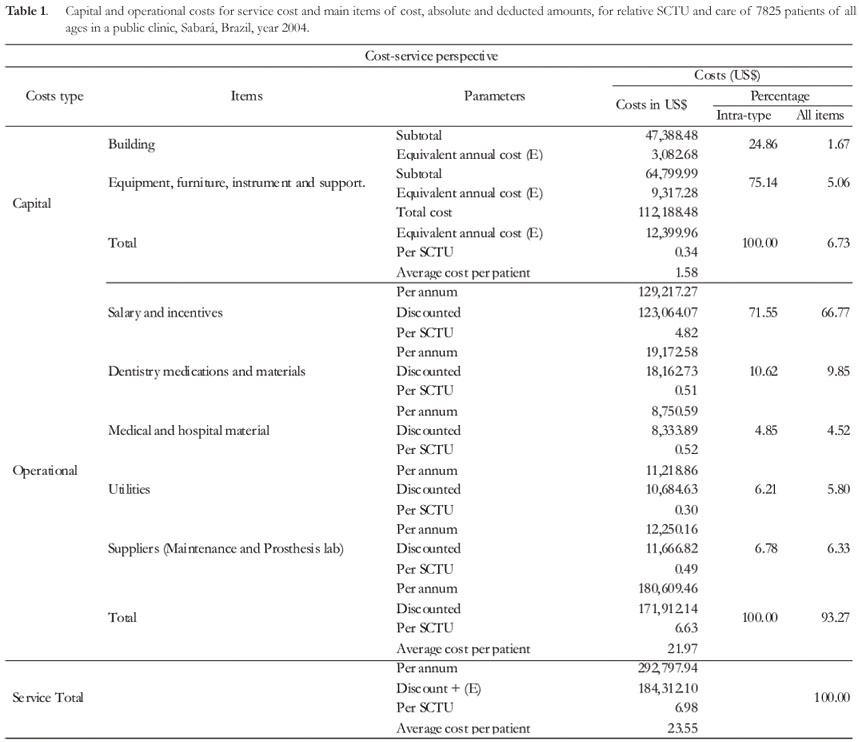
From the baseline sample of 8,178 patients, 353 (4.32%) were excluded for several reasons, such as: treatment dropout, incomplete data etc. The final sample consisted of 7825 patients, 4,847 (61.94%) in elective care and 2,978 (38.06%) in emergency care. Table 1 presents service costs.
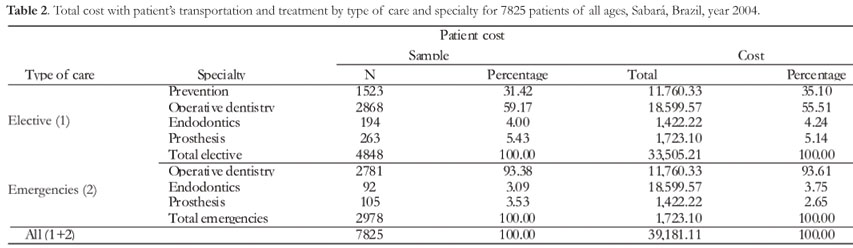
The capital cost is significant in the first year, but after being adjusted as a yearly equivalent cost, the amounts were: average per patient equal to $1.58 and 6.73% of the total cost of the service. The average operational cost per patient was $21.97, which represented 93.30% of the total cost. The total average cost was $23.55 per patient. The main cost item was salary plus incentive (66.77%), followed by dental material (9.85%). Table 2 shows the total patient costs.
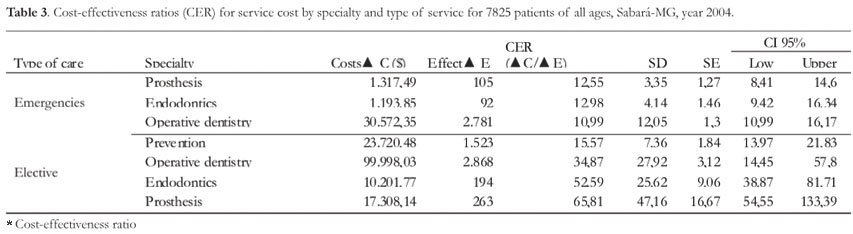
The total cost for patients was $39,181.11. Both in elective care and emergencies, the higher total cost was in operative dentistry. Table 3 presents the cost-effectiveness ratio for elective and emergency care from the perspective of service.
Table 3 presents the CERs from the perspective of service for 7825 patients. The most used specialty (elective + emergency) was general practice (72.19%), followed by prevention (19.46%), prosthesis (4.70%) and endodontics (3.65%). Emergency care presented the best CER compared with the CER for elective care, with no significant difference. The best CER was prosthesis emergencies, with no significant difference for other emergency care. The CER for all the elective services except for prevention was $38.35 (not shown). The best cost-effectiveness ratio (CER) was in prevention, followed by operative, endodontics and prosthesis. The confidence intervals show a significant difference in elective care CER only between prevention and the other specialties.
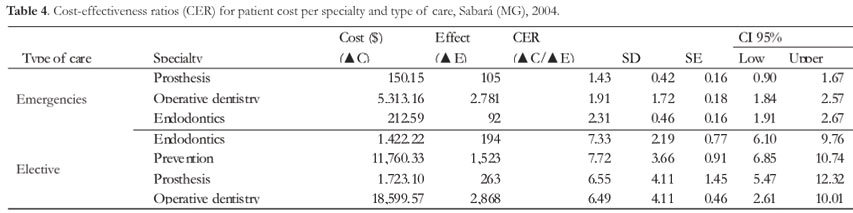
From the perspective of society, emergency care presented the best CER compared with elective care and there was a significant difference for these healthcare services. In emergencies, the best CER was for prosthesis, with significant difference only between this care service and the others in emergencies. For elective care, the best CER was for endodontics, followed by prevention, prosthesis and operative dentistry. The confidence intervals did not indicate significant differences among those types of care.
DISCUSSION
A question for economic studies to answer is: to what extent the results of a given scenario are valid for other scenarios? Costs and productive efficiency may vary considerably among health settings11. To increase the external validity of the present study, a pragmatic outlining was used with longitudinal routine data collected from a typical public dental care clinic in Brazil, located in the outskirts of a big metropolitan area that provided assistance for poor patients of any age by demand. These are the characteristics that admittedly contribute to the good external validity of the results for scenarios similar to the one assessed12.
Uncertainty was approached by doing a sensitivity analysis. The simulations for deterministic data resulted in small CER differences compared with the original ones. Productive efficiency simulations considerably impacted the costs, affecting more intensely higher fixed-cost specialties (prevention) than variable cost ones (prosthesis), but the differences have not changed the direction of the results, which increase the confidence in the validity of the results.
One limitation of the present study is that it used as an outcome measurement intermediate endpoints and not final endpoints, like quality adjusted life years or others, which evaluate the consequences of the interventions on the patient's health. However, this approach has been advocated when the intention is to assess the productive efficacy of the several types of independent interventions, and not the assessment of the usefulness of the healthcare interventions for consumers of health services13.
A somewhat unexpected result was the evidence, in a middle income country, of elective care costs very close to those reported for high income countries, mainly due to the assessed salary costs, main cost item, which were up to six times lower than those reported for high income countries14. In Australia15, cost assessment in the public sector found an average of $46.59 for general practitioners and $30.16 for emergencies.
In high-income countries, the high cost of preventive programs done in a clinical setting has been previously set16-17. The economic efficiency of those programs has been questioned in systematic literature reviews4,18.
Many factors may be suggested to explain that surprising finding. The most obvious are the methodological differences. The cost items considered here were very comprehensive and included all the capital costs and overhead costs, which may result in very different costs9. Other reasons may be related to the differences of settings relative to the delivery of oral care services, like the number of untreated cases and the coverage of the healthcare services. In Australia, the services for adults were much more limited.
From the perspective of service, a projection of the costs obtained, in case the oral care were extended in public clinics to only twenty percent of the Brazilian population, in one year, the present national budget for oral health would have to be more than doubled19. This shows the difficulties that most of the low-income countries have to finance oral care services for children. The results presented here indicate the need of economic rationality to allocate the scarce resources of middle-income countries.
The CER found in this study indicated that - from the perspective of service - emergency care should be a priority, followed by prevention, operative dentistry, endodontics and prosthesis. From society's perspective, the priorities should be: emergency, endodontics, prevention, prosthesis and operative dentistry. The results show differences when both perspectives are considered. For example, among the elective care and from the perspective of service, prevention presented the best CER, with a significant difference for other interventions. From the society's perspective, prevention was the second to last priority, with a less favorable CER and a significant difference, compared with emergency care intervention and with similar CER, and without significant difference for other elective care.
The present study assessed health cost and benefits for society as a result of oral health interventions. For public policies purposes, the comparability of the study is enhanced when it is taken as a norm from the society's perspective20. The results suggest that, since preventive care services and other healthcare services have similar costs, when poor patients from middle-income countries, with numerous accumulated and untreated needs, have to choose to which type of care they should allocate their scarce resources to achieve greater well-being, many may not choose preventive care services, compared with treatment. The patient costs for access to preventive care represent from eight to twelve percent of the monthly income of 15% of the Brazilian families who live on a minimum wage5. However, although low, that percentage may be "catastrophic" because most of the income of poor people is used up by their basic needs (food, transportation, housing)21.
Since a positive time preference ratio is preferred, it may be difficult for patients to allocate their limited resources to interventions that have a smaller impact on their immediate well-being. Preventive interventions represent a perspective of better health status in the future, but for many, that choice may hinder the chances of access to other oral care services whose perception of well being is more immediate. Very poor people from middle-income countries tend to concentrate more on the present - surviving each day is the greatest challenge - with little margin to think and plan for the future22. The lack of life perspective for those populations makes the future very uncertain. In this context, choices are limited; as the saying goes: "a bird in the hand is worth two in the bush."
Ferreira23, while evaluating other data collected in the present work, showed that preventive care interventions done in clinical settings present a lower compliance rate. Only half of the patients agreed to participate; missing visits doubled and treatment dropout was 30% higher, as well as requests to lengthen the intervals between visits, compared with the other elective care services.
In high-income countries, the consumption of oral health care services tends to have a demand-inelastic behavior24. However, the priorities of the studied population, many accumulated needs (more than 75% of the elderly over 60 years was totally edentulous and more than 38% had never worn a total prosthesis because they had no access to it), similar cost of elective care, and extreme budget restriction, may affect their demand for preventive care. To maximize utility in a situation of extreme budget restriction, the resources tend to be allocated by shifting the indifference curve to achieve greater utility25; in this case, by including more treatment than prevention.
Access to treatment for that population represented greatly improved well-being and quality of life26. Fisher et al.27 consider that, when facing situations of major gains, people tend to have risk-averse behaviors. In this case, the choice of not investing in a future that seems uncertain to them should be understood as assuming a risk-averse behavior. In middle-income countries, the social status of a patient is a critical barrier for compliance with certain protocols required by free services, even when life is jeopardized28. The concept suggested by Birch & Ismail et al.29 probably applies here: some oral care may be in the best interest of the patient's oral health, but not in the best interest of that patient's well-being.
The results of the present study show that, concerning health services, emergency and preventive care and operative dentistry should be prioritized and expanded and, if funds are available, specialized care should be implemented. Concerning society, preventive care interventions done in the clinical settings should not be prioritized. Only health-promotion interventions with a population approach should be considered. The results also suggest that the decision process regarding health policies should consider what patients are willing to sacrifice to improve their well-being. In a situation of extreme scarcity of resources, it is unlikely that people will be indifferent to the out-of-pocket costs originating from the number of visits and the time spent to complete the treatment, because of the perceived gains with the care service endpoints. Finally, the results also indicate that, especially in middle-income countries, the adoption of a non-societal perspective may provide partial information that leads to resource allocation decisions that reduces society's well-being.
CONCLUSION
Priorities differ from the perspective of the service and of society. From the perspective of service, the costs for elective care, including prevention, were close to the costs of high-income countries. From the society's perspective, the CER for prevention in clinical settings was unfavorable to be recommended as priority for poor populations. The society's perspective is essential for making decisions on the allocation of resources.
Collaborators
CA FERREIRA was responsible for conceiving the work, collecting data, reviewing the literature, analyzing the data and writing the manuscript. CA LOUREIRO supervised the statistical analyses, data interpretation, discussion of results and made a final review of the manuscript.
REFERENCES
1. Teixeira HV, Teixeira MG. Public health financing in Brazil: the Siops experience. Ciênc Saúde Coletiva. 2003;8(2):379-91. [ Links ]
2. Donaldson C. Economic evaluation in dentistry: an ethical imperative? Dent Update. 1998;25(6):260-4. [ Links ]
3. Iglesias CP, Drummond MF, Rovira J, NEVALAT Project Group. Health-care decision-making processes in Latin America: problems and prospects for the use of economic evaluation. Int J Technol Assess Health Care. 2005;21(1):1-14. [ Links ]
4. Ferreira CA, Loureiro CA. Economy on health in focus on oral health: literature review. Epidemiol Serv Saúde. 2006;15(4):55-64. [ Links ]
5. Instituto Brasileiro de Geografia e Estatística. [database on the Internet]. Pesquisa Nacional por Amostra de Domicílios: acesso e utilização de serviços de saúde 2003 [acesso em 2006 Nov 18]. Disponível em: <http://www.ibge.gov.br/home/estatistica/populacao/trabalhoerendimento/pnad2003/saude/tab11.pdf. [ Links ]>.
6. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação Nacional de Saúde Bucal. Diretrizes da Política Nacional de Saúde Bucal [site da Internet]. [citado 2006 jul 17]. Disponível em: <http://dtr2004.saude.gov.br/dab/saudebucal/publicacoes/diretrizes_da_politica_nacional_de_saude_bucal.pdf> [ Links ].
7. Pucca Júnior GA. A política nacional de saúde bucal como demanda social. Ciênc Saúde Coletiva. 2006;11(1):243-6. [ Links ]
8. Loureiro CA, Araujo VE, Lopes MI, Ayres JR. Pesquisa de avaliação da utilização de um método sistemático de mudança em um serviço de saúde bucal - BEPREM, MG. UFES Rev Odontol. 2001;3(1):68-78. [ Links ]
9. Drummond MF, O'Brien BJ, Stoddart GI, Torrance GW. Methods for the economic evaluation of health care programmes. 2nd. ed. New York: Oxford University Press; 1997. [ Links ]
10. Phillips C, Thompson G. What is cost-effectiveness? [homepage on the Internet] Oxford: Hayward Medical Communications; 2003 [cited 2006 jan 21]. Available from: <http://www.jr2.ox.ac.uk/Bandolier/painres/download/whatis/Cost-effect.pdf> [ Links ].
11. Drummond MF, Davies L. Economic analysis alongside clinical trials. Revisiting the methodological issues. Int J Technol Assess Health Care. 1991;7(4):561-73. [ Links ]
12. Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al. Generalisability in economic evaluation studies in healthcare: a review and case studies. Health Technol Assess. 2004;8(49):3-4. [ Links ]
13. Doherty N, Hussain I. Costs of providing dental services for children in public and private practices. Health Serv Res. 1975;10(3):244-53. [ Links ]
14. Bolin KA, Shulman JD. Nationwide survey of work environment perceptions and dentists salaries in community health centers. J Am Dent Assoc. 2005;136(2):214-20. [ Links ]
15. Richards L, Symon B, Burrow D, Chartier A, Misan G, Wilkinson D. Undergraduate student experience in dental service delivery in rural South Australia: an analysis of costs and benefits. Aust Dent J. 2002;47(3):254-8. [ Links ]
16. Arrow P. Cost minimisation analysis of two occlusal caries preventive programmes. Community Dent Health. 2000;17(2):85-91. [ Links ]
17. Oscarson N, Kallestal C, Fjelddahl A, Lindholm L. Cost-effectiveness of different caries preventive measures in a high-risk population of Swedish adolescents. Community Dent Oral Epidemiol. 2003;31(3):169-78. [ Links ]
18. Kallestal C, Norlund A, Soder B, Nordenram G, Dahlgren H, Petersson LG, et al. Economic evaluation of dental caries prevention: a systematic review. Acta Odontol Scand. 2003;61(6):341-6. [ Links ]
19. Robert Y, Sheiham A. The burden of restorative dental treatment for children in Third World countries. Int Dent J. 2002;52(1):1-9. [ Links ]
20. Byford S and Raftery J. Perspectives in economic evaluation. BMJ. 1998;316(7143):1529-30. [ Links ]
21. Ramos CA. Aspectos distributivos do gasto público na saúde. Planej Polít Públicas. 2001;(24):189-268. [ Links ]
22. Giannetti E. O valor do amanhã: ensaio sobre a natureza dos juros. São Paulo: Companhia da Letras; 2005. [ Links ]
23. Ferreira CA. Avaliação econômica de centro de especialidades de saúde bucal do serviço público de Sabará-MG, Brasil [monografia]. Campinas: Faculdade São Leopoldo Mandic; 2006. [ Links ]
24. Chattopadhyay A, Slade GD, Shugars DA. Charges for oral health care during a period of economic growth in the US: 1987-96. J Public Health Dent. 2003;63(2):104-11. [ Links ]
25. Piola SF, Viana SM. Economia da saúde: conceitos e contribuição para a gestão da saúde [sítio na Internet]. Brasília: Instituto de Pesquisas Econômicas Aplicadas; 1995 [citado 2006 jul 15]. Disponível em: <http://www.ipea.gov.br/pub/livros/livro149.pdf> [ Links ].
26. Miotto MH, Loureiro CA. The effect of social-demographic characteristics on the impact of oral health in life quality. UFES Rev Odontol. 2003;5(3):6-14. [ Links ]
27. Fisher G, Kamlet M, Fienberg S, Schkade D. Risk preferences for gains and losses in multiple objective decision making. Manage Sci. 1986;32(9):1065-86. [ Links ]
28. Lignani Júnior L, Greco DB, Costa MC. Avaliação da aderência aos anti-retrovirais em pacientes com infecção pelo HIV. Rev Saúde Pública. 2001;35(6):495-501. [ Links ]
29. Birch S, Ismail AI. Patient preferences and the measurement of utilities in the evaluation of dental technologies. J Dent Res. 2002;81(7):446-50. [ Links ]
Recebido em: 31/10/2008
Aprovado em: 11/3/2009
* Correspondência para / Correspondence to: CA FERREIRA. E-mail: <chrisaf2005@gmail.com>.

{kind=link}
{kind=link}
{kind=link}
{kind=link}