










Serviços Personalizados
Artigo
 pdf em Português
pdf em Português Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.59 no.1 Porto Alegre Jan./Mar. 2011
ORIGINAL ORIGINAL
Epidemiology of periodontal status in dentate male adults of Jalore, Rajasthan, India: a cross sectional study
Epidemiologia do estado periodontal em homens adultos dentados de Jalore, Rajastão, Índia: um estudo transversal
Arvind TatikondaI; Santhosh KumarII,*; Jyothi TadakamadlaIII; Harish TibdewalIV; Prabu DuraiswamyII; Suhas KulkarniII
IDepartment of Periodontics. School of Dental Sciences, Krishna Institute of Medical Sciences University. Malkapur, Karad, Maharashtra, India
IIDepartment of Preventive & Community Dentistry, Vishnu Dental College. Bhimavaram 534 202, West Godavari District, Andhra Pradesh, India
IIIDepartment of Oral Medicine and Radiology, Vishnu Dental College. Bhimavaram, Andhra Pradesh, India
IVDepartment of Preventive & Community Dentistry, Darshan Dental College and Hospital. Udaipur, Rajasthan, India
ABSTRACT
OBJECTIVE: The purpose of this study was to investigate the epidemiology of periodontal status among dentate male adults in the general population of Jalore, Rajasthan using the Community Periodontal Index.
METHODS: The condition of the periodontium was assessed by the Community Periodontal Index with use of the Community Periodontal Index probe. A total of 648 male subjects belonging to five age groups, namely 12, 15, 18, 35-44 and 65-74, were selected by stratified cluster sampling technique and examined.
RESULTS: The proportion of total subjects with healthy periodontium was 9.7% and the mean number of healthy sextants was 1.7. Bleeding on slight provocation was the most commonly observed condition in all age groups, comprising 38.8% of the total subjects. The results showed that the proportions of subjects who reported bleeding, calculus and periodontal pockets decreased steadily with age and a high statistically significant difference was observed among various age groups (p<0.001).
CONCLUSION: The results indicate that the study population has more widespread and severe periodontal destruction than other populations. Hence, to maintain periodontal health in this population, appropriate preventive and periodic periodontal therapies should be provided.
Indexing terms: Epidemiology. Periodontal discases. Adult.
RESUMO
OBJETIVO: O objetivo deste estudo foi investigar a epidemiologia do estado periodontal em homens adultos dentados na população geral de Jalore, Rajastão, utilizando o Índice Periodontal Comunitário.
MÉTODOS: A condição do periodonto foi avaliada pela sonda Índice Periodontal Comunitário. Um total de 648 homens pertencentes a cinco faixas etárias, 12, 15, 18, 35-44 e 65-74, foram selecionados pela técnica de amostragem estratificada por conglomerados e examinados.
RESULTADOS: A proporção de sujeitos com um periodonto saudável foi de 9,7% e o número médio de sextantes saudáveis foi 1.7. Sangramento resultante de pouca provocação foi a condição observada mais comum em todas as faixas etárias, atingindo 38.8% da amostra. Os resultados mostraram que as proporções de indivíduos com queixas de sangramento, cálculo e bolsas periodontais diminuíram de forma constante com a idade e houve diferença significativa entre as várias faixas etárias (p<0.001).
CONCLUSÃO: Os resultados indicam que a população estudada apresenta uma destruição periodontal mais generalizada e grave que outras populações. Assim, para manter a saúde periodontal desta população, terapias periodontais preventivas adequadas e periódicas devem ser fornecidas.
Termos de indexação: Epidemiologia. Doenças periodontais. Adulto.
INTRODUCTION
Periodontal disease is one of the two major dental diseases that affect human populations worldwide at high prevalence rates1. The prevalence and severity of periodontal disease have been measured in population surveys in several developed and developing countries, and these studies were carried out with a wide range of objectives, designs, and measurement criteria2. The Community Periodontal Index (CPI)3 was introduced by the World Health Organization (WHO) to provide profiles of periodontal health status in countries and to enable countries to plan intervention programs for effective control of periodontal disease. In addition, CPI data may be helpful in the surveillance of oral health at country and intercountry levels. Although this index has certain shortcomings when used as a stand-alone means of assessing the extent and severity of periodontal disease, it has been widely used for descriptive periodontal epidemiologic studies and needs assessment in developed and developing countries.
Epidemiologic data available at WHO confirm studies which show that periodontal disease prevalence and severity tend to be high in older age groups as compared to younger age groups4.
The most severe score or sign of periodontal disease (CPI score 4) varies worldwide from 10% to 15% in adult populations; however, the most prevalent score in all regions is CPI score 2 (gingival bleeding and calculus), which primarily reflects poor oral hygiene.
In most epidemiologic studies carried out globally, significant relationships between socioeconomic status and periodontal disease have been observed; i.e., low income or low education contributes to poor periodontal disease status5-6.
However, socioeconomic data could not be retrieved from the study subjects of the present study. There is no systemic data on the oral health status of the present study population, hence the present study intended to investigate the prevalence and distribution of periodontal status among dentate male adults in the general population of Jalore, Rajasthan, using the Community Periodontal Index.
METHODS
The study area is located in the southwest part of Rajasthan, India, and it was divided into four strata according to geographic zones, namely Siana, Betala, Mailavas and Jalore city, and a cluster was selected from each strata. Free camps were organized in each cluster and whoever responded was included in the study. The individuals were examined using a mouth mirror and CPI probe in a mobile dental unit. The WHO sampling procedure (stratified cluster sampling) was used to collect the representative population and a sample of 648 subjects was selected belonging to WHO standard age groups, 12, 15, 18, 35-44 and 65-74.
Ethical clearance was obtained from the Ethical Committee of Darshan Dental College and Hospital, Udaipur.
The oral cavity was divided into six sextants and the index tooth from each sextant was examined for gingival bleeding, calculus and periodontal pockets7. When more than two teeth were missing or indicated for extraction in a sextant, the extant was excluded. Moreover, subjects aged 12 and 15 years were only assessed for bleeding and calculus, as suggested by WHO.
Clinical examination was performed by a single, calibrated examiner and the kappa coefficient for intra-examiner variability was 0.91 for periodontal data.
Statistical analysis
The chi-square test was used to assess the significant differences between the age groups for occurrence of bleeding, calculus and pockets. The data were processed by the SPSS/PC+ software (11.0 Version). p>0.05 was accepted as statistically not significant and p<0.001 was set to be highly statistically significant.
RESULTS
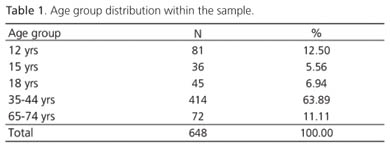
The distribution of age groups within the sample is shown in Table 1. A total of 648 subjects were included in the study, of which 414 belonged to the 35-44-year-old age group.
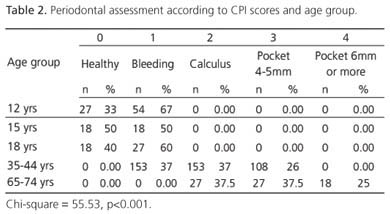
Bleeding on slight provocation was the most commonly observed condition in all age groups, affecting 38.8% of all subjects. Calculus and pockets were observed in the older age groups. Shallow pockets were observed in 20.8% of the total population, of which subjects in the 35-44-year-old and 65-74-year-old age groups contributed a major part, 26% and 37.5% respectively. Deep pockets of 6mm or more were only observed in the oldest age group, affecting 25% of these subjects. The majority (74%) of the subjects in the 35-44-year-old age group presented bleeding and calculus. None of the subjects in the oldest age group presented healthy periodontium or bleeding gingiva. The results showed that the proportions of subjects who reported bleeding, calculus and periodontal pockets decreased steadily with age and there was a high statistically significant difference among the various age groups (p<0.001).
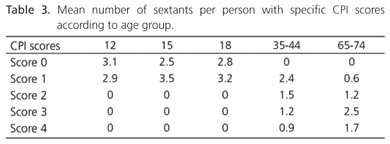
The proportion of subjects in the entire sample with healthy periodontium was 9.7% and the mean number of healthy sextants was 1.7. Healthy sextants without any periodontal disease were found in subjects of all but the oldest age group. The mean number of healthy sextants decreased as age increased. The greatest periodontal destruction was observed in subjects of the 65-74-year-old age group. They presented shallow probing depths in almost 2.5 sextants, deep probing depths in 1.7 sextants, and no excluded sextants.
Bleeding with gentle probing as a symptom of gingivitis was present in all age groups, particularly in the 15-year-old age group, affecting 3.5 sextants.
DISCUSSION
The study is an arid area with a water fluoride level of 4.5. It is a part of the Rajasthan fluoride belt where the majority of the population is of low socioeconomic status or below the poverty line. They have little access to formal health care services and particularly oral health; about 90% of the subjects have reported that they have never been to a dentist and completely rely on local quacks for their treatment. Our study also revealed poor oral hygiene habits in the study population; not one subject in the whole sample brushed his teeth twice or more than twice daily. The most commonly used oral hygiene aids were finger with tooth powder and Neem sticks.
Apart from poor oral hygiene habits, 60% of subjects, irrespective of age, have reported smoking or chewing tobacco.
The study planned to assess the periodontal status of the female population, but clinical examination could not be done as they were anxious and uncooperative when the examination was attempted by males.
The CPI criteria were used for determining the periodontal status, and despite some limitations, the system may provide reliable information on the important signs of periodontal disease8. This survey showed that bleeding and calculus were the most common problem in all age groups; less than 20% of the sample presented shallow periodontal pockets and very few participants presented deep pockets. Similar results were observed in the second national oral health survey of China by Wang et al.9 and Baelum et al.10. Destructive periodontitis was less frequent as supported by other studies11-14.
The prevalence of subjects with healthy periodontium (score 0) decreased with age. A similar trend was seen for bleeding on probing (score 1), whilst calculus deposit (score 2) was the main problem in all age groups over 35 years. Similar findings were reported in a study done by El-Qaderi and Quteish Ta'ani11. The prevalence of periodontal pockets was relatively high in older age groups, with 33.3-37.5% presenting shallow pockets (score 3) and 25% presenting deep pockets in the oldest age group. The present study found that the prevalence of periodontal disease in the 35-44-year-old age group was 100%, which is relatively higher than that of the general population of India in that age range, which is 89.6%15. A study done in Iran found a prevalence of 99%16.
Calculus was the most frequently observed periodontal condition in the 12, 15 and 18 age groups. The percentage of individuals with shallow and deep pockets was higher in the 35-44 and 65-74 age groups. Similar results were observed by Dini and Guimaraes17. The percentage of healthy adults decreased with age, in accordance with other studies18-22.
Participants under 35 years of age presented more than two healthy sextants, which is in agreement with the study done by Adegbemdo et al.23.
A major finding of this study was that no subject in the 35-44 age group had deep periodontal pockets whereas 0.3% and 12.5% of the population studied by Maity et al.24 in rural West Bengal, India, and by Mengel et al.25 in Yemen, respectively, had deep pockets.
In the entire sample, only 9.7% had a healthy periodontium. Similar findings were reported by Ahlberg et al.26 in Finland, Shizukuiski et al.27 in Japan, and Roman and Pop28 in Romania, where 6%, 7.4% and 9.34% of the industrial workers, respectively, had a healthy gingiva. Meanwhile, Hugoson and Jordan29 have reported a prevalence of periodontal disease in Finland of 100%.
The results of the present study show that the mean number of healthy sextants in the 35-44 age group is zero, while Mengel et al.25 have found 1.5 healthy sextants in the same age group in the Yemen upland, and Mumghamba et al.30 have found 2.5 healthy sextants in their study.
The mean number of sextants with deep pockets in the present study was 0.9, in contrast with the study done, who found an average of 0.1 sextants with deep pockets in 35-44-year-olds.
The mean number of excluded sextants (0%) in the surveyed population contrasts with those found in the general population of South East Asia (0.0 - 0.7), America (0.2 - 0.15), Europe (0.0 - 1.5), Africa (0.0 - 0.7), Middle East (0.0 - 0.1) and Western Pacific (0.0 - 0.9) and French Polynesia (1.7)20.
CONCLUSION
The results indicate that the study population has more widespread and severe periodontal destruction than other populations. Hence, to maintain periodontal health in this population, appropriate preventive and periodic periodontal therapies should be provided.
REFERENCES
1. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century - The approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl. 1):3-24. [ Links ]
2. Kingman A, Albandar JM. Methodological aspects of epidemiological studies of periodontal diseases. Periodontol 2000. 2002;29:11-30. [ Links ]
3. Pilot T. The periodontal disease problem. A comparison between industrialised and developing countries. Int Dent J 1998;48(Suppl. 1):221-32. [ Links ]
4. World Health Organization. The WHO Global Oral Health Data Bank. Geneva: World Health Organization; 2003. [ Links ]
5. Albandar JM, Tinoco EM. Global epidemiology of periodontal diseases in children and young persons. Periodontol 2000. 2002;29:153-76. [ Links ]
6. Borrell LN, Burt BA, Neighbors HW, Taylor GW. Social factors and periodontitis in an older population. Am J Public Health. 2004;94(5):748-54. [ Links ]
7. World Health Organization. Oral Health Surveys: basic methods, 4th ed. Geneva: World Health Organization; 1997. [ Links ]
8. Holmgren C. CPITN: interpretations and limitations. Int Dent J. 1994;44(5):533-46. [ Links ]
9. Wang HY, Petersen PE, Bian JY, Zhang BX. The second national survey of oral health status of children and adults in China. Int Dent J. 2002;52(4):283-90. [ Links ]
10. Baelum V, Pisuithanakan S, Teanpaisan R, Pithpornchaiyakul W, Pongpaisal S, Papapanou PN, et al. Periodontal conditions among adults in Southern Thailand. J Periodontal Res. 2003;38(2):156-63. [ Links ]
11. El-Quaderi SS, Queteish Ta'ani D. Assessment of periodontal knowledge and periodontal status of an adult population in Jordan. Int J Dent Hyg. 2004;2(3):132-6. [ Links ]
12. Garcia ML, Cutress TW. A national survey of periodontal treatment needs of adults in the Philippines. Community Dent Oral Epidemiol. 1986;14(6):313-6. [ Links ]
13. Oliver RC, Brown LJ, Loe H. An estimate of periodontal treatment needs in the U.S based on epidemiological data. J Periodontol. 1989;60(7):371-80. [ Links ]
14. Pilot T, Brames DE, Leclerco MH, Mc Combie BJ, Sardo-infirri J. Periodontal conditions in adults 35 - 44 years of age. An overview of CPITN data in the WHO Global Oral Data Bank. Community Dent Oral Epidemiol. 1987;14(6):310-2. [ Links ]
15. Bali RK, Mathur VB, Talwar PP, Chanana HB. National oral health survey and fluoride mapping, India. 2002 - 2003. New Delhi: Dental Council of India; 2004. [ Links ]
16. Hessari H, Vehkalahti MM, Eghbal MJ, Murtomaa HT. Oral health among 35- to 44-year-old Iranians. Med Princ Pract. 2007;16(4):280-5. [ Links ]
17. Dini EL, Guimarães LOC. Periodontal conditions and treatment needs (CPITN) in a worker population in Araraquara, SP Brazil. Int Dent J. 1994;44(4):309-11. [ Links ]
18. Guile EE. Periodontal status of adults in Central Saudi Arabia. Community Dent Oral Epidemiol. 1992;20(3):159-60. [ Links ]
19. Miller N, Benamghar L, Martin J, Abt F. An analysis of the CPITN periodontal treatment needs in France. Community Dent Health. 1987;4:415-23. [ Links ]
20. Miyazaki H, Hanada N, Andoh MI, Yamashaita Y, Saito T, Sogame A, et al. Periodontal disease prevalence in different age groups in Japan as assessed according to the CPITN. Community Dent Oral Epidemiol. 1989;17(2):71-4. [ Links ]
21. Pilot T, Barmes DE. An update of periodontal conditions in adults, measured by CPITN. Int Dent J. 1987;37(3):169-72. [ Links ]
22. Skaleric U, Kovac- Kavcic M. Periodontal treatment needs in a population of Ljubjana, Yugoslavia. Community Dent Oral Epidemiol. 1989;17(6):304-6. [ Links ]
23. Adegbembo AO, Adeyinka A, Danfillo IS, Mafeni JO, George MO, Aihveba N, et al. National pathfinder survey of periodontal status and treatment needs in the Gambia. SADJ. 2000;55(3):151-7. [ Links ]
24. Maity AK, Banarjee KL, Pal TK. Low levels of destructive periodontal disease in a rural population in West Bengal, India. Community Dent Oral Epidemiol. 1994;22(1):60-1. [ Links ]
25. Mengel R, Eigenbrodt M, Schünemann T, Florès-de-Jacoby L. Periodontal status of a subject sample of Yemen. J Clin Periodontol. 1996;23(5):437-43. [ Links ]
26. Ahlberg J, Tuominen R, Murtomaa H. Periodontal status among male industrial workers in Southern Finland with or without access to subsidized dental care. Acta Odontol Scand. 1996;54(3):166-70. [ Links ]
27. Shizukuishi S, Hayashi N, Tamagawa H, Hanioka T, Maruyama S, Takeshita T, et al. Lifestyle and periodontal health status of Japanese factory workers. Ann Periodontol. 1998;3(1):303-11. [ Links ]
28. Roman A, Pop A. Community periodontal index and treatment needs values (CPITN) in a factory worker group in Cluj-Napoca, Romania. Int Dent J. 1998;48(2):123-5. [ Links ]
29. Hugoson A, Jordan T. Frequency distribution of individuals aged 20 – 70 years according to severity periodontal disease. Community Dent Oral Epidemiol. 1982;10(4):187-92. [ Links ]
30. Mumghamba EG, Markkanen HA, Honkala E. Periodontal status and treatment needs in a rural area of Ukonga, Tanzania. Int Dent J. 1996;46(3):156-60. [ Links ]
Received on: 28/4/2010
Approved on: 11/6/2010
* Correspondence to: S KUMAR. E-mail: <santosh_dentist@yahoo.com>.
