










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
ORIGINAL / ORIGINAL
Public service dental actions in a small town
Ações odontológicas do serviço público em um município de pequeno porte
Ana Cristina Viana CAMPOS I; Carolina Marques BORGES I; Simone Dutra LUCAS I; Andréa Maria VARGAS I; Efigênia Ferreira e FERREIRA I
I Universidade Federal de Minas Gerais, Faculdade de Odontologia, Departamento de Odontologia Social e Preventiva. Av. Antônio Carlos, 6627, Pampulha, 31270-901, Belo Horizonte, MG, Brasil
ABSTRACT
Objective
To describe the actions of the public dental service in a small town in the Brazilian state of Minas Gerais.
Methods
An historical series study using secondary data obtained from the Outpatient Information System of the National Health Service in Brazil. The study sample consisted of all dental procedures and actions (n= 97.331) and basic medical actions (n= 126.340) performed between 2000 and 2007, as obtained from the Ministry of Health's official website.
Results
The percentage of basic dental actions (44%) was lower than the percentage of actions in the medical area (56%). Direct restorations, ignoring the number of tooth surfaces involved, were the most performed dental procedure (40%). The extractions of deciduous and permanent teeth (including root fragments) ranked second (35%), followed by preventive procedures such as scaling, curettage and crown polishing (11%), plaque control (8%), dental sealing (3%) and direct capping and pulpotomy (3%).
Conclusion
Given the data presented, it was possible to suggest that the dental service in this municipality was predominantly curative /restorative, to the exclusion of collective actions, that are not seemingly carried out and/or not recorded.
Indexing terms: Dentistry. Health service accessibility. National Health Service. Oral health.
RESUMO
Objetivo
Descrever as ações odontológicas do serviço público em um município de pequeno porte de Minas Gerais, Brasil.
Métodos
Estudo de série histórica com utilização de dados secundários obtidos através do Sistema de Informação Ambulatorial do Sistema Único de Saúde. A amostra do estudo foi composta por todos os procedimentos e ações básicas odontológicas (n=97.331) e ações básicas médicas (n=126.340) realizadas no período de 2000 a 2007 obtidos no site oficial do Ministério da Saúde.
Resultados
O percentual de ações básicas odontológicas (44,0%) foi inferior a percentual de ações da área médica (56,0%). As restaurações diretas - independentemente do número de faces dentárias envolvidas - foram o procedimento odontológico mais realizado (40,0%). As exodontias de dentes permanentes e decíduos (incluindo restos radiculares) ocuparam a segunda posição (35,0%), seguidos pelos procedimentos preventivos como a raspagem, curetagem e polimento coronário (11,0%), o controle de placa (8,0%), o selamento dental (3,0%) e o capeamento direto e a pulpotomia (3,0%).
Conclusão
Diante os dados apresentados, é possível sugerir que o serviço odontológico desse município predominantemente curativo-restaurador, em detrimento às ações coletivas que parecem não estarem sendo executadas e/ou registradas.
Termos de indexação: Odontologia. Acesso aos serviços de saúde. Sistema Único de Saúde. Saúde Bucal.
INTRODUCTION
Historically, dental care and assistance provided by the public sector in Brazil have almost exclusively given priority to schoolchildren between the ages of 6 and 12, and in the vast majority of instances, actions offered to the adult population focused on repair or removal1. When we compare different countries, Australia also fits this dental assistance profile, as 85% of dentists work in the private sector while the public sector is devoted to a small minority of the population2.
The situation is even less favorable when it is a matter of the rural population of Brazil and the native population, few studies having been conducted to characterize the conditions of access and the quality of the dental services offered to this sector of the population3. Moreover, the impact of oral health on people's quality of life is different when age, schooling and economic class4-5 are compared.
The fact that an individual has never in his life paid a visit to the dentist may be indicative of limited access to dental services, which allows us to characterize the essentially private nature of dental assistance in Brazil6.
Even after nearly 20 years since the implementation of the Brazilian National Health Service (SUS), the model based on the philosophy of getting the patience in and out as quickly as possible is still the one most frequently used in the primary oral healthcare services in Brazil, while the concept of total care seems to have made no headway in terms of actions that propose to improve the provision of dental services in the country7. An evaluation of the usage of dental services and the main factors associated with its limitations seems to be fundamental in helping with the effective scope of the challenge of universal access to health, as proposed by the National Health Service in Brazil8.
Based on these assumptions, the aim of the present study was to describe the dental actions of the public services in a small town in Brazil.
METHODS
The present study was of the historical series type, using secondary data obtained via the National Health Service's Outpatient Information System (SIA/SUS) in respect of the municipality.
SIA/SUS was implemented by the Ministry of Health in 1993 with the aim of recording and processing appointments, procedures and treatments performed in every health establishment, in a decentralized fashion9. The database, which may be accessed free of charge by the general public, is created by the National Health Service's Department of Technology (DATASUS) in cooperation with the National Epidemiology Center (CENEPI). SIA/SUS contains all the procedures conducted by health units, whether or not they are part of the Family Health Strategy. Production is entered on a monthly basis, including oral health activities within the scope of basic care.
The town is located in the south of the state, and has a population of around 10.537, 73.8% of whom live in the urban area; it has a Human Development Index (HDI) of 0.736, and the main source of revenue at the present time is historical tourism. In 2005, it had 9 public health establishments, 79 beds in private wards but no beds in public wards10. The Family Health Strategy and the initial dental consultation attained a coverage of 37.38% and 0.75%, respectively, in 2007.
The study sample was made up of all procedures and basic dental actions (n=97.331) and basic medical actions (n=126.340) performed between 2000 and 2007. The data available for review on DATASUS website referred to collective dental actions (n=76.067) were restricted to the period from 2000 to 2005 and those of health education (n=1.106) from 2000 to 2003. The use of data related to basic medical actions is justified by the fact that these actions may represent the level of access to health services in a particular town or country and, also by the secondary desire of the present study to compare the two types of basic dental actions to the medical ones. Despite the fact that data for 2008 are already available, they were not included since, from January that year, the system ceased to exhibit a specific table for each procedure, replacing it with just one table containing all procedures9.
The raw data relating to dental procedures and actions, as well as all the variables of interest to the present research, were obtained in March 2008, from the DATASUS web page (http://w3.datasus.gov.br/datasus/datasus.php). The construction of the database and the descriptive analysis were carried out using Excel for Windows 2007.
RESULTS
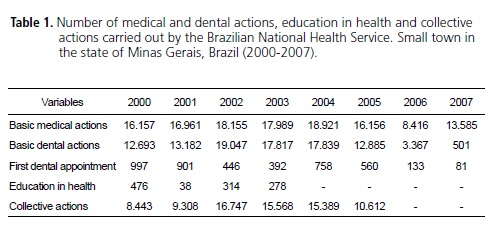
A total of 126.340 and 97.331 items were used of recorded data relating to basic medical and dental actions, respectively. In general, there is a predominance of basic actions of a medical nature (56%) when compared to dental (44%). As far as the basic dental services provided are concerned, an increase was noted in the number of dental procedures. In 2002, this number surpassed the number of medical actions, 19.047 and 18.155, respectively. Between 2002 and 2004, the number of dental actions remained constant and from this time forward, a drop has been noted, with only 501 recorded in 2007 (Table 1).
The lowest number found for activities of education in health was in 2001, namely 38. With regard to first-time dental appointments, the data revealed a sharp drop by 2003 but practically doubled the following year. From 2005, however, values have fallen drastically, as in 2007 only 81 dental appointments were recorded. Collective actions almost doubled between 2001 (9.308) and 2002 (16.747), but fell in subsequent years (Table 1).
Direct restorations, regardless of the number of tooth surfaces involved, were the dental procedure most frequently performed (40%) between 2000 and 2007. Extractions of permanent and deciduous teeth (including root fragments) occupied second position (35%) among the dental procedures most carried out by the public health service. This was followed by preventive procedures such as scaling, curettage and crown polishing (11%), plaque control (8%) and dental sealing (3%). Direct capping and pulpotomy represented 3% of the total number of dental procedures performed (Table 2).
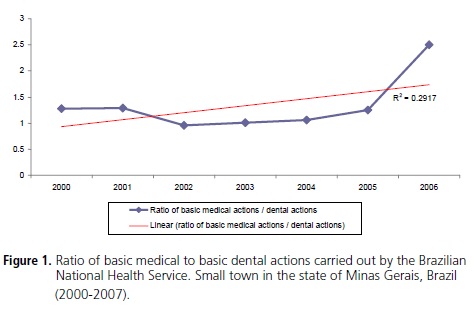
Basic medical actions remained twice as high as dental actions in the years under review, rising from 1.27 in 2000 to 2.49 in 2006 (r2=0.291) (Figure 1).

DISCUSSION
The time analysis of the ratio between basic medical and dental actions showed a slight declining tendency through 2004, and rose again the following year (r2=0.291). In 2007, this ratio was approximately 27 times higher, which could be indicative of reduced access to dental services. Access to medical appointments seems to be easier when compared to the dental service, even amongst exclusively National Health Service users.
The Family Health proposal is to work in teams so that all professionals consider themselves to be responsible, co-participants in the care provided to the public. In reality, there still exists an hegemony of the doctor figure in multi-professional teams, which is often reflected in the damage done through the quest to meet work targets and consequently to the service provided to the community11.
Access to services pervades the relationship between the need for health, the demand for and the use of health services. These three elements, when arranged in sequence, show that the "needs" of individuals in terms of health are transformed into "demand" which in turn generates the "use" of the services, provided that access to them is guaranteed4.
Table 1 shows that, over the seven year period, it was only in 2002 that dental actions exceeded medical actions. This result concurs with data from the 1998 National Household Sample Survey (PNAD/1998) which demonstrated a much lower proportion of dental appointments funded by the SUS. One study in the Metropolitan Region of Belo Horizonte revealed that 74% of adults had at least one medical consultation within the previous 12 months12.
The use of dental services represents an important resource in the effective scope of the universalization of access to health proposed by the SUS8. In addition, it is known that the use of dental services with the appropriate regularity and frequency contributes to maintaining oral health, whether it be by way of early treatment or through the prevention of disease at all ages7.
In a study conducted in the town of Sobral, it was found that, despite the need for increased coverage, 84.5% of dental appointments for children occurred through the public service. However, it should be borne in mind that 49.1% of these children had no access to any form of dental service, even though they were in the age range considered to be priority by the health programs8.
In the present study, a reduction was perceived in the number of first-time dental appointments, mainly after 2005. A first-time dental appointment may be regarded as the initial route of access to the public dental service. However, it should be stressed that it would be hard to regard such a session as representing the servicing and oral healthcare of the population. Moreover, we are dealing with raw data here, therefore we cannot confirm precisely if the cause is a reduction in access or an increase in the public attended, for example.
The absence of records relating to collective actions after 2005 and education in health after 2003 is an important point in the effective provision of the service as proclaimed by the SUS, which no longer accepts care which is simply remedial. A study conducted in Pompeu showed that the public's complaints and unresolved problems represent years of repressed demand by virtue of the absence of any type of care that differs from the traditional model that focuses on the disease13.
Being aware of the difficulties faced by health teams, such as lack of space and scarcity of resources, it is to be hoped that the practices of education in health and collective actions are still in their incipiency in many towns and cities. In this context, it can be seen that preventive and educational actions are scarce and limited to particular age groups14.
While the services demonstrate difficulty in meeting dental care needs, collective actions in oral health can and should be carried out with the aim of controlling the indices of caries and consequently the need for restoration and extraction. The main limitation of this type of approach is not being able to promote the definitive inclusion of health habits into oral health, through not being enduring by nature15.
In Table 2, it can be seen that, over the seven year period, there were just 28 records of intensive therapeutic use of fluoride per session. This result is rather different from that suggested by the literature, as the indiscriminate use of fluoride gel, resulting from the preventionist movement, continues to the present day, and is the procedure most referred to by dentists. Dental preventionism came to the fore in the 1980s with the creation of the Brazilian Association of Preventive Dentistry (ABOPREV) which systematically proclaimed the virtues of applying fluoride gel in schoolchildren between the ages of 6 and 12, as a means to preventing dental caries14.
In a study comparing urban and rural areas, it was not possible to confirm if fluoridation of the water supply had had a significant impact on the prevalence of observed dental caries. Nevertheless, a greater prevalence of the disease was noted in the rural areas, indicating the need to broaden access to dental care and to preventive interventions with actions focusing on preventing the formation and development of the disease16.
With regard to the individual clinical procedures carried out between 2000 and 2007, 75% were direct restorations and extractions of permanent and deciduous teeth (including root fragments). This is still the situation in many towns in Brazil whose systems of dental service provision are still almost entirely based on restoration and extraction17.
Tooth loss is considered to be a problem for public health in Brazil18 and in the rest of the world19 due to the high prevalence rates, to the negative impact caused to the daily lives of individuals and to society. The most recent national inquiry into oral health, SB Brasil, revealed that 65%, 77% and 76% of adults living in the Southeast, North and Northeast regions, respectively, require the use of a lower prosthetic device. As for the need to use upper prosthetics, 33% of adults and 26% of elderly individuals living in the Southeast region require rehabilitation18.
Tooth extraction represents the vestiges of an oral health conception and practice that for a long time was concerned with eliminating dental pain (restoring normality) by establishing the abnormality of "not having teeth"20. The biggest challenge for the public services is how to revert this negative perception of oral health in the Brazilian population. It is necessary for preventive actions, educational actions and promotion in health to work in parallel in order to really promote a process of building new wisdoms and the incorporation of new healthy habits appropriate to the situation of each individual, each community, a better quality of life4,21.
From this perspective, the appreciation of oral health care could herald a new vision, based on the representations of society, so that they can express the subjectivity of the real situation, instead of being limited to technical questions that are not responding to the health needs of the Brazilian population17.
CONCLUSION
Given the presented data, it is possible to suggest that the dental service in this town is predominantly curative/restorative, to the detriment of collective actions that are not seemingly performed and/or recorded. Moreover, using the available databases, further studies that point out this fragility could help to improve the quality of this information.
Collaborators
ACV CAMPOS was responsible for the conception and preparation of the project, for the data collection and statistical analysis and the composition of the article. CM BORGES, SD LUCAS and AMD VARGAS participated in the composition and final revision of the article. EF FERREIRA participated in the analysis, composition and final revision of the article.
REFERENCES
1. Lacerda JT, Simionato EM, Peres KG, Peres MA, Traebert J, Marcenes W. Dor de origem dental como motivo de consulta odontológica em uma população adulta. Rev Saúde Pública. 2004;38(3):453-8. [ Links ]
2. Brennan DS, Luzzi L, Roberts-Thomson KF. Dental service patterns among private and public adult patients in Australia. BMC Health Serv Res. 2008,8:1.
3. Dumont AFS, Salla JT, Vilela MBL, Morais PC, Lucas SD. Índice de necessidade de tratamento odontológico: o caso dos índios Xakriabá. Ciênc Saúde Coletiva. 2008;13(3):1017-22.
4. Mesquita FAB, Vieira S. Impacto da condição autoavaliada de saúde bucal na qualidade de vida. RGO - Rev Gaúcha Odontol. 2009;57(4):401-6.
5. Figueiredo RMO, Wassall T, Flório FM. Freqüência de impactos dos problemas de saúde bucal na qualidade de vida: avaliação dos efeitos de características sócio-demográficas e do estilo de vida. RGO - Rev Gaúcha Odontol. 2006;54(1):11-6.
6. Manhães ALD, Costa AJL. Acesso a e utilização de serviços odontológicos no Estado do Rio de Janeiro, Brasil, em 1998: um estudo exploratório a partir da Pesquisa Nacional por Amostra de Domicílios. Cad Saúde Pública. 2008;24(1):207-18.
7. Martins AMEBL, Barreto SM, Pordeus IA. Uso de serviços odontológicos entre idosos brasileiros. Rev Panam Salud Publica. 2007;22(5):308-16.
8. Noro LRA, Roncalli AG, Mendes Júnior FIR, Lima KC. A utilização de serviços odontológicos entre crianças e fatores associados em Sobral, Ceará, Brasil. Cad Saúde Pública. 2008;24(7):1509-16.
9. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Regulação. Avaliação e Controle. Coordenação Geral de Sistemas de Informação. Manual do Sistema de Informação Ambulatorial (SIA): manual de orientações técnicas e atualização. Brasília: Ministério da Saúde; 2008.
10. Instituto Brasileiro de Geografia e Estatística. Canal: banco de dados. Cidades [citado 2009 Mar 10]. Disponível em: <http://www.ibge.gov.br/cidadesat/topwindow.htm?1>.
11. Nickel DA, Lima FG, Silva BB. Modelos assistenciais em saúde bucal no Brasil. Cad Saúde Pública. 2008;24(2):241-6.
12. Lima-Costa MF, Loyola Filho AI. Fatores associados ao uso e à satisfação com os serviços de saúde entre os usuários do Sistema Único de Saúde na Região Metropolitana de Belo Horizonte, Estado de Minas Gerais, Brasil. Epidemiol Serv Saúde. 2008;17(4):247-57.
13. Andrade KLC, Ferreira EF. Avaliação da inserção da odontologia no Programa Saúde da Família de Pompeu (MG): a satisfação do usuário. Ciênc Saúde Coletiva. 2006;11(1):123-30.
14. Almeida GCM, Ferreira MAF. Saúde bucal no contexto do Programa Saúde da Família: práticas de prevenção orientadas ao indivíduo e ao coletivo. Cad Saúde Pública. 2008;24(9):2131-40.
15. Souza GB, Nogueira de Sá PHR, Junqueira SR, Frias AC. Avaliação dos Procedimentos Coletivos em Saúde Bucal: percepção de adolescentes de Embu, SP. Saúde Soc. 2007;16(3):138-48.
16. Souza CER, Pamplona DF, Gonçalves L, Vale MJLC, Wassall MAJ, Boaretto P. Levantamento epidemiológico de cárie dentária - Barão Geraldo - Campinas - SP. RGO - Rev Gaúcha Odontol. 2007;55(4):363-8.
17. Roncalli AG. Levantamentos epidemiológicos em saúde bucal no Brasil. In: Peres MA, Antunes JLF. Epidemiologia em saúde bucal. Rio de Janeiro: Guanabara Koogan; 2006.
18. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação de Saúde Bucal. Projeto SB Brasil 2003. Condições de saúde bucal da população brasileira: 2002-2003. Resultados principais. Brasília: Ministério da Saúde; 2004.
19. World Health Organization (WHO). The World Oral Health Report 2003. Continuous improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Geneva: 2003.
20. Ferreira AAA, Piuvezam G, Werner CWA, Alves MSCF. A dor e a perda dentária: representações sociais do cuidado à saúde bucal. Ciênc. Saúde Coletiva. 2006;11(1):211-8.
21. Carvalho ES, Hortense SR, Rodrigues LMV, Bastos JRM, Peres AS. Prevenção, promoção e recuperação da saúde bucal do trabalhador. RGO - Rev Gaúcha Odontol. 2009;57(3):345-9.
 Correspondence to:
Correspondence to:
S KUMAR
e-mail: santosh_dentist@yahoo.com
Received on: 17/1/2010
Final version resubmitted on: 25/7/2011
Approved on: 1/9/2011
