










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
ORIGINAL / ORIGINAL
Solid waste management in private dental practices
Gerenciamento dos resíduos sólidos em serviços odontológicos privados
João Ferreira LIMA NETO I; Filomena Maria da Costa PINHEIRO II; Sílvia Maria NÓBREGA-THERRIEN III; Virgínia Costa PINHEIRO IV
I Faculdade Católica Rainha do Sertão, Curso de Odontologia. Quixadá, CE, Brasil
II Faculdade Católica Rainha do Sertão, Curso de Odontologia. Rua Juvêncio Alves, 660, Centro, 63900-000, Quixadá. CE, Brasil
III Universidade Estadual do Ceará, Centro de Ciências da Saúde, Departamento de Saúde Publica. Fortaleza, CE, Brasil
IV Universidade Federal do Ceará, Faculdade de Odontologia. Fortaleza, CE, Brasil
ABSTRACT
Objective
To check the management of solid waste in dental practices that generates risks to health and the environment. With this in mind, the aim of this study was to ascertain the management of solid waste in private dental practices in the municipality of Quixadá, Ceará, Brazil in 2009. More specifically it was to ascertain its management, segregation, packing, collection, storage and final discording.
Methods
This is a descriptive, exploratory and quantitative study. Out of a total of 15 dental practices in the municipality, 11 (73.3%) were included in the study. Data collection was conducted through a questionnaire applied to dentists in August 2009.
Results
It was found that 81.8% of establishments do not have a Health Service Waste Management Plan. Nevertheless, 90.9% of professionals perform waste segregation, 45.5% of the dentists perform the packing of biological waste in plastic bags, 63.7% pack amalgam waste in glass with water, 60% dispose of developers and fixers directly into the sewerage system and for the sharps, 60% use cardboard boxes. Most dentists dispose of garbage on the sidewalk and the public collection is made by a truck, there being no separate collection service, and they were transported to the landfill, where they do not receive the appropriate treatment.
Conclusion
The lack of a Health Service Waste Management Plan leads to many failures and the involvement of the public authorities is essential in order to prevent harm to health and the environment.
Indexing terms: Dental waste. Solid waste. Waste management.
RESUMO
Objetivo
Verificar o gerenciamento dos resíduos sólidos nos serviços odontológicos privados do Município de Quixadá, Ceará, no ano de 2009, mais especificamente, verificar esse gerenciamento, quanto à segregação, acondicionamento, coleta, armazenamento e destinação final.
Métodos
Trata-se de um estudo descritivo, exploratório e predominantemente quantitativo. De um total de 15 serviços odontológicos do Município, 11 (73,3%) fizeram parte do estudo. A coleta de dados foi realizada por meio de um questionário, aplicado aos cirurgiões-dentistas, no mês de agosto de 2009.
Resultados
Verificou-se que 81,8% dos estabelecimentos não possuem um Plano de Gerenciamento de Resíduos dos Serviços de Saúde, e ainda que 90,9% dos profissionais realizam a segregação dos resíduos e que 45,5% dos cirurgiões-dentistas realizam o acondicionamento dos resíduos biológicos em saco plástico comum, 63,7% acondicionam os resíduos de amálgama em vidros com água, 60% dispensam reveladores e fixadores diretamente na rede de esgoto e, para os resíduos perfurocortantes, 60% usam caixas de papelão. A maioria dos cirurgiões-dentistas acomoda o lixo na calçada e a coleta pública é feita por um caminhão, não havendo coleta diferenciada, sendo transportado para o aterro sanitário e sem tratamento correto.
Conclusão
A falta do Plano de Gerenciamento de Resíduos dos Serviços de Saúde leva a muitas falhas e é importante a presença do poder público no sentido de prevenir os danos que podem causar à saúde e ao meio ambiente.
Termos de indexação: Resíduos odontológicos. Resíduos sólidos. Gerenciamento de resíduos.
INTRODUCTION
With the development of technology and the disorderly growth of cities and also taking into account population growth and the incorrect way in which natural resources are being exploited, the environmental imbalance has brought to the surface the discussion on the environmental impacts caused, along with the implications for the health of the population.
One of the main problems that requires attention is the growing output of solid waste and its impact on the health of the general public. With this broader concept of health, resulting from its determining and conditioning factors, the correct management of waste has become an essential issue in the preservation of people's health and quality of life.
Amongst the various sources of refuse, solid waste from the health services, despite it representing a small proportion of the total solid waste generated in the urban milieu, is the subject of some debate as it presents a worrying health risk and leaves behind irreparable environmental consequences by virtue of its improper management, resulting from the material's biological, chemical and physical properties.
According to the Health Services Waste Management Manual1, of the149,000 tons of household and commercial waste produced every day in Brazil, just a fraction, less than 2%, is made up of solid waste from the health services and, of this, only 10% to 25% requires special treatment. These remnants are a significant part of the total urban waste, not because of the quantity generated but on account of the potential risk they represent to health and the environment.
Ministry of Health resolution RDC 3062 of December 7, 2004, which establishes the Technical Regulations for the management of solid waste in the health services, constitutes a set of administrative procedures, planned and implemented based on scientific, technical, legal and normative foundations, with the aim of minimizing the production of waste and providing the refuse generated with safe, efficient disposal, aimed at protecting workers and preserving public health, natural resources and the environment.
The above mentioned Resolution defines those generating solid waste in the health services as any service related to human or animal healthcare, including the services of home visits and fieldwork; analytical laboratories for health products; morgues, funeral homes and services where embalming activities are performed (the preparation and preservation of corpses); coroner services; drugstores and pharmacies, including manipulation pharmacies; education and research establishments in the area of health; zoonosis control centers; pharmaceuticals distributors, importers, distributors and manufacturers of materials and controls for in vitro diagnosis; mobile healthcare units; acupuncture services; tattooing services, amongst others of a similar nature.
Waste generated in the dental services promotes a risk to public and occupational health which is equivalent to the refuse of the other healthcare establishments. This waste is made up of several different orders, such as biological, chemical, sharps and common materials3. In this list we might highlight the following: clinical waste, body parts, amalgam leftovers, disinfectant solutions, solutions used for processing radiographic film, lead plates from radiographic filming and drugs that are inappropriate for use.
As the waste generated in Dentistry causes risks to public and occupational health, and as these risks are also closely related to its internal and external handling, the way it is segregated and therefore managed in health establishments, on the basis of these considerations, the need has emerged to study these two types of handling (internal and external). In addition, we are obliged to check compliance with the management of this solid waste as far as segregation, packing, collection, storage and final disposal are concerned, in the case of private dental practices in the city of Quixadá (state of Ceará).
Based on this context this study is charged with social importance to the community, the environment and the profession since waste, when properly managed, contributes to better quality at work, both for the professional and for the public.
METHODS
A predominantly quantitative methodology, of a descriptive and exploratory nature, was employed in this 2009 study undertaken in Quixadá, in the Brazilian state of Ceará in 2009, within the city's private dental practices.
We used as the field for investigation the city's private dental practices through the dental surgeons that work in these locations, a total of 15 practices belonging to 15 professionals. The study group corresponded to 11 practices / dental surgeons (73.3%). The subjects included in the study were those dental surgeons in the health establishments investigated who agreed to take part in the study.
Data was collected in August of the afore mentioned year. Contact was made with the dental surgeon responsible for the practice in order to present the study and to request the participation of his/her health establishment in the investigation.
Afterwards, having obtained the proper authorizations, the investigation tool was applied, namely a semi-structured questionnaire where the dentists were asked about the system used for managing the waste they produced. The first part of the questionnaire dealt with questions concerning general information, while the second part covered the handling of the waste, from its packing to final disposal, with the aim of obtaining data for the study. The free and informed consent form was employed.
Observing the ethical aspects established in the National Health Council's Resolution 196/96, the study was submitted and approved by the Ethics Committee in Research at the Ceará Dental Academy, filed under case no. 95. The study presented no risk to the subjects as the information collected from their participation did not enable them or their health establishment to be identified. Neither did it result in any form of loss or financial cost.
RESULTS
The study population corresponded to the 15 private dental practices in the city of Quixadá, in the Brazilian state of Ceará. All of these health establishments were visited by one of the researchers who, at the time of the presentation of the study project, requested the participation of each of them. Of the total of dental surgeons, 11 answered the questionnaire, two refused to take part in the study and two received the questionnaire but did not answer it. The sample size, therefore, was 73.3% (11 dental surgeons).
The dental surgeons were questioned about general information concerning the system of waste management in their dental practices. With regard to the existence of a health service solid waste management plan in their establishments, 81.8% (9) of those investigated answered that they did not have such a plan. They were also questioned as to whether they were aware of the regulations of the Brazilian National Health Vigilance Agency (ANVISA) in respect of health service waste management. A total of 54.5% (6) of dental surgeons replied that they were aware of the regulations while 4.5% (5) were not. When questioned if they had participated in any training on this topic, 72.7% (8) professionals responded that they had never had any training while 27.3% (3) of them stated that they had.
When queried about which members of staff participate in the handling of waste in the practice, 90.9% (10) professionals responded that it is the dental hygiene assistants that carry out the activity and 9.1% (1 professional) stated that, in addition to the dental hygiene assistants, the general services employee also took part in the handling operation.
As for the handling of waste in these health practices, it was investigated whether separation of waste was being conducted according to the properties of the rubbish. We found that 90.9% (10) of professionals carry out separation while 9.1% (1) did not carry out any segregation in their health practice.
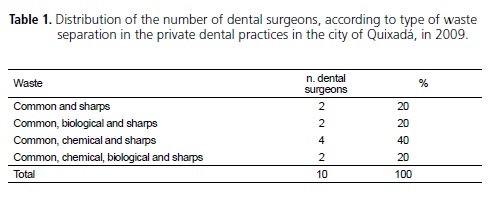
The 90.9% (10) of professionals who stated that they carried out waste separation in their establishment were questioned as to what type of material was segregated, the results of which are shown in Table 1.
With regard to the method of packing health services solid waste that is classified as biological, such as gloves, caps, masks, dressings, cotton wool and the remains from surgical procedures in the dental clinic, we were able to ascertain that 45.5% (5) of the professionals pack biological waste from their establishments in common plastic bags and 36.3% (4) of professionals packed it in white bags.
As for health service waste of a chemical nature emanating from these dental practices, such as expired anesthetics and dental products, 27.3% of subjects packed this waste in common plastic bags, 27.3% disposed of it in cardboard boxes and 18.1% in white bags, while 2 professionals responded that they use the products before expiry date and 1 replied that he did not make use of this type of material in his clinic.
In relation to the packing, in these dental practices, of health service solid chemical waste such as amalgam residue, we were able to ascertain that, of the 11 dental clinics, 36.3% (4) of professionals packed their waste in plastic containers with water, 63.7% (7) disposed of the waste in glass bottles containing water and one did not use amalgam.
On investigating the disposal of developers and fixers, we found that 60% (6) of the dental practices that use them get rid of these products directly into the sewage system, while 40% (4) place them in plastic containers for subsequent treatment and one does not use these materials in his clinic.
The dental surgeons were queried as to the packing of sharp waste; 60% use cardboard boxes, 30% plastic storage and 1 dental surgeon stated that he did not use this type of material. As for the location where the rubbish is placed after removal from the surgery, 54.5% (6) of dental surgeons stated that they placed it directly outside the health establishment and 45.5% (5) deposited it in a suitable temporary storage location.
As for the frequency with which the rubbish is removed from the dental surgery, all of them assumed it to be on a daily basis. They were, in addition, asked if they performed any treatment on contaminated waste in order to lessen the risks and just one professional (9.1%) responded that the files and drill bits underwent autoclave sterilization prior to disposal. The remaining 90.9% did not carry out any form of treatment.
On removal from the private dental practices, 81.1% (9) of the dental surgeons assumed the rubbish was deposited on the sidewalk, while 9.1% (1) professional advised that he deposited the remnants in containers and one other dental surgeon (9.1%) stated he left it in the collection cart. All the surgeons also stated that the public refuse collection is daily and that it is carried out by a dump truck (90.9%). Only one (9.1%) professional stated that it was performed by truck and by the sweepers' rubbish carts. 90.9% (10) of the professionals also stated that there is no separate collection for health service solid waste and one (9.1%) reported that he did not know.
DISCUSSION
According to the Brazilian National Health Vigilance Agency's resolution RDC 306/042, health services should produce a Management Plan for Health Service Waste based on its characteristics and classification, establishing handling policies which should cover the various stages of planning such as physical resources, materials and human resource training. The results of this study show a lack of knowledge by the majority of professionals in regard to the management of the waste in their establishments, ranging from knowledge of the standards that govern it to having a management plan and staff training. Perhaps the involvement of the Public Authorities would be of interest in this regard as, besides the ANVISA standards, these health services should also be guided by the local standards in force.
The Health Services Waste Management Plan is a document that should be produced by the generator of the waste, based on the characteristics of the waste produced, and should be compatible with local standards related to collection, transportation and final disposal, as established by the local agencies responsible for these stages2. The city of Quixadá does not yet have a local regulation in force, just the requirement for health establishments to have a health agency license. The agency carries out annual inspections.
As far as handling is concerned, we were able to ascertain that almost all dental practices perform it. Segregation of waste at the point of generation is one of the most important steps in its management, since it provides identification and classification according to its properties and also reduces the volume of infectious material as, when mixed with common waste, the latter is also deemed to be infectious. Without proper segregation, all the other management steps are compromised.
As regards the type of material with which separation is performed, it was found that all these professionals segregate sharp waste, which denotes an awareness of and responsibility for these materials, while for other types of material certain failures are still being noted. The risk with the handling of Health Service Waste is mainly related to accidents that occur due to defects in the packing and segregation of sharp materials without the use of mechanical protection1.
In respect of the methods for packing health service solid waste classified as biological, such as gloves, caps, masks, dressings, cotton wool and waste from surgical procedures conducted in the dental surgery, we were able to ascertain that 45.5% (5) of professionals pack biological waste from their establishments in common plastic bags and 36.3% (4) of these professionals pack using white bags, as recommended by ANVISA4, which also establishes that these bags should be replaced when they reach 2/3 capacity or at least every 24 hours and that it should also be identified as per item 1.3.3 of resolution RDC 306/04. Compared to a similar study by Pedrosa et al.5, the author obtained information that for this waste, in Campina Grande, Pernambuco, in 2006, the majority (81.1%) of private clinics packed material in other types of bags in a variety of colors, without any specification as to the infectious nature, and it was not segregated from common rubbish.
In terms of health service solid chemical waste from these dental practices, such as anesthetics and expired dental products in the dental surgeries, according to ANVISA4 packing should be performed in separate containers, observing the requirements for the waste's chemical compatibility with the packing materials, so as to avoid chemical reactions between the components, weakening it or degrading it, or the possibility that the packing material could be permeable to the components of waste. It should then be dispatched to licensed final disposal systems. The fact is that 27.3% of subjects pack this waste in common plastic bags, 27.3% use cardboard boxes for packing, 18.1% (2) use white bags, two professionals replied that they used all products before expiry date and one responded that he did not use this type of material in his surgery. A total of 45.4% (5) of the subjects followed ANVISA guidance in that they were segregated and packed separately.
In relation to the packing by these dental practices of health service solid chemical waste such as amalgam, we were able to ascertain that all those practices using amalgam perform segregation of material, denoting responsibility as to its disposal. According to Resolution 257/99 of the National Environmental Council (CONAMA6), batteries and accumulators containing lead (Pb), cadmium (Cd) and mercury (Hg) and their compounds should be disposed of. Waste containing mercury (Hg) should be packed in water-sealed containers and sent away for recovery4. Nazar et al.7 state that glycerin is recommended more so than water for storing mercury waste, plastic containers being more highly recommended than glass containers, which break easily. Storage should be in a dry, ventilated location, free from exposure to high temperatures (away from autoclaves, for example) and from risk of collision (people or cart traffic)8.
It is worth pointing out that when small particles of amalgam are introduced into the local sewage system, they contaminate the environment because, despite it being mixed with an alloy, the mercury in the amalgam could be released via natural chemical reaction, heat, shaking and changes in pH that occur in the environment which could lead to bio-accumulation and bioincorporation into the food chain9.
As far as the disposal of developers and fixers in the dental practices is concerned, according to the guidance issued by ANVISA in resolution RDC 3062 of December 7, 2004, the former may be subjected to neutralization in order to achieve a pH between 7 and 9, being subsequently discharged into the sewage system or receiving water body. Meanwhile, the latter may be submitted to recovery of the silver or be sent away to a Class I hazardous waste landfill or be submitted to treatment as per the guidance of the local environmental agency, in purpose-specific installations2. According to the results, there are deficiencies in this sector with regard to some of the dental practices (60%), as they discharge these products directly into the sewerage system. This waste can pass through a recovery and recycling process for subsequent reuse, thereby increasing the useful life of the septic drains and diminishing the impacts caused to the environment10.
Dental surgeons were questioned about the packing of sharp waste and it was discovered that 60% use cardboard boxes, 30% plastic containers and 1% use a rigid plastic container with material identification, while 1 dental surgeon stated that he did not use this type of material. The handling risk of this waste is high due to its potential for contamination and accidents, requiring safe handling and packing standards. The results demonstrate the awareness of these health establishments with care in the packing of this waste, using for the packing rigid containers, with a sealable lid, watertight, resistant to rupture or puncture, as recommended by ANVISA2.
According to instructions in ANVISA's resolution RDC 306/042, temporary storage may be dispensed with in cases where the distance between the point of generation and external storage so justifies. As the majority of the establishments investigated (7) are just surgeries and not clinics containing more than one surgery, perhaps this explains the result of 54.5% (6) of dental surgeons placing waste directly outside the health establishment.
In investigations concerning external storage of this waste, note that no exclusive external environment exists to this end, while awaiting collection. This has an impact on the health of the population, on workers and on environments, since this waste, exposed on the sidewalk, imposes serious risks. It is an alert to the Public Authorities in relation to this fact, in the sense of ordering, guiding and inspecting these health services. Article 225 of Brazil's 1988 Federal Constitution11, which refers to the environment, imposes on the Public Authorities and on society in general a duty to protect it and preserve it for both current and future generations.
According to Article 32 of Ceará12 state law 13103 of January 24, 2001, which establishes the state's policy on solid waste and provides related measures, transportation, treatment and final disposal of health service waste shall be the responsibility of the generator and must be segregated at source, with treatment and final disposal in systems authorized and licensed by the appropriate health and environmental agencies. According to information from the Urban Development Department of the city under review, the collection of health service solid waste only exists for the public health services and with regard to final disposal they stated that this waste is deposited in the sanitary landfill in a ditch, separated from common rubbish. As no separate collection exists for private health services, we were able to ascertain that the final disposal of health service waste from private clinics is the same as for common rubbish. So we were able to confirm what Monteiro et al.13 tell us, that the problem of final disposal takes on alarming proportions, observing a generalized action by local public administrations over the years to just get rid of the collected waste from urban zones, and depositing it at times in totally inappropriate locations.
The reality in Brazil is that the final disposal of Health Service waste is still inadequate and the health services should take responsibility for its management at a local level. This happens equally in other Latin American countries in that they do not get special treatment, its final disposal being the same location used for the disposal of other urban waste14. Through adequate management of this waste, the occurrence of infections in places where it is generated can be avoided, as well as minimizing or avoiding damage to the environment15.
Pedrosa et al.5 show us in a similar 2006 study in Campina Grande, in the state of Pernambuco, that even with proper packing, dental surgeons are faced with the problem of where to discard the waste once accumulated. Then there are those who report that they bury the waste or dispose of it in their bins along with common rubbish. When questioned as to the final disposal of the waste produced, 67% of dental surgeons stated they knew nothing about it and 31% believed that the disposal was performed in the landfill.
It is essential to discuss joint responsibility for production, management and final disposal of this waste which spans professional and staff liability, its correct treatment and the training of professionals in the correct handling, liability of public authorities via their overseeing agencies and the responsibility of society, so that we may have protection for the population and the environment.
CONCLUSION
In the majority of private dental practices in the city of Quixadá, professionals are largely unaware of the waste management in its establishments, ranging from the standards that govern it to having a Health Service Waste Management Plan and staff training.
A large number of the professionals carries out separation of waste, and all of them segregate sharps, denoting an understanding of and responsibility for this waste, while for some other types of waste a number of failures are still being noted.
As regards the method used for packing biological waste, almost one half of the health services pack biological waste in common plastic bags. As for health service chemical waste, such as amalgam waste, we found that all the professionals put it into plastic containers in water or in glass containers with water, while they still discharge developers and fixers straight into the sewerage system.
As regards the packing of sharp waste, the results demonstrate that these health establishments have an awareness of the care required when packing, using rigid containers with sealable, watertight lids that are resistant to rupture and puncture, as recommended by ANVISA.
With regard to the place where the rubbish is deposited after being removed from the surgery, the dental surgeons stated that they placed it right outside the health establishment or in a suitable temporary storage location, while just one professional performed some technique for treating contaminated waste in order to reduce the risks.
Almost all of the subjects said they deposited the rubbish on the sidewalk. Note that no form of external storage exists for this waste, where it may be deposited in an environment that is exclusive to this end, awaiting collection. This has an impact on the health of the population, workers and environments as, when exposed on the sidewalk, it imposes serious risks.
According to the majority of dental surgeons, public collection of this health service waste is conducted by a dump truck. They also stated that there is no separate collection for health service waste. The final disposal of health service waste, according to the Urban Development Department for the city, is separate, but only for the public health services. The results point to a lack of conditions offered by the city's public sector for the correct disposal of this waste.
Collaborators
JF LIMA NETO was responsible for the survey of the bibliography, data collection, tabulation of data and the composition of the article. FMC PINHEIRO was responsible for data searches, data analysis and composition of the article. SM NÓBREGA-THERRIEN contributed to the analysis of data, composition and revision of the article. VC PINHEIRO was responsible for data searches, composition and revision of the article.
REFERENCES
1. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Manual de gerenciamento de resíduos de serviços de saúde. Brasília: Ministério da Saúde; 2006.
2. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Resolução n. 306, de 7 de dezembro de 2004. Dispõe sobre o Regulamento Técnico para o gerenciamento de resíduos de serviços de saúde. Official Gazette of the Union, Brasília (DF); 2004 Dec 10.
3. Silva LCF, Barcellos RMG. Gerenciamento de resíduos em serviços odontológicos. In: Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Serviços odontológicos: prevenção e controle de riscos. Brasília: Ministério da Saúde; 2006. p. 113- 20.
4. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Serviços odontológicos: prevenção e controle de riscos. Brasília: Ministério da Saúde; 2006.
5. Pedrosa HLO, Figueiredo RLQ, Albuquerque TTP, Costa EB. Avaliação dos cirurgiões-dentistas sobre o gerenciamento dos resíduos odontológicos produzidos na prática diária. Arq Odontol. 2007;43(4):125-30.
6. Brasil. Ministério do Meio Ambiente. Conselho Nacional do Meio Ambiente. Resolução n. 257, de 30 de junho de 1999. Dispõe sobre o descarte e o gerenciamento adequados de pilhas e baterias usadas, no que tange à coleta, reutilização, reciclagem, tratamento ou disposição final. Diário Oficial da União, Brasília (DF); 1999 Jul 22.
7. Nazar MW, Pordeus IA, Werneck MAF. Gerenciamento de resíduos sólidos de odontologia em postos de saúde da rede municipal de Belo Horizonte, Brasil. Rev Panam Salud Publica. 2005;17(4):237-42.
8. Alves-Rezende MCR, Rossi AC, Alves-Claro APR. Amálgama dentário: controle dos fatores de risco à exposição mercurial. Rev Odont Araçatuba. 2008;29(2):9-13.
9. Mota SM, Magalhães CS, Pordeus IA, Moreira NA. Impacto dos resíduos de serviços de saúde sobre o homem e o meio ambiente. Arq Odontol. 2004;40(2):111-206.
10. Ferreira DDM, Gorges J, Silva LE. Plano de gerenciamento de resíduos do serviço de saúde: o caso do setor odontológico de uma entidade sindical. Rev Cient Internacional. 2009;2(9):1-18.
11. Brasil. Constituição da República Federativa do Brasil: promulgada em 5 de outubro de 1988. 16ª ed. São Paulo: Ed. Saraiva; 1997. p.114.
12. Ceará (Estado). Superintendência Estadual do Meio Ambiente. Lei n. 13.103, de 24 janeiro 2001. Dispõe sobre a Política Estadual de resíduos sólidos e dá providências correlatas. Diário Oficial do Estado do Ceará, Fortaleza (CE); 2001 Fev 5.
13. Monteiro JHP, Figueiredo CEM, Magalhães AF, Melo MAF, Brito JCX, Almeida TPF, et al. Manual de gerenciamento integrado dos resíduos sólidos. Rio de Janeiro: IBAM; 2001.
14. Rosa HCB, Ulhôa N. Gestão dos resíduos do serviço de saúde no município de Passos (MG). Ciência Et Praxis. 2009;2(4):53-8.
15. Almeida RCF, Pinto SL, Nascimento AJR, Feitosa CR, Alencar PRP. Gerenciamento dos resíduos sólidos em unidades de saúde da família. Rev RENE. 2009;10(2):103-12.
 Correspondence to:
Correspondence to:
FMC PINHEIRO
e-mail: filomenapinheiro@ig.com.br
Received on: 7/6/2010
Final version resubmitted on: 2/11/2010
Approved on: 17/1/2011
