










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
ORIGINAL / ORIGINAL
Oral healthcare profile of a Brazilian state capital according to data from the Outpatient Clinic Information Database of the Unified National Health System
Caracterização do modelo de atenção à saúde bucal de uma capital estadual brasileira, utilizando o sistema de informações ambulatoriais do Sistema Único de Saúde
Letícia Lara LINHARES I; Ronaldo BORDIN I
I Universidade Federal do Rio Grande do Sul, Faculdade de Medicina, Departamento de Medicina Social. Ramiro Barcelos, 2600, 4º andar, sala 428, 90055-003, Porto Alegre, RS, Brasil
ABSTRACT
Objective
This study determined the oral healthcare profile of Porto Alegre, Rio Grande do Sul, Brazil.
Methods
Data on the oral care procedures provided by the public healthcare system of the municipality of Porto Alegre from 2000 to 2007 were obtained from the Outpatient Clinic Information Database of the Brazilian Unified National Health System and categorized according to their level of care (preventive and curative) and complexity (primary and specialty).
Results
Preventive and primary procedures represented 60.2% and 87.7%, respectively, of the procedures done during the study period. The number of procedures involving dental prostheses increased 1031%, endodontic treatments increased 153%, and primary surgical procedures decreased 48%.
Conclusion
The Municipal Department of Health does not have data on the oral health of the municipal population because there was no oral health management at the time. The Outpatient Clinic Information System proved to be an important tool for the assessment of the federal, state and municipal oral healthcare policies. The critical information it provides improves policy makers' decision-making, the purpose of any information system.
Indexing terms: Health management. Oral health. Public health dentistry.
RESUMO
Objetivo
Caracterizar o modelo de atenção à saúde bucal em Porto Alegre, Rio Grande do Sul, Brasil.
Métodos
Caracterização a partir de informações obtidas no banco de dados do Sistema de Informações Ambulatoriais do Sistema Único de Saúde, segundo procedimentos realizados por nível de atenção (preventivos e curativos) e complexidade (básicos e especializados), no período 2000-2007.
Resultados
Observou-se que os procedimentos preventivos representaram 60,2% da produção ambulatorial do período avaliado, enquanto os procedimentos básicos representaram 87,8%. Houve um aumento de 1031% na realização de procedimentos relacionados a próteses dentárias e de 153% nos tratamentos endodônticos, ao mesmo tempo em que ocorreu uma redução de 48% na produção de procedimentos cirúrgicos básicos.
Conclusão
A Secretaria Municipal de Saúde não dispõe de dados referentes à saúde bucal no município, pois inexiste, neste momento, uma coordenação de saúde bucal. O Sistema de Informações Ambulatoriais mostrou-se uma importante ferramenta na avaliação das políticas de saúde bucal nos níveis municipal, estadual e nacional, fornecendo, aos gestores, um material indispensável para a tomada de decisão: finalidade de qualquer sistema de informações.
Termos de indexação: Gestão em saúde. Saúde bucal. Odontologia em saúde pública.
INTRODUCTION
Historically, the oral healthcare services provided in Brazil have been of low complexity, that is, limited to curative and mutilating actions, and of limited access. Experiments with preventive treatments, on the other hand, were occasional, and are focused mainly on to the school population, with reduced performance of mediumand high-complexity oral healthcare procedures.
The consolidation process of the Unified National Health System (SUS) has increased the scope of discussions regarding the organization of healthcare so as to provide universal access, full scope of services, equality, decentralization, service hierarchization and social control. The dynamics of the said consolidation was based on the reorganization of primary healthcare by the Community Health Agents Program and Family Health Program, currently known as Family Health Strategy2.
Decentralization is one of SUS' pillars and, from the point of view of the 5.507 Brazilian municipalities, it means the creation, restructuring and implementation of municipal healthcare systems whose control is gradually and progressively transferred from the federation to the municipality3.
The decentralization process of the Brazilian healthcare actions began when the Basic Operational Norm (NOB) was published in 1991, but this norm did not change the municipality-state relationship significantly. This process began to consolidate in 1993, when NOB/93 was passed and the municipalities began to incorporate SUS with different degrees of autonomy, which depended on the type of management chosen by each municipality as provided by the law 8.142/1991. This law provided a formula that included population and epidemiological data for determining how much money the municipality would receive from the federal government.
Four transition options were made available: incipient, partial, considerable and full management4. In 1993, the Municipal Department of Health of Porto Alegre manifested interest in the incipient management5. In the next year, the responsibility for many healthcare facilities, hospital care for occupational diseases and accidents, and sanitary surveillance of marketed foods was transferred to the municipality.
In 1995, six municipal district managements were implemented. The Municipal Department of Health also assumed other responsibilities, such as hiring or outsourcing service providers, sanitary surveillance of daycares and healthcare facilities and programming of hospital admission authorizations.
In 1996, SUS Basic Operational Norm (NOB-01/96) was changed, proposing full control and responsibility for the citizens' health, to promote and consolidate full autonomy by the municipalities and Distrito Federal. The norm redefined the function of the municipal manager, and, consequently, the responsibility of the states, Distrito Federal and federal government, and advanced the consolidation of the principles that guide a universal and equity system4.
In that same year, the Municipal Department of Health of Porto Alegre implemented the ‘considerable management' level of autonomy. Since then, Porto Alegre has been responsible for many different services, such as primary healthcare facilities, outpatient clinics and specialty services, which were formerly controlled by state and federal governments through laws and sponsorship of all the procedures provided by SUS in the municipality, including those outsourced to private providers.
In 1998, Porto Alegre was eligible for the highest level of autonomy defined by NOB/96, which is full control of the healthcare system. Hence, control and responsibility for the healthcare services provided by SUS in Porto Alegre were transferred to the Municipal Department of Health. Healthcare would then be provided by a network of municipalized and outsourced services and included primary and specialty outpatient care, hospital admissions and treatments, and urgency and emergency care5.
According to Chagas6, the vast number of people without access to dental care associated with the efforts of dental health workers resulted in the publication of Ordinance number 1.444, in 2000. This ordinance established the inclusion of oral healthcare in the Family Health Strategy, which was later detailed by Ordinance number 267, passed in 2001, and named Reorganization of Oral Health Actions in Basic Healthcare. It defines the objectives and bases for the reorganization of oral healthcare actions by the Family Healthcare Strategy, clarifies the attributions of healthcare teams (dental surgeon, dental hygienist, dental office assistant), and defines the financing given to the teams and the minimum equipment and instruments required for assistance.
In addition to the cost of including oral healthcare in the Family Health Strategy, specialty services provided by SUS were very limited, corresponding to 3.5% of the total oral healthcare procedures. Thus, in 2004, Ordinance number 1.570/GM was published. It established criteria, norms and requirements for the implementation and licensing of dental specialty clinics and regional dental prosthesis laboratories. These clinics would provide specialty oral healthcare services, such as: diagnosis with emphasis on the diagnosis and detection of oral cancer, specialty periodontics, minor oral surgery of soft and hard tissues, endodontics and services for patients with special needs. Ordinance number 1.571, passed in that same year, guaranteed financial incentives for sponsoring and implementing the dental specialty clinics and regional dental prosthesis laboratories.
In 2006, Ordinance number 648 of the Ministry of Health approved the National Basic Healthcare Policy, which provided revision of the guidelines and norms for organizing primary healthcare provided by the Family Health Program and Community Health Agents Program. This ordinance explicitly included oral healthcare in primary healthcare, approaching the oral health of the population to the work of a multidisciplinary team.
The final report of the 10th National Health Conference in 1996 established that the federal, state and municipal departments of health must implement actions to provide full oral healthcare. These actions must guarantee access of the entire population to everything that promotes, preserves, corrects and rehabilitates oral health, including the most complex and specialty services, and always respecting the local needs.
A study done by the Health Department of the state of Rio Grande do Sul in 2003 investigated the oral health profile of the state's population and found that dental caries, periodontal disease, malocclusion, missing teeth and the consequent need of prostheses were the most common problems affecting the oral health of the population. The mutilation caused by an increasing number of tooth extractions beginning at adolescence and rehabilitation difficulties were the greatest problems found by the study. The need of reflecting about the dental practices provided by public services and their healing and technocentric logic with low social impact was evident7.
The health decentralization process has increased the use of information systems as planning and management instruments. Databanks with social development data (Municipal Human Development Index (HDI-M) and census) and health information systems, such as the Outpatient Clinic Information System (SIA) and the Basic Healthcare Information System (SIAB), among others, contain very useful population and municipal data. This information is valuable for the implementation of social policies and health programs, and for reorganizing and controlling oral healthcare actions8.
Health information systems are units that produce, analyze and disseminate data, and are an important component of the healthcare system. Their purpose is to promote the creation and facilitate the assessment of health policies, plans and programs, since their indicators reflect the population's health. They expose the diseases of the population, magnitude of their health problems, possible risk factors and epidemics. This knowledge allows the quantification of intervention efficiency and impact of sanitary practices9.
The only national systems with records of the procedures done by oral healthcare teams are SIA and SIAB. The latter is still under development with respect to oral healthcare actions. SUS' challenge is to turn innumerous data into useful information and information into the health portrait of the country, so that the public sector can indeed order and meet the population's needs9.
The municipal primary healthcare system of Porto Alegre consists of 117 health facilities and 84 Family Health Strategy teams, established in 1996. These 84 teams provide care to a population of 290.000. Each team consists of six community health agents, two nursing assistants, one doctor and one nurse. Each team is responsible for about 850 families, corresponding to 3.500 to 4.000 people. According the Municipal Department of Health, only seven oral healthcare teams have been included in the Family Health Strategy until this time10.
According to the Ministry of Health, less than 4% of the population of Porto Alegre is receiving oral healthcare from the Family Health Strategy. In 2008, there were 189 dental surgeons working in municipal healthcare facilities, of which 167 were general dental practitioners. During this same period, there were two modality-1 oral healthcare teams and five modality-2 oral healthcare teams. Modality-1 teams consisted of one dental surgeon and one dental office assistant and modality-2 teams consisted of one dental surgeon, one dental hygienist and one dental office assistant. Additionally, there were 5 specialty dental facilities, 3 regional dental prosthesis laboratories and 3 facilities providing care to people with orofacial deformities.
The objective of this study was to determine the municipal oral healthcare profile of Porto Alegre and for this purpose, data were on outpatient clinic services and costs were obtained from SIA-SUS. This database has already been used to determine the municipal oral healthcare profile of Cuiabá11, reorganization process of healthcare actions8, and relationships between decentralization of healthcare actions in Brazil and oral healthcare characteristics12.
The small number of studies in the literature analyzing SUS' oral healthcare policies motivated this study, whose objective was to use SIA-SUS data on outpatient clinic services to determine the municipal oral healthcare profile of Porto Alegre (RS).
METHODS
The general objective of this study was to characterize the municipal oral healthcare profile of Porto Alegre (RS) by analyzing SIA-SUS data on the outpatient services provided by the municipality from 2000 to 2007, and to categorize the services according to level of care (preventive or curative) and complexity (primary and specialty).
Secondary data about all the municipal outpatient oral healthcare services provided from 2000 (year in which oral healthcare was included in the Family Health Strategy) to 2007 in Porto Alegre were obtained from SIA-SUS, categorized and analyzed. Population-based calculations used the municipal population of the year in question. The yearly population was either determined by census or estimated by the Brazilian Institute of Geography and Statistics (IBGE).
The study procedures included all the oral healthcare procedures listed in SUS table and recorded in SIA-SUS. The procedures were then categorized by level of care (preventive or curative) and complexity (primary or specialty).
Primary procedures include (a) group procedures, such as supervised tooth brushing, fluoride rinse, topical fluoride application and mouth examination for epidemiological purposes; (b) individual procedures include first scheduled dental visit, therapeutic topical fluoride application, cariostatic agent application, sealant application, control of dental plaque, removal of caries, materia alba and calculus, and tooth polishing; (c) primary dentistry: caries removal, pulp capping, restorations with amalgam, composites, silicate, light-cured composite resin, glass ionomer and foundation restoration; (d) primary surgical dentistry: simple extraction of deciduous and permanent teeth, treatment of alveolitis, small bleedings, urgent procedures and ulotomy.
Specialty procedures include: a) specialty dentistry: restorations with glass ionomer; b) periodontics: periodontal surgery, gingival graft, gingivoplasty, gingivectomy, scaling, urgent periodontal treatment and subgingival curettage; c) endodontics: pulpectomy of deciduous and permanent teeth, endodontic treatment of deciduous and permanent teeth with one or more roots, endodontic retreatment of deciduous and permanent teeth with one or more roots and apicoectomy; d) specialty surgical dentistry: preprosthetic surgery, surgery for orthodontic purposes, periapical curettage, multiple tooth extractions, reduction of temporomandibular joint dislocation, glossorrhaphy, tooth transplantation and replantation, cyst removal, cyst marsupialization, removal of foreign bodies in the orofacial region, removal of retained teeth, removal of torus and exostoses, partial lip reconstruction, removal of salivary stones, removal of the submandibular gland, reduction of dentoalveolar fractures, surgical treatment of fistulas, ulectomy, tooth contention, and residual focus removal and tunneling; e) dental radiology: occlusal, periapical, interproximal and panoramic radiographs and cephalometric analysis; and f) dental prostheses: temporary crowns, recementation of inlays and onlays, removable total and partial dentures, temporary prostheses, contention plates, denture rebasing, porcelain-fused-to-metal post and core, primary and secondary impressions and follow-up of dental prostheses.
Of the abovementioned procedures, the preventive group and individual procedures were considered preventive. All other procedures were considered curative.
The procedures were categorized according to the outpatient clinic production from 2000 to 2007, which resulted in the municipal oral healthcare profile of Porto Alegre, considering the following: number of procedures per level of care to determine which practices prevailed (preventive versus curative); complexity; and scope of the services.
The study was based on analysis of data collected from public domain databases. Nevertheless, the project was approved by the Research Ethics Committee of the Federal University of Rio Grande do Sul School of Medicine, protocol number 14.738.
RESULTS
The procedures performed by the municipal outpatient oral healthcare clinics of Porto Alegre, according to SIA-SUS, organized by categories, are listed in Table 1. The number of each procedure did not vary too much yearly between 2000 and 2007. It is noteworthy that preventive group procedures became available in 2006 and increased 191.4% in 2007.
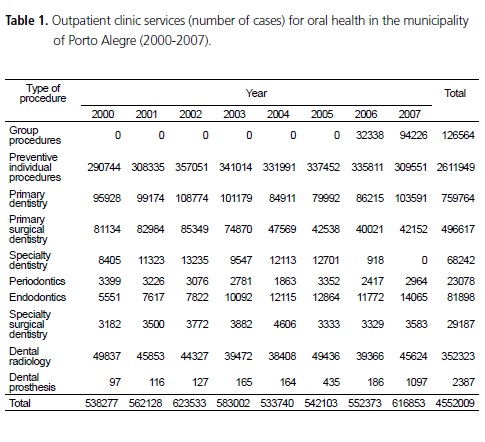
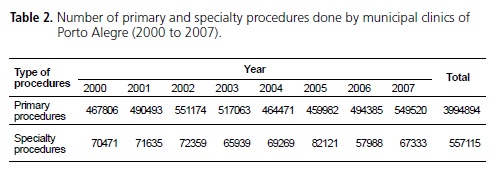
The production of dental prostheses increased 1.031% and endodontic treatments increased 153% between 2000 and 2007. On the other hand, primary surgical procedures decreased 52% over that period and specialty dentistry decreased 89.1% from 2000 to 2006 and reached a 100% decrease in 2007. Most (87.8%) procedures done at the municipal clinics were primary procedures (Table 2).
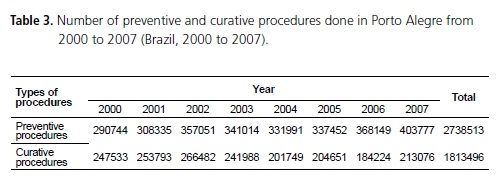
Preventive procedures increased 38.9% from 2000 to 2007 (Table 3). They also prevail over curative procedures, representing 60.2% of all the procedures done during that period.
DISCUSSION
According to SIA-SUS data, the total number of procedures done yearly by the municipal outpatient oralhealth clinics of Porto Alegre did not vary significantly from 2000 to 2007. According to Barros & Chaves8, database data on the most usual procedures, such as visits, tooth extractions and restorations, are reasonably reliable. Group procedures, because of their more recent nature, have serious input and standardization problems, so their reliability is questionable.
Procedures that required production of dental prostheses increased 1031%, going from 97 in 2000 to 1097 in 2007. In 2007, another two modality-2 dental specialty centers were inaugurated in the municipality, in addition to one more regional laboratory of dental prostheses. The number of endodontic treatments also increased progressively.
The number of endodontic procedures, which attempt to preserve dental structure, increased 153% from 2000 to 2007. On the other hand, there was a progressive decrease in the number of primary surgical procedures, which includes dental extractions, reaching a total decrease of 48.05% in 2007. However, it is not possible to state that these findings are related, since information is insufficient.
In 2002, the Municipal Department of Health found that there was a decrease in the number of dental extractions and an increase in the number of restorative procedures. The Department suggested that this increase could be stemming from better access to the services and earlier request for help, but concluded that the ratio between restorative and radical treatments, such as tooth extractions, was still high and far from ideal13.
In 2003, the Municipal Department of Health reported that the number of tooth extractions decreased in relation to total treatments performed. Although the decrease was not too steep and less than expected, it was considered a positive response to the recommendation of favoring conservative over radical treatments14.
Primary procedures were much more numerous than specialty procedures: 87.8% of the outpatient clinic production during the study period consisted of primary procedures.
The public oral healthcare provided in Brazil has been restricted almost entirely to primary procedures. Nevertheless, the pent-up demand is still very high. The most recent numbers indicate that specialty procedures correspond to no more than 3.5% of the total oral healthcare procedures provided by SUS. Its limited ability to provide secondary and tertiary care is evident, compromising the establishment of appropriate referral (patient's records sent from general dental practitioner to specialist) and counter-referral (patient's records sent from specialist to general dental practitioner) systems in oral healthcare in nearly all regional health systems. Expansion of the secondary and tertiary oral healthcare network did not accompany the increased supply of primary care services15.
The guidelines of the National Oral Health Policy provide for the expansion and improvement of primary care, access to all age groups, and more services, guaranteeing secondary and tertiary care so that full care is available. They emphasize the need of changing the oral healthcare profile. One of its suppositions is to assume the compromise of providing good quality primary healthcare, guaranteeing quality and problem resolution, regardless of the strategy used by the municipality to organize healthcare, and use family's health as an important guide for the reorganization of primary healthcare15.
Another proposal of the National Oral Health Policy provides for changing the oral healthcare profile by responding to a health conception that is not only centered on treating the diseased, but, most of all, promotes good quality of life and intervenes when quality of life is jeopardized.
Among the proposed measures is the progressive incorporation of health-promoting and protecting actions, such as fluorination of water, health education, supervised oral hygiene and topical fluoride applications. Except for water fluoridation, all other actions require dental surgeons, making them the protagonists of these actions.
According to data from the Municipal Department of Health, fluoridated water is available in 99% of Porto Alegre's households13. But according to SIA-SUS data, the number of preventive procedures increased exponentially during the study period while curative procedures decreased. Preventive procedures greatly outnumbered curative procedures.
CONCLUSION
In conclusion, preventive and primary practices prevailed in the municipality during the study period. The number of extractions tends to decrease while the number of conservative treatments tends to increase.
The current municipal administrators of Porto Alegre and, more specifically, of its Department of Health, have little information on the population's oral health because there is no oral healthcare coordinator or policy in force. The Department's annual reports with information on the population's oral health stopped being published in 2003.
Article 196 of the Brazilian constitution defined a broader concept of health. This concept must guide the change that healthcare requires, that is, transition from a disease-treating model to a holistic health model by implementing more actions that promote and protect health instead of only curative actions.
It is important to follow SIA-SUS always, since this system is an important tool for the assessment of federal, state and municipal oral healthcare policies, providing to public managers indispensable information for decision-making, which is the purpose of any information system.
Health professionals involved in the process should use epidemiology and territorial information to support planning. In other words, professionals should demand that actions be preceded by a family-based diagnosis of the population's health and a diagnosis of the relationships that emerge where health practices are provided. Finally, health professionals should use indicators to determine the impact of oral healthcare actions, which requires the existence of easy-to-use, reliable and updated databases.
Collaborators
LL LINHARES and R BORDIN conceived and designed the study, collected, analyzed and interpreted data, and wrote the article.
REFERENCES
1. Brasil. Ministério da Saúde. Brasil Sorridente: autorização para procedimentos de alto custo/complexidade (APAC) para prótese dentária total e prótese dentária parcial removível. Brasília: Ministério da Saúde; 2006.
2. Brasil. Ministério da Saúde. Portaria n. 267, de 06 de março de 2001. Dispõe sobre a reorganização das ações de saúde bucal na atenção básica. Diário Oficial da República Federativa do Brasil, Brasília (DF); 2001 Mar 6.
3. Scatena JHG, Tanaka OY. A descentralização da saúde no Estado de Mato Grosso, Brasil: financiamento e modelo de atenção. Rev Panam Salud Publica. 2000;8(4):242-9.
4. Brasil. Ministério da Saúde. Manual para a Organização da Atenção Básica Saúde. Brasília: Ministério da Saúde; 1999.
5. Heidrich AV. O Conselho Municipal de Saúde e o processo de decisão sobre a política de saúde municipal [dissertação]. Porto Alegre: Universidade Federal do Rio Grande do Sul; 2002.
6. Chagas RA. Política nacional de atenção à saúde bucal. In: Andrade LOM, Barreto ICHC. SUS passo a passo: história, regulamentação, financiamento e políticas nacionais. 2ª ed. São Paulo: Hucitec; 2007. p. 685-702.
7. Rio Grande do Sul (Estado). Secretaria Estadual de Saúde. 2ª Conferência Estadual de Saúde Bucal: relatório final. Porto Alegre: Secretaria Estadual de Saúde; 2004.
8. Barros SG, Chaves CL. A utilização do Sistema de Informações Ambulatoriais (SIA-SUS) como instrumento para caracterização das ações de saúde bucal. Epidemiol Serv Saúde. 2003;12(1):41-51.
9. Rio Grande do Sul (Estado). Secretaria Estadual de Saúde. Manual para sistema de informação em saúde bucal do SUS. Porto Alegre: Secretaria Estadual de Saúde; 2007.
10. Baldisserotto J, Luvison I. Saúde bucal na Estratégia Saúde da Família em Porto Alegre, RS. In: Moysés ST, Kriger L, Moysés SJ. Saúde bucal das famílias: trabalhando com evidências. Porto Alegre: Artmed; 2008. p. 125-35.
11. Volpato LER, Scatena JH. Análise da política de saúde bucal de Cuiabá, Estado de Mato Grosso, Brasil, a partir do banco de dados do Sistema de Informações Ambulatoriais do Sistema Único de Saúde (SIA-SUS). Epidemiol Serv Saúde. 2006;15(2):47- 55.
12. Chaves SCL, Silva LMV. Atenção à saúde bucal e a descentralização da saúde no Brasil: estudo de dois casos exemplares no Estado da Bahia. Cad Saúde Pública. 2007;23(5):1119-31.
13. Porto Alegre. Secretaria Municipal de Saúde. Relatório de Gestão Anual 2002. Porto Alegre: Secretaria Municipal de Saúde; 2002.
14. Porto Alegre. Secretaria Municipal de Saúde. Relatório de Gestão Anual 2003. Porto Alegre: Secretaria Municipal de Saúde; 2003.
15. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação Nacional de saúde bucal Diretrizes da política nacional de saúde bucal. Brasília: Ministério da Saúde; 2004.
 Correspondence to:
Correspondence to:
R BORDIN
e-mail: ronaldo.bordin@ufrgs.br
Received on: 7/12/2009
Approved on: 7/5/2010
