










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
ORIGINAL / ORIGINAL
Secondary dental care and implementation of specialized dental clinics in a state in Northeast Brazil
Atenção secundária em saúde bucal e a implementação dos Centros de Especialidades Odontológicas em um estado do Nordeste, Brasil
Denis Bezerra de ARAÚJO I; Léa Maria Bezerra de MENEZES I; Denise Lins de SOUSA I
I Universidade Federal do Ceará, Faculdade de Odontologia. Rua Monsenhor Furtado, s/n, Rodolfo Teófilo, 60430-350, Fortaleza, CE, Brasil
ABSTRACT
Objective
To describe the implementation of secondary oral health care services in the Brazilian state of Ceara, through secondary data on specialist dental clinics and the provision of specialist dental care.
Methods
Descriptive epidemiological study that used secondary data from the diagnosis of specialist dental clinics conducted by the Health Department of the state of Ceara and the production of secondary outpatient dental care recorded in the Outpatient Information System from 2000 to 2010.
Results
An increase was detected in the number of specialist dental clinics in the state, and consequently an increase in the recording of specialist dental procedures after 2004, showing a greater provision of such services to the population.
Conclusion
Despite the expansion of secondary oral health care services in the state of Ceara and the growing number of specialist dental procedures recorded in the Outpatient Information System of the National Health Service in the country as a whole, the capacity to solve the issues of these services is still considered to be a challenge for managers and professionals in oral health care, which may compromise the establishment of reference and counter-reference systems, having negative consequences on the doctrinal principles of the National Health Service in the state, such as universality of services, equitability and totality in health care.
Indexing terms: Dental health services. Dental specialties. Public health policy.
RESUMO
Objetivo
Descrever a implementação dos serviços da atenção secundária em saúde bucal no estado do Ceará, Brasil, através de dados secundários sobre os Centros de Especialidades Odontológicas e a oferta de atendimento especializado em Odontologia.
Métodos
Estudo descritivo que utilizou dados secundários do Diagnóstico Situacional dos Centros de Especialidades Odontológicas realizado pela Secretaria de Saúde do Estado do Ceará e da produção ambulatorial da atenção secundária em saúde bucal cadastradas no Sistema de Informações Ambulatoriais do Sistema Único de Saúde no período de 2000 a 2010.
Resultados
Constatou-se que houve um aumento expressivo do número de Centros de Especialidades Odontológicas implantados neste estado e, consequentemente, um aumento do registro dos procedimentos especializados em Odontologia a partir de 2004, evidenciando uma maior oferta desses serviços para a população.
Conclusão
Apesar da ampliação dos serviços de atenção secundária em saúde bucal no estado do Ceará e do aumento de procedimentos especializados em Odontologia cadastrados no Sistema de Informações Ambulatoriais do Sistema Único de Saúde neste estado, a resolutividade desses serviços ainda é considerada um desafio para os gestores e profissionais da assistência em saúde bucal, o que pode comprometer o estabelecimento de sistemas de referência e contra-referência, tendo consequências negativas sobre os princípios doutrinários do Sistema Único de Saúde como universalidade dos serviços, equidade e integralidade na assistência à saúde.
Termos de indexação: Serviços de saúde bucal. Especialidades odontológicas. Políticas públicas de saúde.
INTRODUCTION
The current National Policy on Oral Health, known as Brasil Sorridente ("Smiling Brazil"), was created by the Ministry of Health in 2004 with, amongst others, the aim of reorganizing oral health services at all levels, by strengthening and qualifying basic healthcare and broadening the population's access to specialist treatment in the public health system1-2. This policy was put together based on the results of the epidemiological survey entitled "OH Brazil – Oral health condition of the Brazilian population"3, which highlighted dental caries and its consequences (tooth pain and loss) and the lack of access to dental actions and services as the main oral health problems to be confronted4-5.
Access by the Brazilian population to basic dental services, such as restorations, extractions, topical fluoride application, amongst others, was expanded considerably following the inclusion of the dental health teams in the Family Health Strategy5-6. However, it was evident that there was a need for organization and expansion of the dental services system for cases of medium complexity, seeing as how, according to data published by the Outpatient Information System (SIA/ SUS)7 for the year 2003, the supply of specialist dental services corresponded to less than 3.5% of the total of basic dental care procedures3,8.
Accordingly, dental care in Brazil was almost exclusively confined to basic services, thus compromising the development of the system of reference for services of medium complexity, indicating the need for investment that would allow increased access to more complex levels of healthcare1-2. Given this picture, from the perspective of increasing the provision of specialist dental services and assuring the totality of dental healthcare, the National Oral Health Policy gave priority to the implementation of Specialty Dental Centers as an alternative for the organization of Secondary Oral Healthcare2,8. The Specialty Dental Centers are considered to be one of the fronts of activity of Brasil Sorridente, being a reference for the Family Health Strategy's dental health teams. These should provide the public with a minimum level of care under the specialties of periodontology, endodontology, patients with special needs, oral diagnosis and minor oral surgery. By virtue of their physical and structural resources, they may be classified into three categories: Type I Specialty Dental Centers, equipped with 3 dental consulting rooms; Type II Specialty Dental Centers, equipped with between 4 and 6 consulting rooms; and Type III Specialty Dental Centers with 7 or more consulting roooms8.
In the Brazilian state of Ceará, the State Oral Health Policy for the period from 2007 to 2010 proposed the construction of 16 regional Specialty Dental Centers, which would be characterized by their greater complexity (Type III Specialty Dental Centers with 11 dental consulting rooms) and by providing the population with a greater number of specialties, such as orthodontics, prosthetics and x-rays. Unlike the municipal Specialty Dental Centers which only treat patients referred by the same municipality, the regional Specialty Dental Centers would come under the management of public health partnerships and would care for patients referred by the city where the service is based and by the other municipalities within the partnership, thereby obtaining greater gains in scale and a better technical, management and financial capacity to provide these services9.
In spite of the fact that Brasil Sorridente recognizes the secondary oral healthcare services as priority as part of the implementation of the National Health Service (SUS), little research has been performed on these services2,10-11. Findings from other countries, however, with their more structured and consolidated oral healthcare models, already show evidence of the concern with studying them12-14.
Given the above, the aim of this study was to describe the implementation of secondary oral healthcare services in the state of Ceará, as well as to analyze the impacts of these services on the provision of specialist dental procedures for the population of this state.
METHODS
This is a descriptive, epidemiological study based on secondary data, using a quantitative approach, structured in two stages: the first stage covers the Situational Diagnosis information on Specialty Dental Centers carried out by the Department of Health for the state of Ceará in February 2011; the second stage used data, based on historical series, of the production of specialist dental procedures carried out by these services, as recorded in the National Health Service's Outpatient Information System (SIA/SUS) in the period from 2000 to 2010.
Data was collected directly from the Department of Health for the state of Ceará by researching the number of Specialty Dental Centers in operation, type of administration (municipal or public partnership), category and year of implementation. Data relating to the outpatient information produced by these services, in the period from 2000 to 2010, were obtained directly from the National Health Service's Outpatient Information System (SIA/SUS).
As the criterion for inclusion in the study, all Specialty Dental Centers implemented through 2010 were included, that had a production of at least 3 months available in the database of the National Health Service's Information Technology Department (DATASUS).
The data were obtained and tabulated using the software application Tab for Windows - TABWIN (Ministry of Health, Brazil) and were exported to Microsoft Excel 2010 (Microsoft Corp., USA), where consolidation and grouping of the data was performed in accordance with the dental procedure subgroups to be evaluated and presented by way of Figures, Tables and descriptive means.
In compliance with National Health Council Resolution 196/96, the research project was sent to the Ethics in Research Committee at the Federal University of Ceará (COMEPE/UFC), and was submitted for subsequent approval under COMEPE case reference no. 222/08.
RESULTS
The study showed that there was a significant growth in the number of municipal Specialty Dental Centers as a result of the National Oral Health Policy, implemented in 2004, while following the implementation of the Oral Health Policy of the state of Ceará, an increase was noted in the number of regional Specialty Dental Centers managed by public health partnerships (Figure 1).
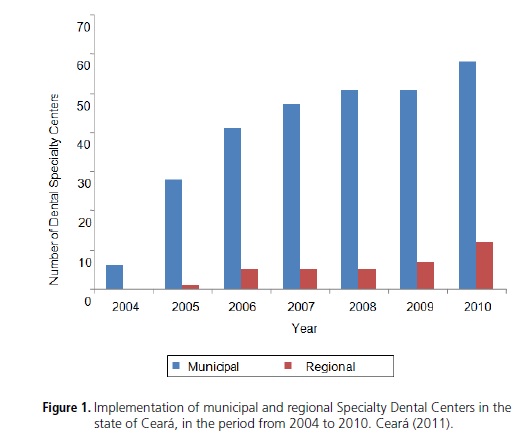
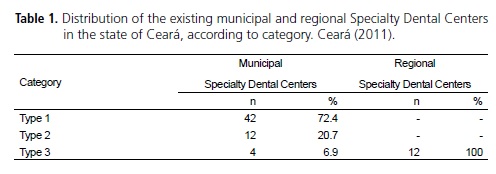
The Specialty Dental Center situational diagnosis conducted by the Oral Healthcare Unit (NUASB) of the Department of Health in the state of Ceará, demonstrated that, through December 2010, 70 Specialty Dental Centers had been implemented in the state. Of these, 58 are municipal, only receiving patients referred by the municipality itself, their activities being financed by federal and municipal funding, and 12 are regional, receiving patients referred by the municipality where the service is based and the other municipalities in the partnership, their activities being financed through federal and state funding, and also from each municipality. As for the category, all the regional Specialty Dental Centers are type III (12/12), while 60% (42/58) of the municipal Specialty Dental Centers are type I, 20.7% (12/58) type II and 6.9% (4/58) type III (Table 1).
By noting the historical series of specialist dental procedures in Ceará, recorded in the SUS Outpatient Information System (SIA/SUS), a considerable increase was found in the number of these procedures after 2004, evidence of the positive impact of the implementation of national and state dental health policy. It can also be seen that the increase in the productivity of these services coincided with the implementation of the regional Specialty Dental Centers, evidence of the important role played by these services in the provision of specialist dental procedures in this state, seeing that the number of these procedures trebled after the increase in the number of these services, which took place after 2008 (Figure 2).

In Table 2, with is described the ratio between specialist and basic dental procedures increased over the course of the last decade, seeing that in 2000 this ratio was 0.04 specialist procedures for every basic procedure while by 2010 the ratio had risen to 0.1. We can also see that the volume of specialist dental procedures in Ceará per inhabitant per year grew significantly, going from 0.03 procedures per inhabitant per year to 0.21.

DISCUSSION
The implementation of Brasil Sorridente has had positive repercussions on the expansion of secondary oral healthcare services and consequently on the availability of specialist dental procedures across the country as a whole15-16.
In the state of Ceará, there was a considerable increase in the number of Specialty Dental Centers, however the vast majority of these are type I and come under municipal administration, being characterized by a reduced number of dental consulting rooms, by a lower monthly productivity and for only treating patients referred by the same municipality in which they were established. In the whole state, during the period studied, twelve regional Specialty Dental Centers were implemented in the municipalities that were the base for health micro-regions, however as this state is divided into 22 micro-regions and only twelve of them were included in this service, the number of Specialty Dental Centers is still insufficient to assure the totality of oral healthcare for the state's entire population17.
The results of this study suggest that the municipal Specialty Dental Centers that were mostly implemented in small municipalities in the state hinterland, have less technical and financial capacity to carry out the tasks for which they are equipped, resulting in low service performance10,18. Table 2. Volume of basic and specialist dental procedures carried out in the state of Ceará, ratio between number of specialist and basic procedures and between number of specialist procedures and the population. Ceará (2011). Year 2000 2004 2010 Population of the state of Ceará 7,430,661 7,998,849 8,180,087 Basic Dental Procedures 7,070,362 10,299,557 17,127,928 Specialist Dental Procedures 272,493 502,009 1,747,474 Ratio between specialist and basic procedures 0.04 0.05 0.10 Ratio between specialist procedures and the population 0.03 0.06 0.21 DB ARAÚJO et al.
According to a descriptive study conducted in Pernambuco relating to the existing secondary oral healthcare services in this state, it was noted that the lower the municipality, the lower its Human Development Index (HDI), and the worse the performance of the Specialty Dental Centers, evidencing the importance of the implementation of regional centers of reference in order to carry out secondary oral health care10. Following this line of thinking, the state of Ceará organized its specialty services network in a regional, decentralized format by means of the formation of public health partnerships as an alternative for making these services viable in small municipalities in the state hinterland and growing the coverage of specialty treatment for the populations in these municipalities9,17-18.
The growth in the number of Specialty Dental Centers in Ceará and consequently the growth in the number of dental specialty procedures recorded in this state's SUS Outpatient Information System, have had the effect of increasing the ratio between dental specialty procedures per inhabitant per year in Ceará, which suggests a growth in the supply of these services to the population. However, this ratio may still be regarded as low by virtue of the epidemiological profile of the population in Ceará as there is a large repressed demand and the epidemiological profile of this population is evidence of the great need for specialty treatment, which could adversely affect the establishment of adequate systems of reference and counter-reference in oral health1,10,19-20.
As an alternative to be used to turn this situation around, authors such as Neves & Ribeiro21 and Nicoletto et al.22 suggest an increase in State Government investment destined for the implementation of the regional Specialty Dental Centers, complying with the agreed Regionalization Master Plan, stimulating the creation of inter-municipal health partnerships to carry out the regionalization of secondary oral healthcare, thereby enabling greater gains in scale and better technical and financial capacity with the provision of these services9.
CONCLUSION
Given the above, an expansion was observed in oral health services in the secondary care system in the state of Ceará, which has made possible a larger supply of specialty dental procedures for the population of the state. However, the capacity to solve the issues with these services is still considered to be a challenge for the administrators and professionals in the area of oral healthcare, as the poor performance of these services could compromise the establishment of a system of reference and counter-reference in oral health, having negative consequences for the doctrinarian principles of the National Health Service such as the universality of services, equitability and totality of healthcare.
Another factor which will help to increase the supply of specialty dental services is the maintenance of dental health policy and the expansion in funding for these services. It is recommended that the State Oral Health Policy is revived, the aim of which was to implement a regional Specialty Dental Center in every health micro-region in the state, thereby considerably growing the supply and access of the population of Ceará to these services.
Lastly, due to the exploratory nature of this study, it was not possible to analyze in greater depth the use of specialist dental procedures made available by the Specialist Dental Centers implemented in Ceará for the state's population. It is recommended that new studies are carried out that are capable of evaluating if there are restrictions on access to these services, if the productivity targets are being met and if the system of reference and counter-reference is well defined.
Collaborators
DB ARAÚJO was responsible for the idea and for all stages of the research and production of the article. LMB MENEZES directed the research and participated in the composition of the article. DL SOUSA actively participated in the composition of the article.
REFERENCES
1. Pucca Jr GA, Costa JF, Chagas LD, Silvestre RM. Oral health policies in Brazil. Braz Oral Res. 2009;23(Suppl 1):9-16. [ Links ]
2. Pucca Jr GA. A política nacional de saúde bucal como demanda social. Ciênc Saúde Colet. 2006;11(1):243-6.
3. Brasil. Ministério da Saúde. Projeto SB Brasil 2003: condições de saúde bucal da população brasileira 2002-2003. Resultados principais. Brasília: Ministério da Saúde; 2004.
4. Baldani MH, Almeida ES, Antunes JLF. Equidade e provisão de serviços públicos odontológicos no estado do Paraná. Rev Saúde Pública. 2009;43(3):446-54 .
5. Pinheiro RS, Torres TZG. Uso de serviços odontológicos entre os Estados do Brasil. Ciênc Saúde Colet. 2006;11(4):999- 1010.
6. Pereira CRS, Patrício AAR, Araújo FAC, Lucena EES, Lima KC, Roncalli AG. Impacto da Estratégia Saúde da Família com equipe de saúde bucal sobre a utilização de serviços odontológicos. Cad Saúde Pública. 2009;25(5):985-96.
7. Brasil. Ministério da Saúde. DATASUS: Sistema de Informação Ambulatorial (SIA/SUS). Brasília (DF) [citado 2010 Fev 28]. Disponível em: <http://www.datasus.gov.br>.
8. Brasil. Ministério da Saúde. Desenvolvimento de Sistemas e Serviços de Saúde. Coordenação Nacional de Saúde Bucal. A Política Nacional de Saúde Bucal do Brasil: registro de uma conquista histórica. Brasília: Ministério da Saúde; 2004.
9. Ceará (Estado). Secretaria de Saúde do Estado. Consórcios Públicos em Saúde no Ceará. Estrtégia para o fortalecimento da regionalização da saúde. Fortaleza: Secretaria de Saúde do Estado do Ceará; 2009.
10. Figueiredo N, Goes PSA. Construção da atenção secundária em saúde bucal: um estudo sobre os Centros de Especialidades Odontológicas em Pernambuco, Brasil. Cad Saude Publica. 2009;25(2):259-67.
11. Volpato LER, Scatena JH. Análise da política de saúde bucal do município de Cuiabá, Estado de Mato Grosso, Brasil, a partir do banco de dados do Sistema de Informações Ambulatoriais do Sistema Único de Saúde (SIA-SUS). Epidemiol Serv Saúde. 2006;15(2):47-55.
12. Morris AJ, Burke FJT. Primary and secondary dental care: how ideal is the interface? Br Dent J. 2001;191(12):666-70.
13. Cheshire PD. Why undertake outreach into general dental practice? Br Dent J. 2002;192:371-4.
14. Morris S, Sutton M, Gravelle H. Inequity and inequality in the use of health care in England: an empirical investigation. Soc Sci Med. 2005;60(6):1251-66.
15. Lima ACS, Cabral ED, Vasconcelos MMVB. Satisfação dos usuários assistidos nos Centros de Especialidades Odontológicas do Município do Recife, Pernambuco, Brasil. Cad Saúde Pública. 2010;26(5):991-1002.
16. Pinheiro RS, Aguiar FP, Sass PE, Vilela MJN. Diferença no uso de serviços odontológicos entre os Estados do Brasil: uma análise baseada em modelos hierárquicos. Cad Saúde Colet. 2006;14(1):141-8.
17. Ceará (Estado). Secretaria de Saúde do Estado. Plano Estadual de Saúde 2007 - 2010. Fortaleza: Secretaria de Saúde do Estado do Ceará; 2008.
18. Beltrammi DGM. Descentralização: o desafio da regionalização para Estados e Municípios. Rev Admin Saúde. 2008;10(41):159-63.
19. Leal RB, Tomita NE. Assistência odontológica e universalização: percepção de gestores municipais. Ciênc Saúde Coletiva. 2006;11(1):155-60.
20. Silva MCB, Silva RCA, Ribeiro CCC, Cruz MCFN. Perfil da assistência odontológica pública para a infância e adolescência em São Luís (MA). Ciênc Saúde Coletiva. 2007;12(5):1237-46.
21. Neves LA, Ribeiro JM. Consórcios de saúde: estudo de caso exitoso. Cad Saúde Pública. 2006; 22(10):2207-17.
22. Nicoletto SCS, Cordoni JrL, Costa NR. Consórcios Intermunicipais de Saúde: o caso do Paraná, Brasil. Cad Saúde Pública. 2005;21(1):29-38.
 Correspondence to:
Correspondence to:
DB ARAÚJO
e-mail: denisbzr@yahoo.com.br
Received on: 17/06/2010
Final version resubmitted on: 27/12/2010
Approved on: 14/2/2011
