










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
ORIGINAL / ORIGINAL
Odontogenic lesions of the jaw: a clinical-pathological study of 461 cases
Lesões odontogênicas dos maxilares: estudo clinico-patológico de 461 casos
Leandro Bezerra BORGES I; Francisco Vagnaldo FECHINE II; Mário Rogério Lima MOTA I; Fabrício Bitu SOUSA I; Ana Paula Negreiros Nunes ALVES I
I Universidade Federal do Ceará, Faculdade de Farmácia, Odontologia e Enfermagem, Curso de Odontologia. Rua Alexandre Baraúna, 949, Rodolfo Teófilo, 60430-160, Fortaleza, CE, Brasil
II Universidade Federal do Ceará, Departamento de Fisiologia e Farmacologia. Fortaleza, CE, Brasil
ABSTRACT
Objective
To establish the epidemiological profile, according to the variables of sex, age group and location of cysts and odontogenic tumors, in the state of Ceará.
Methods
A survey was performed of cases of odontogenic lesions diagnosed and recorded between 1994 and 2009 in the Biopsy Service of the Department of Pathology and Forensic Medicine at the Federal University of Ceará. A total of 48 procedures (24.12%) were grafts using particulate bone while sinus lift grafts were performed on 28 patients (14.07%). Osteogenesis distraction and inferior alveolar nerve lateralization were performed in five (2.51%) and three (1.51%) procedures respectively. Eleven autogenous bone grafts were lost, of which 90.9% were onlay block.
Results
We obtained a total of 461 odontogenic cystic and tumor lesions. Among the cysts, the periapical cyst was the predominant lesion with 196 cases, which predominantly occurs between the age of 21 and 30 years (n=60) and in females (n=120). Ameloblastoma was the most common tumor (n=47) and was most frequently observed between 21 and 30 years of age (n=15) and in females (n=35).
Conclusion
Case series of epidemiological profile of cysts and tumors, contribute to the understanding of the etiological and clinical aspects of these lesions and they also help to confirm correct diagnosis and appropriate treatment.
Indexing terms: Epidemiology. Odontogenic cysts. Odontogenic tumors.
RESUMO
Objetivo
Contribuir para o estabelecimento do perfil epidemiológico, segundo as variáveis de sexo, localização e faixa etária, de cistos e tumores odontogênicos no estado do Ceará.
Métodos
Foi realizado um levantamento dos casos de lesões odontogênicas diagnosticados e registrados de 1994 a 2009 no Serviço de Biópsia do Departamento de Patologia e Medicina Legal da Universidade Federal do Ceará.
Resultados
Obteve-se um total de 461 lesões odontogênicas, císticas e tumorais. Dentre os cistos, o radicular foi a lesão mais prevalente com 196 casos, ocorrendo, predominantemente, na faixa etária de 21 a 30 anos (n=60) e no sexo feminino (n = 120). O ameloblastoma foi o tumor de maior ocorrência (n=47), sendo mais observado entre 21 a 30 anos (n=15) e no sexo feminino (n=35).
Conclusão
Séries de perfil epidemiológico de cistos e tumores odontogênicos contribuem para o entendimento dos aspetos clínicos e etiopatológicos destas lesões corroborando para um correto diagnóstico e um tratamento adequado.
Termos de indexação: Epidemiologia. Cistos odontogênicos. Tumores odontogênicos.
INTRODUCTION
The mouth and the maxillofacial complex are made up of structures that are the target of a wide variety of odontogenic lesions that vary in location, etiology and histogenesis, attacking soft tissue and bone, as well as presenting variable clinical manifestations1.
Amongst the neoplasms of the oral cavity, odontogenic tumors constitute a heterogeneous group of lesions with histopathological characteristics and diverse clinical manifestations2. In a retrospective study by the Oral Pathology Reference Institute at the University of Chile, they represented around 1.29% of tumor lesions of the oral cavity, 99% of which were benign and only 1% malignant3. They affect people in all age groups, being most significant between the second and fifth decade of life and in the female sex. Generally speaking, the lower jaw is the place they most often occur2,4. In a case series of biopsies studied in Washington and at the Biopsy Service at Oregon University Dental School, 19.4% of tumors and 16.6% of cysts were found to be of odontogenic origin. In other analyses within the same study, these lesions represented 17.2% in Canada and 14.9% in Singapore5.
Ameloblastoma is the most quoted odontogenic tumor in several case series in the literature, equating to approximately 10% to 30%6. It is most common in individuals between the second and fifth decades of life, though there is some disagreement amongst authors as to the gender most affected2-4. A greater preference for the lower jaw3,4,6 has been found. Apart from ameloblastoma, other tumors of odontogenic origin are worthy of mention, such as the keratocystic odontogenic tumor, odontoma, odontogenic myxoma2,4. The keratocystic odontogenic tumor, owing to its peculiar clinical-pathological characteristics, was recently reclassified by the World Health Organization (WHO) as a neoplasm of odontogenic origin7. It occurs predominantly as an asymptomatic lesion, between the second and fourth decades of life, in the posterior mandibular region, causing extensive areas of bone reabsorption prior to being diagnosed8. Odontomas constitute one of the odontogenic tumors that occur most frequently in the upper jawbones, being most common in the upper jaw and in patients in the first two decades of life, the average age being 149. The compound type is usually found in the anterior region of the upper jaw; complex odontomas, on the other hand, occur most frequently in the molar region, in both bones of the upper jaw9. Myxomas constitute rare, benign neoplasms and make up around 3% to 9% of odontogenic tumors, occurring in the lower jaw, between the second and fourth decades of life, peaking in the third decade, and are reported to occur most frequently in women, the proportion being 2:110.
Odontogenic cysts represent one of the main causes of upper jaw destruction, found frequently in dental practices and potentially in outpatient clinics engaging in head and neck surgery11. They are classified according to their etiopathogenesis, in progressive or inflamed cysts5,12. According to records in oral histopathological diagnostic services in Mexico City, around 52.5% present in men, 47% in women while in 0.5% of cases, the sex was not identified12. These lesions occur most frequently in people in their second and third decades of life, the average age being 36.5 years, with the upper jaw being the most affected in a ratio of 1.5:15,11.
In an epidemiological analysis using archives from the histopathology laboratory at the Xochimilco Autonomous Metropolitan University in Mexico, the most frequently found progressive cysts were dentigerous, followed by lateral periodontal, eruption, adult gingival, glandular cysts, calcifying epithelial and new-born baby gingival12. These are usually asymptomatic, nevertheless some have the potential to become extremely large and cause expansion of the cortex and erosion11.
In the group of inflamed cysts, periapical and residual are the ones most frequently encountered. The periapical cyst presents a prevalence of 60% of cysts in the upper and lower jaws and is formed on the apexes of teeth with necrotic pulp resulting from the proliferation of epithelial rests of Malassez present in the periodontal ligament or in an existing dental granuloma13-14. In 60% of cases, they occur with the female sex and have a preference for adults between the third and sixth decades of life and for regions of the upper jaw12-13. Residual cysts develop in 57.9% of the male sex, most of which occur between the fourth and sixth decades of life. This fact is often due to its discovery taking place in routine x-rays since, as its name suggests, the cyst is formed out of the epithelial rests left after an erroneous enucleation of the periapical cyst5.
In absolute numbers, after the periapical cyst, the next most prevalent is the dentigerous cyst15. Together, these two entities add up to 73% of all odontogenic cysts12. The dentigerous cyst engulfs the crown of an unerupted tooth, connecting to its cervical region11. In cases diagnosed between 1990 and 2001 in the Surgical Pathology Laboratory in the School of Dentistry at the Federal University of Minas Gerais, 102 dentigerous cysts were found in men, corresponding to 53.7%, a ratio of 1.15:1, the second age group was the period of life most affected, the average being 15.3 years of age; and 133 of the cases (76.4%) occurred in the lower jaw16.
The aim of the present study was to carry out a transversal, observational study, using historical data, of odontogenic tumors and cysts totaling 461 lesions according to the following variables: anatomic site, age and sex, from oral biopsies conducted over a period of 16 years (1994-2009), in the Biopsy Service of the Department of Pathology and Forensic Medicine (DPML) at the Federal University of Ceará.
METHODS
Survey of patient records
A survey was carried out of the histopathological reports from records of patients with lesions in the stomatognathic system, cared for in the disciplines of Stomatology, Oral Dental and Maxillofacial Surgery, Periodontics, Pediatric Dentistry and Endodontics in the Dentistry course at the Faculty of Pharmacy, Dentistry and Nursing and also the discipline of Head and Neck Surgery in the Faculty of Medicine, as catalogued by the Biopsy Service of the Department of Pathology and Forensic Medicine (DPML), all of which are located at the Federal University of Ceará (UFC), during the period from 1994 to 2009.
Epidemiological data collection
Data concerning the clinical aspects, sex, age, anatomic site and histopathological diagnosis of the lesions were taken from the record cards of patient biopsies. Subsequently, these lesions were grouped according to the direction of the World Health Organization and separately studied as to the most frequent location, sex and age range. During the survey, it was noted that a number of patient records did not contain details of the place where the lesion occurred nor the age of the patient. Other records contained inadequate descriptions as to the site of the affliction, thus making it impossible to distinguish between upper jaw and lower jaw. In these cases, therefore, where there were no records or the records carried insufficient description, these were grouped as Not Identified (NI). Lesions of odontogenic origin were divided into benign or malignant cysts and tumors. The inclusion of the odontogenic keratocyst as an odontogenic tumor was considered based on a review of all the histological slides. The entity orthokeratinized odontogenic keratocyst was considered for the rare cases in which the morphological characteristics presented a fine, uniform epithelial layer with an orthokeratinized surface, a prominent subjacent granular area and cuboidal or squamous basal layer cells.
Statistical analysis
Turning to the qualitative variables, the descriptive statistics consequently included the definition of absolute and relative frequencies. The chi-squared test was used to verify the association between variables, as well as the differences between proportions. The level of significance was set at 5%, so a value of p less than 0.05 was considered to be statistically significant. The statistical procedures were carried out with the use of the software application GraphPad Prism® version 5.00 for Windows® (GraphPad Software, San Diego, California, USA, 2007). The project was submitted to the Ethics in Research Committee at the Hospital Complex of the Federal University of Ceará (COMEPE), which regulates research on humans, and approved under reference no. 280/05.
RESULTS
A total of 4,319 lesions from the most diverse origins was obtained in the Biopsy Service of the DPML (UFC) over a period of sixteen years (1994 - 2009), of which 461 were odontogenic in nature, comprising 131 tumors and 330 cysts. Amongst the benign tumor lesions, ameloblastoma presented the highest number of cases at 47, while ameloblastic fibroma presented 4 cases and cementoma 1 case, constituting the 5 cases that represented rarely occurring lesions. Amongst the cystic lesions, 196 cases of periapical cyst were diagnosed and just 2 cases of glandular odontogenic cyst (Table 1).
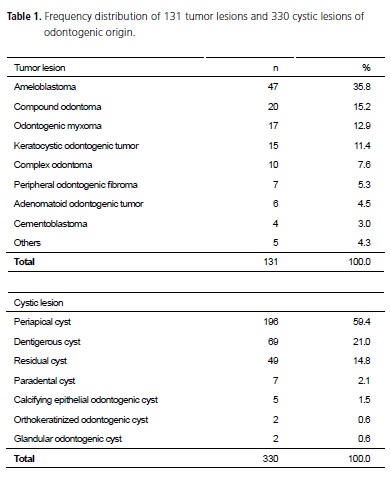
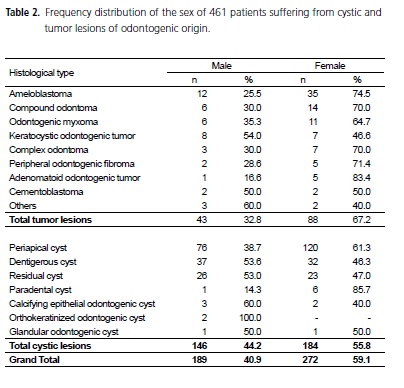
Odontogenic tumors and cysts are more common in the female sex with 88 and 184 cases, respectively. In the odontogenic tumor lesion group, most notably ameloblastoma affected the female sex, with 35 cases. Odontogenic cystic lesions presented the periapical cyst also as being more prevalent in the female sex, amounting to 120 cases. Amongst the other forms of lesion, 3 cases of ameloblastic fibroma were found in the male sex while in the female sex, 1 case of cementoma and also 1 case of ameloblastic fibroma were found (Table 2).
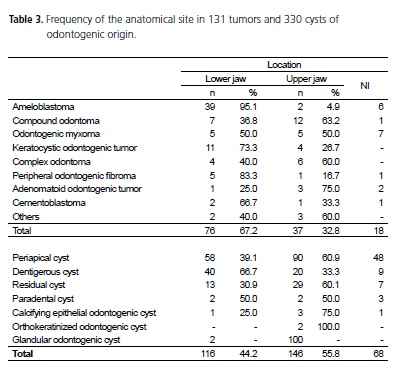
As for location, odontogenic tumors favored the lower jaw in a ratio of 2.05:1. This site presented 2 cases of ameloblastic fibroma, while the upper jaw also exhibited 2 cases of ameloblastic fibroma and another of cementoma. On the other hand, the odontogenic cysts showed the upper jaw to be the site most affected in a ratio of 1.25:1. Only the dentigerous cyst and the glandular odontogenic cyst affected the lower jaw more (Table 3).
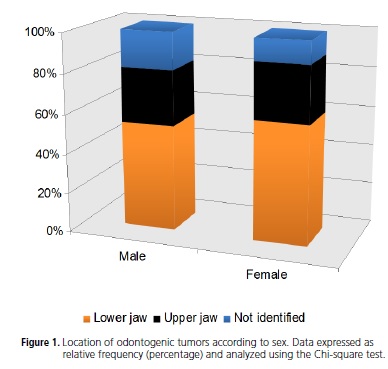
When linking the information on sex and location of odontogenic tumors, it was found that there was no significant difference between the female and male sexes in terms of tumor location (i.e. upper jaw or lower jaw) (Chi-square test = 0.3294; p= 0.8482) (Figure 1).
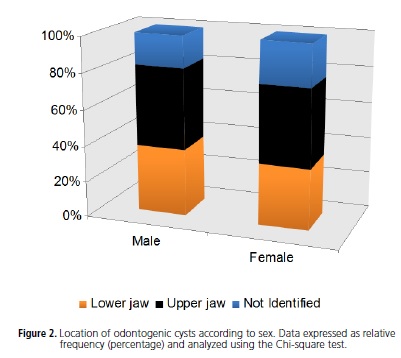
Following the same line of reasoning for the odontogenic cysts, again no statistically significant difference was found between the female and male sexes in terms of cyst location (i.e. upper jaw or lower jaw) (Chi-square = 2.1014; p = 0.3497). Not identified = NI (Figure 2).
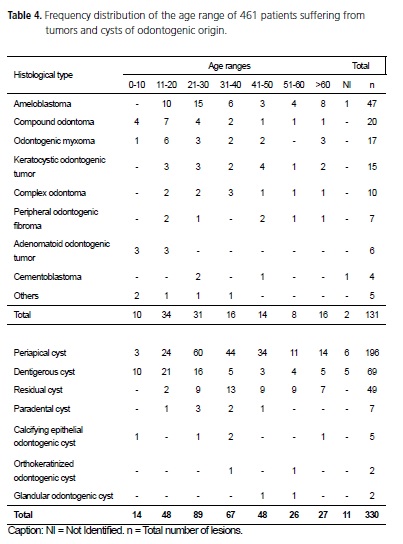
Patients with odontogenic tumors belonged to all age ranges established in this study, though the peak was between 11 and 20 years of age. Ameloblastic fibroma was diagnosed at the ages of 2, 6, 14 and 28 and cementoma in just one patient aged 33. Periapical and residual cysts predominantly occurred in two age groups: 21 to 30 and 31 to 40, respectively, while dentigerous cysts appeared most frequently in patients aged between 11 and 20 years of age. Rare cystic lesions, such as orthokeratinized odontogenic cysts and glandular odontogenic cysts demonstrated no particular preference in terms of age range (Table 4).
DISCUSSION
The incidence and epidemiological behavior of odontogenic lesions experience geographical variations in different regions of the world4. Various scientific studies have evaluated case series according to the variables anatomic site, age range and sex of patients with odontogenic tumors and cysts in one country or in one region1,2,4-5,11,16-18. These lesions occur infrequently in gnathic bones and represent around 2.5% of all lesions biopsied in the dental services2. In a study of 362 cases in Chile, the frequency was 1.29%2. Cystic lesions occur more frequently than tumor lesions as demonstrated by Camisasca et al.1, where out of a total of 131 cases, 89 were cysts and 42 were tumors of odontogenic origin. These data corroborate the results found in our study in terms of the higher frequency of cystic lesions.
As far as the anatomic site is concerned, the lower jaw was the preferred location for odontogenic neoplasms in this survey, consistent with Santos et al.4 and Ochsenius et al.5. As for cystic lesions, these were more prevalent in the upper jaw, also as described in the literature5,17. However, a study by Avelar et al.15 showed the lower jaw to be the site most affected by cystic lesions. As for age range, the incidence of odontogenic neoplasms peaked between the ages of 11 and 20, while cysts occurred in the next age range, between 21 and 30 years of age. These data are consistent with many other surveys2,4-5,17, although the work conducted by Santos et al.11 and Bento et al.19 showed that cysts of an odontogenic nature are common between the ages of 11 and 20. This variance is possibly due to the number of residual cysts that are diagnosed late as a result of the absence of symptoms, being discovered in routine x-rays20. When we compare affliction according to sex, odontogenic tumors present, in our results, a noticeable preference for the female sex, the ratio being 2.04:1. This finding is also borne out by other published case series, however in a greater proportion, varying between 1.33 and 1.76:14-5. In cystic lesions, there was also a greater preference for the female sex, with a lower ratio of 1.26:1, corroborating the results of Bento et al.19 but diverging from other authors inasmuch as incidence in the male sex was more substantive5,11-12,17.
Amongst lesions of a neoplastic nature, ameloblastoma had the highest incidence, this finding being corroborated by Avelar et al.2, Ochsenius et al.3 and Martins et al.6, though it diverged from the findings of other authors where the most prevalent odontogenic tumor was odontoma1,4,9. It was found that, in our State in Brazil, certain services adopt an incorrect stance in which the diagnosis of compound odontoma only takes place in the trans-surgical phase through a visual examination of the teeth, not requiring an histopathological examination to be performed. Therefore they are included in the non-catalogued cases. Martins Neto et al.13, however, showed the keratocystic odontogenic tumor to be the most prevalent neoplasm, a fact not confirmed in this survey, as this was the third most frequently occurring entity. Odontogenic tumors such as peripheral odontogenic fibroma, odontogenic myxoma, adenomatoid odontogenic tumor and cementoma make up the least recurrent group in our results, just as with Avelar et al.2 and Santos et al.4.
The periapical cyst was the most common amongst cystic lesions, a fact that is in agreement with several studies described in the literature1,12,19-21. The periapical cyst is a common entity in dental clinics and its principal etiology is dental caries14. This disease is still the major oral health problem for Brazil and presents a prevalence classified as "very high" in ages and age ranges - indices adopted by the WHO22. The epidemiological picture in Brazil as a whole reflects the continuing sociocultural, economic and political inequality. Allied to this, the difficulty of getting access to public health services in Brazil helps to make the levels of dental caries in the population high and prevalent23. When the carious lesion reaches the pulp and subsequently promotes necrotic pulp, the dissemination and establishment of bacteria or their toxins appear in the periapex or in the para-apical region, which stimulates and activates defense mechanisms permitting vascular and cellular events to give rise to the development of periapical cysts14.
In addition to this entity, the dentigerous cyst constitutes the second most common cystic lesion in our study, findings that are in agreement with Bento et al.19. Some cases of orthokeratinized odontogenic cysts were renamed, according to the new WHO classification7, as keratocystic odontogenic tumors, which exacerbated the grouping and distribution of these two lesions in our results. The calcifying epithelial odontogenic cyst and the glandular odontogenic cyst were the least common lesions found, similar to Santos et al.11 and Taylor et al.12 .
Epidemiological studies should provide reliable, trustworthy data concerning the regions of origin so that they may contribute to the development of health programs and direct care towards the correct target public. However, the geographical variance of a particular disease should be taken into consideration since the search for health services still occurs inequitably between the sexes and age groups. For cultural reasons, men, particularly young men, supposedly seek health services less than others, which results in some diseases appearing to affect the female sex more. Therefore, the participation of the whole population should be encouraged to seek health services when required and to have routine examinations so that early diagnosis can be obtained and consequently get actual data that characterize more faithfully the population of an area or a country.
CONCLUSION
Odontogenic lesions present a peculiar aspect as they occur exclusively in the upper jawbones. Those of neoplastic nature, mainly represented by ameloblastomas, show a preference for the lower jaw in women, while the most frequently occurring cystic lesion was the periapical cyst which prefers the upper jaw in women. Odontogenic tumors have a preference for individuals in the 11 to 20 age range, while cysts were more prevalent in the 21 to 30 age range. Therefore, the understanding, by dental surgeons, of the variances in the epidemiological and clinicalpathological findings, constitutes a basic requirement for the performance of a correct diagnosis and proper treatment.
ACKNOWLEDGMENTS
To the National Council for Scientific and Technological Development (CNPq) for their encouragement and financial support that made this study possible.
Collaborators
LB BORGES, MRL MOTA and FB SOUSA took part in the research, organization and composition of the article. FV FECHINE was responsible for the statistical analysis and composition of the article. APNN ALVES directed the research and participated in the composition of the article.
REFERENCES
1. Camisasca DR, Janini MER, Silva Júnior JA, Bernardo V. Cistos e tumores odontogênicos: estudo epidemiológico. Rev Assoc Paul Cir Dent. 2005;59(4):261-6. [ Links ]
2. Avelar RL, Antunes AA, Santos TS, Andrade ESS, Dourado E. Tumores odontogênicos: estudo clinico-patológico de 238 casos. Rev Bras Otorrinolaringol. 2008;74(5):668-73.
3. Ochsenius G, Ortega A, Godoy L, Penãfiel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases. J Oral Pathol Med. 2002;31(7):415-20.
4. Santos JN, Pinto LP, Figueredo CRLV, Souza LB. Tumores odontogênicos: análise de 127 casos. Pesqui Odontol Bras. 2001;15(4):308-13.
5. Ochsenius G, Escobar E, Godoy L, Peñafiel C. Odontogenic cysts: analysis of 2.944 cases in Chile. Med Oral Patol Oral Cir Bucal. 2007;12(2):E85-91.
6. Martins MD, Rosa Júnior OA, Martins MAT, Bussadori SK, Fernandes KPS. Ameloblastoma: revisão de literatura. ConScientiae Saúde. 2007;6(2):269-78.
7. Phipsen HPP. Tumores odontogênicos. In: Barnes L, Eveson JW, Reichart P, Sidransay D. Genética e patologia dos tumores de cabeça e de pescoço. São Paulo: Ed. Santos; 2009. pp. 283-328.
8. Alva PG, Tanaka A, Oku Y, Yoshizawa D, Itoh S, Sakashita H, et al. Keratocystic odontogenic tumor: a retrospective study of 183 cases. J Oral Sci. 2008;50(2):205-12.
9. Nóia CF, Oliveira FAC, Pinto JMV, Santos WHM. Odontoma composto. RGO - Rev Gaúcha Odontol. 2008;54(2):213-7.
10. Nonaka CFW, Cavalcante RB, Piva MR, Souza LB, Pinto LP. Mixoma odontogênico: estudo clínico-patológico de 14 casos. Cienc Odontol Bras. 2007;10(2):61-7.
11. Santos TS, Antunes AA, Avelar RL, Antunes AP. Cistos odontogênicos: estudo epidemiológico de 72 casos. Rev Bras Cir Cabeça Pescoço. 2007;36(1):30-2.
12. Taylor AM, Camacho MEI, Franco MAD, Tejero MAT. Quistes odontogénicos: análisis de 865 casos. Mecina Oral. 2002;7(2):89-96.
13. Martins Neto M, Danesi CC, Unfer DT. Contribuição ao estudo do cisto radicular revisão de literatura. Saúde. 2004;30(1- 2):90-9.
14. Santos LCS, Ramos EAG, Meira TM, Figueiredo CRLV, Santos JN. Etiopatogenia do cisto radicular. Rev Ciênc Méd Biol. 2006;5(1):69-74.
15. Avelar RL, Antunes AA, Carvalho RWF, Bezerra PGC, Neto PJO, Andrade ESS. Odontogenic cysts: a clinicopathological study of 507 cases. J Oral Sci. 2009;51(4):581-6.
16. Fernandes AM, Souza AF, Mesquita RA, Carmo MAV, Aguiar MCF. Análise das características clínico-histopatológicas do cisto dentígero: estudo retrospectivo de 10 anos. Cienc Odontol Bras. 2006;9(2):56-60.
17. Souza ME, Torres MA, Duarte AHS, Sobral APV. Lesões periapicais: estudo epidemiológico. Rev Bras Patol Oral. 2003;2(1):30-4.
18. Saddy MS, Chilvarque I, Dib LL, Sandoval RL. Aspectos clínicos, radiográficos e terapêuticos do ameloblastoma. RPG Rev Pós Grad. 2005;12(4):460-5.
19. Bento PM, Souza LB, Pinto LP. Estudo epidemiológico dos cistos odontogênicos: análise de 446 casos. Rev Odonto Cienc. 1996;11(22):125-42.
20. Neville BW, Damm DD, Allen CM, Bouquot JE. Doenças da polpa e do periápice. In: Neville BW, Damm DD, Allen CM, Bouquot JE. Patologia oral e maxillofacial. 2ª ed. Rio de Janeiro: Guanabara Koogan; 2004. p. 116.
21. Nanami R, Sampaio C, Olivete J, Pizzatto E, Moresca R, Giovanini AF. Prevalência de cistos maxilares diagnosticados em um centro de referência brasileiro. RSBO. 2009;6(2):143- 6.
22. Peres MAA, Narvai PC, Calvo MCM. Prevalência de cárie dentária em crianças aos doze anos de idade, em localidades do Estado de São Paulo, Brasil, período 1990-1995. Rev Saúde Pública. 1997;31(6):594-600.
23. Baldani MH, Narvai PC, Antunes JLF. Cárie dentária e condições sócio-econômicas no Estado do Paraná, Brasil, 1996. Cad Saúde Pública. 2002;18(3):755-63.
 Correspondence to:
Correspondence to:
LB BORGES
e-mail: le0borges@hotmail.com
Received on: 28/6/2010
Final version resubmitted on: 23/11/2010
Approved on: 11/1/2011
