










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.1 Porto Alegre Jan./Mar. 2012
CLÍNICO / CLINICAL
Cavity instrumentation with chemical vapor deposition diamondcoated bur
Instrumentação cavitária com uso de ponta diamantada obtida pela tecnologia da Deposição Química por Vapor
Flávia Pardo Salata NAHSAN I; Luciana Mendonça da SILVA II; Eduardo Bastista FRANCO I; Paula Costa Pinheiro SAMPAIO I; Luciana Fávaro FRANCISCONI I; Polliana Mendes Candia SCAFFA I; Rafael Francisco Lia MONDELLI I
I Universidade de São Paulo, Faculdade de Odontologia, Departamento de Dentística, Endodontia e Materiais Odontológicos. Al. Dr. Octávio Pinheiro Brisolla, 9-75, 17012-901, Bauru, SP, Brasil
II Universidade Federal do Amazonas, Faculdade de Odontologia. Manaus, AM, Brasil
ABSTRACT
High- and low-speed rotary dental handpieces have been used for a long time in restorative dentistry for cavity preparation. However, problems inherent to conventional burs, such as noise, heat and vibration, have led to the development of new dental burs, such as the chemical vapor deposition diamond-coated bur. Its advantages are many, such as less noise, less pain for the patient, precise cutting, conservative cavity preparation, longer lifetime, less injury to the dental structures, no cutting of soft tissues and easier access of the carious lesion. This case report uses a chemical vapor deposition diamond-coated bur to prepare a cavity by direct proximal access, preserving the marginal ridge. The cavity was then filled with glass ionomer cement. The clinical outcome was satisfactory. Direct access to the cavity was possible because of the chemical vapor deposition diamond-coated bur, resulting in comfort for the patient and dentist.Indexing terms: Dental caries. Dental cavity preparation. Glass ionomer cements.
RESUMO
Os instrumentos rotatórios convencionais têm sido utilizados em alta e/ou baixa velocidade há tempos para a confecção de cavidades na odontologia restauradora. Contudo, problemas inerentes a estes equipamentos, como o ruído, calor e vibração mecânica levaram ao desenvolvimento de novos instrumentos, como a ponta de diamante pela tecnologia Deposição Química por Vapor. Esta apresenta uma série de vantagens como menor ruído, procedimento menos doloroso, desgaste preciso e preparo conservador, maior durabilidade da ponta, menor injúria à estrutura dentária, não corta os tecidos moles e acesso facilitado à lesão cariosa. Este trabalho apresenta um relato de caso clínico demonstrando o uso da ponta de diamante Deposição Química por Vapor para a confecção de um preparo cavitário proximal com acesso direto, com preservação da crista marginal, restauração com cimento de ionômero de vidro. O resultado clínico satisfatório foi conseguido, com acesso direto à cavidade em detrimento à configuração das pontas utilizadas, proporcionando conforto para o paciente e cirurgião dentista.Termos de indexação: Carie dentária. Preparo da cavidade dentária. Cimentos de ionômeros de vidro.
INTRODUCTION
High- and low-speed rotary handpieces with conventional burs are commonly used for cavity preparation. However, conventional burs generate heat, mechanical oscillations and noise, have a short lifetime, often remove too much healthy dental tissue and may injure the pulpal tissue if refrigeration is inadequate1-2.
A new technology has recently introduced a new bur in the market, the chemical vapor deposition (CVD) diamond-coated bur. Its objective is to overcome the limitations of conventional burs in cavity preparation.
CVD diamond-coated burs are made by decomposing the gases hydrogen and methane on the surface of a heated molybdenum shank in a vacuum reactor, producing a synthetic diamond coating of uniform thickness2-3. The mechanical oscillations, that is, vibrations, promoted by ultrasound waves reduce friction and wear and enhance heat evacuation4. CVD diamond-coated burs are less noisy, usually do not require local anesthesia, do not cut soft tissues, exempts the use of hand-cutting instruments to finish the cavity, have a much longer lifetime and wear the dental structures uniformly, precisely and conservatively, three objectives of restorative dentistry1,3,5-7.
The aim of this study was to demonstrate the use of a CVD diamond-coated bur in vivo for the preparation of a proximal cavity by direct access.
CASE REPORT
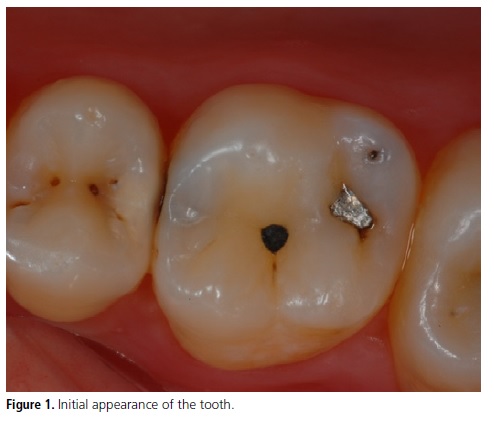
A 23-year-old female patient presented at the Graduate Dentistry Clinic of University of São Paulo Bauru School of Dentistry for dental treatment. The patient complained of pain and difficulty flossing the mesial surface of the first right upper molar (Figure 1). After getting the patient's history and performing a clinical and radiographic examination, a treatment plan for removing the carious lesion (Figure 2) was established. A CVD diamond-coated bur would be used to create and plane the cavity walls.
Pumice and water prophylaxis was followed by complete isolation of the area by a rubber dam. Since a carious lesion was also present on the proximodistal surface of the adjacent premolar, it was removed to allow direct access to the lesion of the first right upper molar, dispensing the need of preparing a vertical or horizontal slot, preserving the marginal ridge.
The CVD diamond-coated bur was attached to an ultrasonic handpiece (Cvdent 1000, CVDentus) and used for the initial access (Figure 3). This system uses mechanical oscillations that promote a uniform and conservative wear on the tooth, and is more silent than the conventional bur1,3,8. Moreover, the bur is cooled by a water stream (Figure 4), avoiding excessive heat and consequent pulpal damage3.
Initial access to the lesion was done by a spherical CVD diamond-coated bur (CVDentus, São José dos Campos, Brazil). The entire carious lesion was then removed by sharp curettes, followed by the CVD diamond-coated bur again to finishing cavity preparation (Figure 4).
A conditioner was applied to the surfaces of the cavity. Light-cured glass ionomer cement (Vitremer, 3M ESPE, St. Paul, MN, USA) was applied for 30 seconds and cured with a halogen light (Optilux-Demetron, Kerr) for 20 seconds (Figure 5). This material was selected because the patient is at high risk of caries. Its formula contains fluoride which benefits the tooth by reacting with the mineral hydroxyapatite from the enamel during the remineralization process, making the tooth more resistant to acid9-10.
The glass ionomer cement was prepared and applied according to the manufacturer's instructions and applied to the cavity with a Centrix tip (Centrix Inc., Shelton, CT, USA). Once the cavity was filled, a polyester matrix band was laid on the glass ionomer cement and light-cured for 40 seconds.
This stage was followed by the initial finish, glazing (Vitremer, 3M ESPE, St. Paul, MN, USA) and light-curing for another 20 seconds. The distal-occlusal restoration of the premolar was finished with amalgam. After seven days, the final polishing of the restoration was done with sandpaper strips and polishing paste (Figure 6).





DISCUSSION
Traditionally, cavities have been prepared with conventional burs, which are made by galvanic bonding of diamond grains on a stainless steel shank. This method of bonding the diamond grains allows the grains and bonding metal (nickel in the form of Ni2+) to detach, along with other components that may contaminate the dental structure1,11-12.
In the CVD diamond-coated system, diamond settles on a metal shank, forming a uniform coating2. More precisely, these burs are made in a vacuum reactor that mixes methane and hydrogen to form a single layer of synthetic diamond characterized by the absence of space between the diamond grains and molybdenum substrate2-3,12. Its roughness is small and standardized and it does not release nickel (II) ions in the oral fluids5.
Conventional diamond burs lose cutting efficiency after each sterilization cycle and use, and need to be replaced constantly12. CVD diamond-coated burs have a longer lifespan and more resistance to the sterilization process2,11. The ultrasound handpiece must be used as instructed by the manufacturer, adjusted according to the CVD diamond-coated bur used. Exceeding the recommended power for a given bur can wear the tip of the diamond coating, destroying the bur.
The use of CVD diamond-coated burs for cavity preparation requires training because it differs from that of conventional burs. This system uses mechanical oscillations, not rotary movement. The dental structure is worn by the lateral face of the CVD diamond-coated bur. The pressure applied on the ultrasonic tip must be mild, only enough to guide the instrument, otherwise the cutting efficiency is reduced, causing pain, noise and heat1,13.
Minimally invasive cavity preparations are one of the main objectives of dental surgery and consists of using instruments to remove as little of the dental structure as possible1,6-7. Ultrasonic CVD diamond-coated burs allow the precise removal of diseased dental tissue, resulting in a minimally invasive cavity preparation, conserving most of the dental structure2,11.
Another reason CVD diamond-coated burs stand out is because of their various inclination angles, allowing direct access to the lesion without damaging the adjacent tooth14. This is often not possible with conventional rotary instruments, making the removal of healthy tooth tissue sometimes necessary.
In the present clinical case, the patient did not experience pain during cavity preparation with the ultrasonic CVD diamond-coated bur. Likewise, in two clinical situations where the cavities were prepared with ultrasonic CVD diamond-coated burs in the distal surface of element 11 and occlusal surface of element 26, the patients did not experience pain1. Other literature reports that used these same burs in pediatric patients also reported that no pain was felt by the patients14-17.
In the future, there will be more emphasis on the improvement of burs by the CVD diamondcoating technology. Studies investigating the long-term effectiveness of this technology are inexistent at this time. It is also important to point out that the marketing of new materials requires caution and more studies.
CONCLUSION
This case report has shown that the use of a CVD diamond-coated bur resulted in a conservative and strictly proximal cavity, easily instrumented thanks to bur angles. The clinical outcome was satisfactory, with greater comfort for the patient and dentist.
Collaborators
FPS NAHSAN, LM SILVA, LF FRANCISCONI, PMC SCAFFA and PCP SAMPAIO helped to treat the patient, took pictures, and wrote and reviewed the article. EB FRANCO and RFL MONDELLI supervised the clinical case and helped to write and review the article.
REFERENCES
1. Carvalho CAR, Fagundes TC, Barata TJE, Trava-Airoldi VJ, Navarro MFL. The Use of CVD diamond burs for ultraconservative cavity preparations: a report of two cases. J Esthet Restor Dent. 2007;19(1):19-29. [ Links ]
2. Valera MC, Ribeiro JF, Airoldi VT, Corat EJ, Peña AFV, Leite NF. Pontas de diamantes - CVD. RGO - Rev Gaúcha Odontol. 1996;44(2):104-8.
3. Predebon JC, Flório FM, Basting RT. Use os CVDentUS diamond tips for ultrasound in cavity preparation. J Cont Dent Pract. 2006;7(3):1-9.
4. Diniz MB, Rodrigues JA, Chinelati MA, Cordeiro RAL. Microinfitração marginal em cavidades preparadas com pontas CVDentus® e diamantadas convencionais. Cienc Odontol Bras. 2005;8(1):75-81.
5. Trava-Airoldi VJ, Corat EJ, Moro JR. Studies of CVD diamond applications as ultrasound abrading devices in odontology and related uses. Rev Bras Apl Vacuo. 2006;25(2):71-4.
6. Peters MC, McLean ME. Minimally invasive operative care. I. Minimal intervention and concepts for minimally invasive cavity preparations. J Adhes Dent. 2001;3(1):7-16.
7. Mount GJ, Ngo H. Minimal intervention: early lesions. Quintessence Int. 2000;31(8):525.
8. Trava-Airoldi VJ, Corat Ej, Ferreira NG, Leite NF. CVD-Diamond: an overview of research and development at INPE. Braz J Phys. 1997;27(4):88-92.
9. Featherstone JDB. The continuum of dental caries: evidence for a dynamic disease process. J Dent Res Res. 2004;83(Spec Iss C):C39-C42.
10. Ingram GS, Agalamanyi EA, Higham SM. Caries and fluoride processes. J Dent. 2005;33(3):187-91.
11. Lima, LM, Motisuki C, Santos-Pinto LS, Santos-Pinto AS, Corat EJ. Cutting characteristics of dental diamond burs made with CVD technology. Braz Oral Res. 2006;20(2):155-61.
12. Borges CFM, Magne P, Pfender E, Heberlein J. Dental diamond burs made with a new technology. J Prosthet Dent. 1999;82(1):73-9.
13. Lima LM, Diniz MB, Galassi MAS, Ramalho LTO, Dos Santos- Pinto L. Evaluation of the dentin-pulp complex after cavity preparation with ultrasonic diamond tip. Minerva Stomatol. 2011;60(1-2):15-23.
14. Cardoso MV, Coutinho E, Ermis RB, Pointevin A, Landuyt KV, Munk JD, et al. Influence of dentin cavity surface finishing on micro-tensile Bond strength of adhesives. Dent Mater. 2008;24(4):492-501.
15. Antonio AG, Primo LG, Maia LC. Case report: ultrasonic cavity preparation: an alternative approach for caries removal in paediatric dentistry. Eur J Paediatr Dent. 2005;6(2):105-8.
16. Oliveira J, Dorado L, Koch D, Scur A, Barbosa A. Marginal microleakage in cavities prepared with CVD tip and 245 bur. Dent Implantol Update. 2009;20(3):17-23.
17. Sá PP, Valente AGLR, Pomarico L. Utilização da técnica da abrasão ultrassônica em odontopediatria. Rev Bras Odontol. 2010;67(2):174-7.
 Correspondence to:
Correspondence to:
JCV RIBEIRO
e-mail: jcarlosvr@gmail.com
Received on: 24/9/2008
Approved on: 5/2/2012
