










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre Abr./Jun. 2012
ORIGINAL / ORIGINAL
Fabrication of plaster models with radiographic features of human bone: a pilot study by fractal analysis
Confecção de modelos de gesso com características radiográficas compatíveis com osso humano: estudo piloto por meio da análise fractal
Guilherme D'Agostino Romanini de FREITAS I; Marcelo Lupion POLETI I; Cláudio Roberto Gaião XAVIER I; Ana Cláudia de ARAÚJO I; Ana Lúcia Alvares CAPELOZZA I
I Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Estomatologia. Al. Doutor Octávio Pinheiro Brisolla, 9-75, 17012- 901, Bauru, SP, Brasil
ABSTRACT
Objective
This study attempted to fabricate plaster models that reproduce the radiographic characteristics of human bone.
Methods
A section of an edentulous dry mandible was radiographed and molded. The inside of the templates was lined with dental wax and filled with gypsum plaster mixed with sawdust or rice flour in proportions of 25%, 33.3% and 50% to simulate the trabecular pattern. Once this mixture settled, the wax lining was removed and the space filled with stone plaster to simulate the cortical bone. Three plaster models were fabricated for each proportion of each material. The models were radiographed and the radiographs that best resembled that of human bone were selected, one for each proportion of each material. The chosen radiographs were digitalized, and the digital images were Gaussian-blurred, binarized, skeletonized and submitted to fractal analysis.
Results
All binary (p=0.000) and most skeletonized (p=0.000) images of the two groups were significantly different from that of the human mandible section, except for the skeletonized image of the model containing 50% rice.
Conclusion
Although the results of this study did not allow consistent conclusions, they showed that the methodology is appropriate and practical for other similar studies. More studies are needed using different proportions of the same materials and bigger sample sizes for more reliable assessments of different mixtures.
Indexing terms: Bone density. Calcium sulfate. Dental radiography.
RESUMO
Objetivo
Desenvolver modelos de gesso que possam reproduzir radiograficamente osso humano.
Métodos
Uma secção de mandíbula edêntula foi radiografada e moldada. O molde obtido recebeu um alívio no interior com cera 7. Para vazá-lo utilizou-se gesso pedra misturado à serragem ou a arroz triturado nas proporções de 25; 33,3 e 50% para simular osso medular. Após o tempo de presa, a cera foi retirada e vazou-se nesse espaço gesso pedra para simular osso cortical. Foram obtidos três modelos em cada proporção estabelecida para os dois materiais. Estes modelos foram radiografados e a imagem mais semelhante à arquitetura óssea da mandíbula foi selecionada. As radiografias foram digitalizadas e as análises radiográficas realizadas por meio das imagens binária e esqueletonizada aplicando-se o protocolo de processamento Gaussian-Binary-Skeletonize.
Resultados
Quando comparados com a mandíbula, todos os grupos apresentaram diferença estatisticamente significativa tanto para as imagens binárias (p= 0,000) quanto esqueletonizadas (p= 0,000), com exceção do Grupo Arroz 50% (A50) para imagem esqueletonizada.
Conclusão
Embora os resultados deste estudo, não tenham permitido conclusões mais consistentes, eles serviram para determinar uma metodologia que se mostra prática e adequada para aplicação em estudos da mesma natureza. Porém, existe a necessidade de testar diferentes proporções dos materiais adicionados ao gesso pedra e aumentar o número das amostras para se obter uma avaliação mais fidedigna destes materiais.
Termos de indexação: Densidade óssea. Sulfato de cálcio. Radiografia dentária.
INTRODUCTION
Imaging phantoms are used for standardizing the reproduction of a given feature. In radiology, phantoms are frequently used for producing images resembling the oral structures, such as bones or soft tissues, or for standardizing variations, such as different tissue widths1-3.
Phantoms are very important because they allow study standardization, avoiding undesirable influences on the results. Ethically, they comply with the principles of biosafety since individuals are not exposed to the ionizing radiations associated with radiographs for study purposes, except when the methodology specifically requires clinical radiographs. Phantoms allow not only a better control of the study variables but also easier execution and repetition of the study stages without biological hazards1-3.
Different methods and phantoms are used in radiographic studies, such as: metal blocks1, usually made of aluminum for comparing perceived contrast; acrylic2 or wax3 blocks for simulating facial soft tissues; and supports, such as dry mandibles or fabricated models for the fixation and subsequent radiographing of teeth, with plaster being the most common material used for this purpose4-6. Nevertheless, these materials should be used judiciously since they may change the appearance of a radiograph and, consequently, its interpretation and study results. Therefore, phantom radiographic features and anatomic shapes should reproduce facial tissues faithfully.
Published studies on phantom fabrication techniques using materials and/or protocols capable of producing radiographic images resembling human bone were not found. Hence, fabrication protocols of phantoms with materials that reproduce the radiographic features of human bone faithfully are needed, both for educational and research functions.
METHODS
A section of an edentulous mandible was molded with addition silicone (Optosil, Heraeus Kulze, Germany). The molds were then lined with wax 7 (Polidental, Cotia, Brazil) to preserve the space corresponding to the cortical bone. Next, the molds were filled with a mixture of gypsum plaster (Vigodent, Rio de Janeiro, Brazil), prepared as recommended by the manufacturer, mixed with different proportions of sawdust or rice flour to simulate the medullary cavity. The experimental groups were: Group S25: 75% plaster mixed with 25% sawdust by volume; Group S33: 66.7% plaster mixed with 33.3% sawdust by volume; Group S50: 50% sawdust and plaster by volume; Group R25: 75% plaster mixed with 25% rice flour by volume; Group R33: 66.7% plaster mixed with 33.3% rice flour by volume; Group R50: 50% rice flour and plaster by volume.
After setting, the models were taken out of the molds, the wax layer removed and the models placed back inside. The empty space was filled with gypsum plaster, prepared according to the manufacturer's instructions, to simulate cortical bone. Three plaster models were fabricated for each experimental group.
The mandibular section and respective models were placed on an acrylic support for the standardization of the radiographs. The support had a 1.5 centimeter wall to simulate the soft tissues of the mouth.
Ektaspeed Plus (Kodak, Manaus, Brazil) films were used within their shelf lives with the radiograph unit Yoshida (Yoshida Dental MFC Co. Ltd., Tokyo, Japan), operating at 70 kVp and 7 mA, and exposure time of 0.4 seconds. The films were manually processed using the standard temperaturetime method and fresh chemicals. All films were developed in a single stage. One radiograph was taken of each plaster model and three of the mandibular section.
The radiographs received paper frames and three radiologists were asked to choose the one that best resembled human mandibular bone (control group). Seven radiographs were selected, one for each experimental group and one for the control group.
These radiographies were photographed in manual mode by the digital camera Nikon model Coolpix 8700 (Nikon Inc., New York, USA), using an exposure time of 1/15 seconds, aperture of f/5.0 and an ISO of 100. The photographs were saved in jpeg format with a resolution of 600dpi.
The polarized-light negatoscope Medalight LP-400 (Medalight, São Paulo, Brazil) was taken to a dark room and covered with a black ethylene-vinyl acetate (EVA) sheet (IBEL, Maracanaú, Brazil) containing a large enough window to hold one radiograph at a time and block the remainder light. The abovementioned camera was mounted on a copy stand (Nikon Repro-Copy Outfit PF-2, Nikon Inc., New York, USA) and the photographs were taken at a distance of 15 centimeters.
The digital photographs were transferred to a computer and converted to grayscale images (8 bits per sampled pixel allowing 256 different intensities) by the software ImageJ (National Institutes of Health, Bethesda, USA). Using this same software, an area of 118x118 pixels was selected from three different regions of interest of each image: left, center and right. Each area selection was cut and processed for better assessment of its features, so three different areas of each image was assessed.
The images were Gaussian-blurred, binarized and skeletonized (GBS) for fractal analysis7,13. The Gaussian blur filter was applied to a circular area with a diameter of 35 pixels. This filter removes all the fine- and medium-scale structure, preserving only the large grayscale variations. The blurred image was subtracted from the original image and the number 128 was added to each pixel of the resulting image. Hence, the resulting image showed the specific variations of the bone trabeculae and medullary cavities. After this procedure, the images were converted to binary images, that is, all pixels became either black or white, corresponding to the bone trabeculae and medullary cavities, respectively.
The contour was submitted to fractal analysis, and the box-counting method attributed a value to the contour and scale measurements.
The binary image was then "opened." In other words, a layer of one pixel is removed from the contours of the black areas and a layer of one pixel is added to these areas. This procedure preserves the features of the image but removes undesired small regions or pixels. Next, the images were skeletonized. Skeletonization consists of removing the pixels in the areas of interest of a binary image until only a one-pixel wide line equidistant from the object borders is left. The resulting skeleton was also submitted to fractal analysis of contour (Figure 1).
The results were submitted to two-way analysis of variance (two-way ANOVA) followed by the Tukey test, which assessed how the added substance and respective proportions affected the image in comparison with the control group (mandible). The significance level was set at 5%. The statistical tests were done by the software Statistica 6.0 (Statistica for Windows 6.0 Copyright StatSoft, Inc. Tulsa, Okla, EUA).
The study was approved by the Research Ethics Committee of the University of São Paulo School of Dentistry of Bauru (Process no 99/2004), according to resolution 196/96 of the National Council of Health.
RESULTS
Three regions of interest of each of the seven chosen images were assessed, totaling 21 regions. The means and standard deviations of the binary and skeletonized images of each group were calculated.
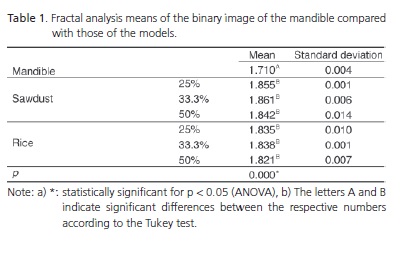
Table 1 shows the comparison between the binary image of the mandible and those of the models, according to two-way ANOVA.
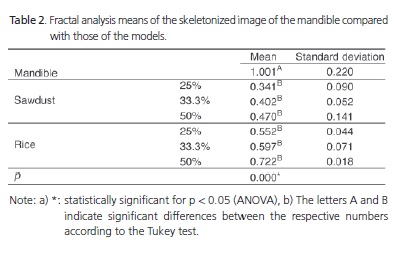
Table 2 shows the comparison between the skeletonized image of the mandible and those of the models, according to two-way ANOVA.

DISCUSSION
Fractal analysis is used for describing complex shapes and structures and measured by fractal dimension. It is considered a good indicator of morphological changes or differences in human bone6-13. In dentistry, fractal analysis has been used in periodontics6-7 and endodontics8. It has also been used to study systemic diseases, such as osteoporosis9-12 and sickle-cell anemia13. These studies also mention the possibility of using fractal analysis for the characterization of bone trabecular pattern.
Studies have used different kinds of radiograph digitalization and image processing methods. Many authors prefer the Gaussian blurring-binarization-skeletonization protocol and obtain encouraging results7,13. This study chose this method because of its ease of use and ample use in similar studies, facilitating future comparisons.
Fractal analysis of the binary image of the mandible and that of the models are compared in Table 1. The control and experimental groups differed significantly in all comparisons, regardless of mixture composition, showing that either the image processing protocol, or the proportions of rice and sawdust used, or both, did not result in radiographic images that effectively resembled human bone.
Table 2 compares the fractal analysis data of the skeletonized image of the mandible with that of the plaster models. The skeletonized image of the mandible differed from nearly all those of the models, except for those of Group R50. Hence, this group was the only one that resulted in images radiographically similar to those of human bone.
A consistent conclusion was not possible because of the abovementioned methodological limitations, but there is evidence that a mixture of gypsum plaster and 50% or more rice may produce images that resemble human bone after Gaussian blurring, binarization and skeletonization.
Since there are no protocols and/or methods in the literature for fabricating materials that reproduce the radiographic features of human bone, the results of the present study are an important contribution to future studies, which may use these results as a guideline. The fabrication of phantoms that resemble human bone has important advantages, such as greater control over the different study variables, easier execution and possibility of repeating the study stages whenever necessary. Another important point is the increasing difficulty of obtaining human tissues for research purposes, which may delay or prevent new studies.
The main limitation of this study is the small number of compositions tested.
CONCLUSION
Although more consistent conclusions are not possible with the present results, this study demonstrates a practical and appropriate methodology for the fabrication and testing of radiographic phantoms. New mixtures of plaster and other materials in different proportions need to be tested to better assess their radiographic behavior.
Collaborators
GDR FREITAS, ML POLETI, CRG XAVIER, AC ARAÚJO and ALA CAPELOZZA participated in all stages of the study, from conception until the final version of the article.
REFERENCES
1. Yoshiura K, Kawazu T, Chikui T, Tatsumi M, Tokumori K, Tanaka T, et al. Assessment of image quality in dental radiography, part 1: phantom validity. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87(1):115-22. doi: 10.1016/S1079- 2104(99)70304-5. [ Links ]
2. Gasparini AL, Lemke F, Carvalho AS, Cunha FL, Junqueira JLC, Tavano O. Verificação das condições do processamento radiográfico em consultórios odontológicos. RGO - Rev Gaúcha Odontol. 2005;53(3):217-9.
3. Moraes LC, Castilho JCM, Dotto GN, Carvalho EC, Araújo BC, Balducci I. Avaliação do comprimento do pino para implante utilizando radiografia digital (técnica do paralelismo). RGO - Rev Gaúcha Odontol. 2004;52(2):79-82.
4. Kang BC, Farman AG, Scarfe WC, Goldsmith LJ. Mechanical defects in dental enamel vs. natural dental caries: observer differentiation using Ektaspeed Plus film. Caries Res. 1996;30(2):156-62.
5. Xavier CRG, Araujo-Pires AC, Poleti ML, Rubira-Bullen IRF, Ferreira Jr O, Capelozza ALA. Evaluation of proximal caries in images resulting from different modes of radiographic digitalization. Dentomaxillofac Radiol. 2011;40(6):338-43
6. Jolley L, Majumdar S, Kapila S. Technical factors in fractal analysis of periapical radiographs. Dentomaxillofac Radiol. 2006;35(6):393-7.
7. Shrout MK, Hildebolt CF, Potter BJ, Comer RW. Comparison of 5 protocols based on their abilities to use data extracted from digitized clinical radiographs to discriminate between patients with gingivitis and periodontitis. J Periodontol. 2000;71(11):1750-5. doi: 10.1902/jop.2000.71.11.1750.
8. Yu YY, Chen H, Lin CH, Chen CM, Oviir T, Chen SK, et al. Fractal dimension analysis of periapical reactive bone in response to root canal treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(2):283-8. doi: 10.1016/j.tripleo.2008.05.047.
9. Jett S, Shrout MK, Mailhot JM, Potter BJ, Borke JL. An evaluation of the origin of trabecular bone patterns using visual and digital image analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(5):598-604. doi: 10.1016/j.tripleo.2004.07.020.
10. Shrout MK, Jett S, Mailhot JM, Potter BJ, Borke JL, Hildebolt CF. Digital image analysis of cadaver mandibular trabecular bone patterns. J Periodontol. 2003;74(9):1342-7. doi:10.1902/ jop.2003.74.9.1342.
11. Ya]ar F, Akgünlü F. Fractal dimension and lacunarity analysis of dental radiographs. Dentomaxillofac Radiol. 2005;34(5):261-7.
12. Tosoni GM, Lurie AG, Cowan AE, Burleson JA. Pixel intensity and fractal analyses: detecting osteoporosis in perimenopausal and postmenopausal women by using digital panoramic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(2):235- 41. doi: 10.1016/j.tripleo.2005.08.020.
13. Demirba AK, Ergün S, Güneri P, Aktener O, Boyacıolu H. Mandibular bone changes in sickle cell anemia: fractal analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(1):e41-8. doi: 10.1016/j.tripleo.2008.03.007.
 Correspondence to:
Correspondence to:
ALA CAPELOZZA
e-mail: anacapel@fob.usp.br
Received on: 15/10/2010
Final version resubmitted on: 19/7/2011
Approved on: 18/11/2011
