










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre Abr./Jun. 2012
ORIGINAL / ORIGINAL
Experience of dental caries in mother/child pairs: association between risk indicators and dental caries
Experiência de cárie dentária em pares de mães e filhos: associação com indicadores de risco para a doença
Márcia Rejane Thomas Canabarro ANDRADE I; Antonio CANABARRO II; Luiz Flavio MOLITERNO I
I Universidade do Estado do Rio de Janeiro, Faculdade de Odontologia. Rua Professor Rodolpho Paulo Rocco, 325, 21941-913l, Rio de Janeiro, RJ, Brasil
II Universidade Veiga de Almeida, Departamento de Ciências da Saúde. Rio de Janeiro, RJ, Brasil
ABSTRACT
Objective
To verify the relationship between the experience of caries in mothers and their children and to identify associations between the child's experience of caries and the socio-demographic and behavioral factors of the families.
Methods
73 mother/child pairs were examined by one calibrated examiner (Kappa = 0.87) using dmft and DMFT (deciduous and permanent dentition, respectively). To collect socio-demographic and behavioral data, a tested questionnaire was used (Kappa = 0.91). The following statistical tests were used: Kappa agreement analysis of the data collection instruments, Kruskal-Wallis and Mann-Whitney tests to compare mean indices, Spearman Correlation to assess the correlation between ordinal variables and Chi-square to assess the association between independent variables and the outcome. Significance level was set at 5%.
Results
100% of mothers and 75.3% of children had at least one tooth with experience of dental caries. There was a statistically significant difference between the mean dmft in relation to age (p <0.01). Among the variables studied, a positive correlation was found between the number of missing teeth of the mother and dmft (p <0.05) in children under eight year-old, and an association between the lack of brushing before bedtime and the outcome for children.
Conclusion
the experience of dental caries in mothers was replicated in their children. Specific programs aimed at changing family behavior and encouraging the consumption of healthy diets may be necessary to control dental caries, especially in children of pre-school age.
Indexing terms: Cross-sectional studies. Dental caries. Epidemiology. Mother-child relations. Risk index.
RESUMO
Objetivo
Verificar a relação entre a experiência de cárie de mães e filhos e identificar associações entre a experiência de cárie do filho com variáveis sócio-demográficas e comportamentais da família.
Métodos
Setenta e três pares mãe-filho foram examinados, por uma examinadora calibrada (Kappa= 0,87), utilizando-se os índices ceo-d e CPO-D (dentições decídua e permanente, respectivamente). Para a coleta dos dados sócio-demográficos e de comportamento foi utilizado questionário testado (Kappa= 0,91). Os testes estatísticos utilizados foram: Kappa para análise de concordância dos instrumentos de coleta, Kruskal- Wallis e Mann-Whitney para comparação das médias dos índices, Correlação de Spearman para avaliação de correlação entre as variáveis ordinais e numéricas e qui-quadrado para avaliar a associação entre as variáveis independentes e o desfecho investigado. Foram considerados significativos valores de p< 0,05.
Resultados
Todas as mães (100%) e 75,3% das crianças apresentavam pelo menos um dente atacado por cárie. Houve diferença estatisticamente significativa entre as médias do índice ceo-d em relação à idade (p< 0,01). Entre as variáveis estudadas, correlação positiva foi encontrada entre o número de dentes perdidos da mãe e o ceo-d (p< 0,05), nas crianças abaixo de oito anos de idade, e associação com a falta de escovação antes de dormir pelas crianças.
Conclusão
A experiência de cárie dentária da mãe mostrou-se reproduzida na experiência de cárie do filho na dentição decídua. Programas orientados para a efetiva mudança de comportamento e o estímulo aos hábitos e dietas saudáveis podem ser necessários para o controle da cárie dentária, especialmente em crianças em idade pré-escolar.
Termos de indexação: Estudos transversais. Cárie dentária. Epidemiologia. Relações mãe-filho. Indicador de risco.
INTRODUCTION
Dental caries is a chronic disease caused by the interaction of multiple factors. Despite the slow progression of lesions in the majority of individuals, they are rarely self-limiting in the absence of treatment. The main contributors to the etiology of dental caries are the cariogenic microorganisms (streptococcus of the group mutans and lactobacillus), fermentable carbohydrates in the diet, susceptibility of the host and time1. The initial bacterial colonization and the transmissibility of the dental caries are important factors in the study of the prevalence of caries in children2. Studies suggest that the mother is the main source of S.mutans infection for her child. There is evidence that children whose mothers have high levels of S.mutans in their saliva have a greater experience of caries than those whose mothers have low saliva levels of these microorganisms2-3.
Despite scientific evidence supporting the association of S.mutans with dental caries, the cause/effect relationship between this bacteria and the disease has been disputed. Therefore, within the current thinking, caries should not be regarded as a classic infection, determined by a specific microorganism, but a complex disease that depends on the interaction of biological, behavioral and socioeconomic factors4-5.
Historically, biological and dietetic influences have merited the greatest attention of researchers, however, given the influence of communitarian, family and individual conditions and of the interrelationship of the causal factors in the outcomes in oral health, studies attempt to identify other indicators associated with the prevalence of caries, suggesting that socio-demographic and behavioral variables may act as risk factors for dental caries or as factors related to this disease6-7. However, there is no consensus that these variables might have predictive power, at the community level, for dental caries8.
Despite the findings of a reduction in the prevalence of dental caries in recent decades9, the disease is still very common in children in Brazil10. Even in developed countries where this reduction has been evident, it has been argued that the factors are probably related to the permanence of high indices of the disease in certain individuals or groups, within a particular region or country11. The possibility of finding out more about them would allow us to "make adaptations to oral health care and redirect the resources spent on prevention", mainly in the poorer countries12.
Based on this evidence, the performance of studies aimed at evaluating the oral health conditions of children and their respective mothers should be encouraged, since to investigate the presence, or not, of a correlation between the experience of dental caries in mother and child, and the relationship between the experience of caries in the child with the socio-demographic and behavioral variables of the family could be fundamental to a better understanding of this multifactorial disease.
Therefore, the aims of this study were to check for the presence, or otherwise, of mother/child dental caries and identify possible associations between the experience of caries in the child with socio-demographic and behavioral variables.
METHODS
For this cross-sectional study (approval CEP 1516 - HUPE/UERJ), we conducted a census of children between the ages of 5 and 12 enrolled in the Pediatric Dental Clinic at the Faculty Of Dentistry at the Rio de Janeiro State University, between January 2000 and December 2005. A total of 530 enrolled children were identified from the register. The record cards of 425 of these children were selected, 105 of them not being located, assumed to have been mislaid. Of the 425 mother/child pairs initially identified, 336 did not respond to the recruitment drive performed by telephone, following two attempts. Of the 89 respondents, 16 were excluded as they did not live with the biological mother or because they presented severe systemic alterations, a syndrome or a physical or emotionally incapacitating condition. The final number of 73 children was considered to be representative, based on the following formula for finite populations:
where ∂ represents the confidence level (95%, 1.96), p.q represents the minimum percentage where the phenomenon occurs (30% of the sample with the disease, based on age-related data from the oral health program known as SB Brasil, 30.30), n represents the population (425) and e represents the sampling error (normally between 3 and 7; 7 was used here). The result was a minimum value of 61 children required, our number being 20% higher.
Clinical examination
The clinical examinations were carried out between November 2006 and June 2007, in a dental consulting room, under artificial light and with a jet of air, with the assistance of a mouth mirror and explorer. The exploratory probe was only used when it was necessary to remove debris in order to confirm the diagnosis. The DMFT and dmft indices of caries attack were applied during the clinical examination in order to evaluate the oral condition of the mother/son pairs13. The condition of the crowns and roots of the permanent teeth were analyzed and for the deciduous teeth just the crown, considering the visual diagnosis of caries in the presence of the lesion cavity. The teeth with fillings with recurring caries were assumed to be decayed and only those teeth lost to caries were recorded. The third molars were not included in the permanent teeth examination. Data from the clinical examinations were noted on a clinical record card. No x-rays were taken for the diagnosis of dental caries.
The examinations were conducted by just one previously calibrated examiner. For the calibration, duplicate clinical exams were performed (DMFT and dmft), in 10 children in the age range defined for the study, with an interval of one week between each. The children examined during the calibration were not included in the study. The Kappa value obtained in the reliability test was 0.87.
Interview
The mothers were interviewed through the application of a questionnaire in order to obtain their socio-demographic and behavioral data and those of their children. The tool was assembled based on the analysis of publications of epidemiological studies. The interview was conducted by the same examiner as on the day of the clinical examination. The evaluation of the reliability of the questionnaire was conducted for 10% of the sample by means of the test and retest method, at an interval of one week between interviews. The agreement calculated via the Kappa statistical test was 0.91.
Statistical analysis
The software application SPSS version 8.0 for Windows was used to analyze the data. Besides the descriptive analysis, calculation of the frequencies, means and standard deviation, the following statistical tests were applied: Kappa test to analyze agreement of the collection instruments employed, Kruskal-Wallis (H) and Mann- Whitney (U) non-parametric tests to compare the means of the indices, Spearman's correlation (rs) to evaluate the correlation between the ordinal and numerical variables and the Chi-square test (2) to evaluate the association between the independent variables and the investigated outcome. Values of p< 0.05 were considered to be significant.
RESULTS
Seventy-three mother/child pairs took part in the study. The high percentage of non-respondents (79%) occurred due to changes in family addresses and telephone numbers (73%), or to not appearing for the clinical examination and interview on the appointed date (27%).
The average age of the children was 8.26 years (±2.09) and the mothers, 34.47 years (±6.45), the youngest mother being 23 and the oldest 48 years old.
The majority were single (71.2%), but lived in a stable relationship with their partners (72.6%). The number of children born per mother was 2.43 (±1.19) on average. In the birth order of the offspring, 46.6% of the children were the first-born, and the average age of the mothers at the date of the birth of the child was 26.09 years (±6.04).
The analysis of the dental condition of the mother/child pairs revealed a high prevalence of caries in the population being studied. One hundred per cent of mothers and 75.3% of the children had at least one tooth attacked by caries, the filled component being the most prevalent (46.8% in the mothers and 65.0% in the children). Just 24.6% of children were caries-free. At the age of seven, 32.0% of teeth had experienced caries.
The mean DMFT of mothers was 14.5 (±5.62), with the component being Decayed 1.75 (±2.13), Lost 5.94 (±5.70) or Filled 6.79 (±4.94).
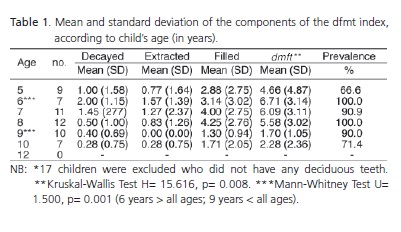
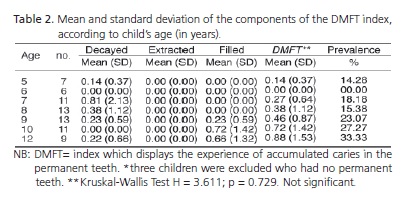
The mean and standard deviation of the number of decayed, lost or filled teeth in the deciduous and permanent dentitions are represented in Tables 1 and 2, respectively. The mean of the dmft index exhibited a significant difference in terms of age (p< 0.05) (Table 1).
At six years of age, it was noted that 100% of children had at least one tooth that had experienced caries in the deciduous dentition, showing the highest mean for the index (dmft= 6.71). The lowest mean for the index was observed at nine years of age (dmft= 1.05). In the permanent dentition, a modest increase was observed with experience of caries, though the DMFT index remained low (Table 2).
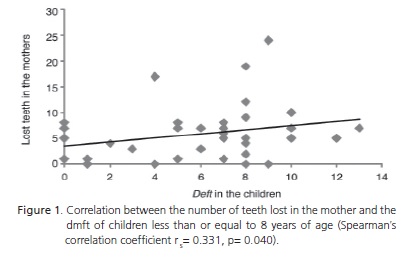
Correlation between experience of caries in mother/child
The link between the experiences of dental caries in the mother/child pairs was observed in children of eight years of age or less. There was a statistically positive correlation between the number of teeth lost in the mother and the number of teeth affected in the deciduous dentition in this age group (Figure 1).
Association between the independent variables and the presence or absence of dental caries
Amongst the socio-demographic factors tested, a statistically significant difference was found between age and the presence or absence of dental caries, when the variable was divided into two age ranges. Children between five and eight years of age, inclusive, presented more caries than those between nine and twelve (p< 0.01).
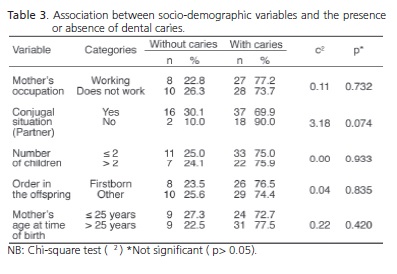
The variables related to mothers, such as occupation, number of children, birth order of the child in the offspring and mother's age at the time the child was born, did not show a significant difference between categories, as far as the investigated outcome was concerned (Table 3).
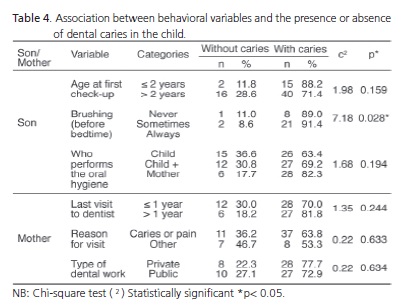
Table 4 shows the association between behavioral variables and the experience of caries by the child. With regard to the children's behavior, all of them used a toothbrush and toothpaste with fluoride to carry out their oral hygiene, therefore this variable was ignored in the association test. Amongst the behavioral variables tested, there was a statistically significant difference between frequency of brushing before sleeping and the presence or absence of caries (p< 0.05), but no association was found with regard to the child performing oral hygiene, without the help or supervision of the mother (Table 4). As for the child's first visit to a dentist, no difference was found in terms of the child's age at the time of the initial dental appointment, despite the fact that 76.7% of them paid their first visit after reaching the age of two (Table 4).
With regard to the behavior of the mothers, among the variables relating to the time elapsed since their last visit to the dentist, reason for appointment and type of dental work received by them, no difference was observed as regards the investigated outcome (Table 4).
DISCUSSION
The results of this study showed a high experience of caries in mothers and children alike. These results reinforce the fact that caries remains a common disease in infancy, although it is clear that its prevalence has diminished in recent decades in several parts of the world. The declining global trend in dental caries, particularly in the developed countries, has been linked to changes in sugar consumption and the standard of caries diagnosis, to better socioeconomic conditions, to access to dental care and especially the widespread use of fluorides9.
When analyzing the high indices of attacks of dental caries in mother/child pairs, it can be seen that the filled component was the most prevalent, which has also been demonstrated in other studies14-15, suggesting that the access of this population to dental care has followed the surgical reconstruction model.
The greater experience of caries in deciduous teeth versus permanent teeth, revealed in this study, may be explained by the greater period of time the deciduous dentition is exposed to the oral environment and due to the age range of children who participated in the study (5 to 12 years of age). This data is compatible with the results obtained in other studies16-17, based on epidemiological surveys conducted in American and Brazilian children, respectively, that established this difference between the deciduous and permanent dentitions in the same age range.
Several studies have shown a link between socioeconomic factors18, behavioral factors19 and the prevalence of dental caries in children. A low prevalence of caries in children was recently associated with families whose mothers have a higher level of schooling20. In the present study, the majority of the variables studied did not show any association with the outcome (dental caries in the children). These results are perhaps due to some limitations of the present study, such as the absence of external validity and limitations inherent to the application of the questionnaires. As an example, we might consider the sample calculation performed by Tagliaferro et al.20 The sample in this study was established assuming a power of 80%, a 5% level of significance and an odds ratio of 2. Almost 500 children were included in the study. Salina et al.18, in a control-case study, used the selfsame parameters and arrived at a total required number of 489 children, divided into three groups for comparison. These numbers are very close to those used by Wigen et al.19 who examined 523 children. Add to this the existence of randomization criteria in the majority of the studies, which obviously also increases their external validity. The present study, therefore, as it possesses a convenience sample of 73 mother/child pairs, does not present a high power of generalization, thus being more prone to a type II error, i.e. accepting that there are no statistical differences when in truth the null hypothesis is invalid. So, it was decided to perform a census of all the children treated over a period of 5 years (2000-2005) and perform a sample calculation based on the finite populated found (425 children). Thus, we arrived at the forecast number of 73 children. In this way, it may be considered that, despite it being a convenience sample, the present study evaluated a sample that was representative of a relatively large and homogeneous group of children, which confers a greater internal validity on the results, i.e. a number was used that was above the minimum required to assure that the experiment is valid for the specific instance to which it was applied. Another important issue was raised by Casanova-Rosado et al.21 These authors highlighted the fact that the application of questionnaires or interviews, directly to the mothers or to those responsible for the collection of information relating to the dietary and oral hygiene habits, can often introduce a degree of bias, since in cross-sectional studies all the data is collected in one session and may not represent a past behavior on account of the influence of the outcome on the response. Moreover, studies are usually designed differently, have different standards of measurement of disease prevalence and severity, as well as different sample sizes, as already mentioned. Nevertheless, there is evidence of a relationship between socioeconomic22-23 and behavioral factors24 and the experience of dental caries in children. In the present study, besides the lack of brushing before bedtime, the number of teeth lost by the mother also presented a significant association with the lower experience of caries in children eight years old or younger. Above this age group, this correlation was not observed, which is perhaps explained by the lower number of teeth attacked in children over eight years old. The correlation between the mother's oral condition and that of the child was also investigated in Canada. As with the present study, the authors found that the children of edentulous mothers had more teeth with experience of caries than those whose mothers had most of their teeth6. It appears, therefore, that specific factors may be connected with this association, such as the eating habits of the edentulous or partially toothed mothers who have difficulty in eating fruit, fiber and vegetables, which could promote the intake of a diet rich in carbohydrates, characterizing a habit that could be replicated in the child6.
Due to the high prevalence of caries found in the mother/child pairs, the implementation of programs of health promotion would seem to be needed that represents a mediatory strategy between the individuals and the environment in which they live, irrespective of the socioeconomic conditions of the mothers and children, in order to diminish inequality of oral care, primarily involving children of pre-school age. For the families studied, the focus of prevention in dentistry that focuses its attention purely on information seems to be inadequate for the prevention of dental caries. Simply addressing the factors relating to family habits and lifestyle, which is the primary source of information for the children25, does not appear to be sufficient to reduce the prevalence of caries. Information to which the population is already privy, such as the importance of brushing before bedtime, should be reinforced, but primarily a transformation of behaviors and attitudes must be encouraged, which includes healthy habits and diets. It is only in this way that Institutions of Higher Education and Pediatric Dentistry services, which treat a public similar to that found in the present study, will be able to work more towards maintaining health rather than the treatment and control of the disease. Offering services of primary and secondary prevention at an individual level, oriented towards (veritable) change in behavior, has now become a professional responsibility for all those that work in the area of oral healthcare26.
CONCLUSION
The experience of dental caries in mothers was found to be replicated in the experience of caries in the child, in the deciduous dentition. Several socioeconomic and behavioral factors were studied. The lack of the habit of brushing teeth before bedtime was shown to be associated with the experience of caries in the children. As mothers with a higher number of missing teeth had children with greater experience of caries, programs directed towards the effective change in behavior and encouragement of healthy habits and diet may be necessary for the control of dental caries, especially in children of pre-school age.
Collaborators
MRTC ANDRADE participated in all stages of the work, from planning the study to the collection and analysis of data and the final editing of the article. A CANABARRO participated in the data analysis and final editing of the article. LF MOLITERNO participated in the planning of the study, data analysis and composition of the article.
REFERENCES
1. van Houte J. Role of micro-organisms in caries etiology. J Dent Res. van Houte J. Role of micro-organisms in caries etiology. J Dent Res. 1994;73(3):672-81. doi: 10.1177/00220345940730031301. [ Links ]
2. Berkowitz RJ, Turner J, Green P. Maternal salivary levels of Streptococcus mutans and primary oral infection of infants. Arch Oral Biol. 1981;26(2):147-9. doi: 10.1016/0003- 9969(81)90086-8.
3. Wan AK, Seow WK, Purdie DM, Bird PS, Walsh LJ, Tudehope DI. A longitudinal study of streptococcus mutans colonization in infants after tooth eruption. J Dent Res. 2003;82(7):504-8. doi: 10.1177/154405910308200703.
4. Beighton D. The complex oral microflora of high-risk individuals and groups and its role in the caries process. Community Dent Oral Epidemiol. 2005;33(4):248-55. doi: 10.1111/j.1600- 0528.2005.00232.x.
5. Fejerskov O. Changing paradigms in concepts on dental caries: consequences for oral health care. Caries Res. 2004;38(3):182- 91. doi: 10.1159/000077753.
6. Bedos C, Brodeur JM, Arpin S, Nicolau B. Dental caries experience: a two-generation study. J Dent Res. 2005;84(10):931-6. doi: 10.1177/154405910508401011.
7. Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA, Soobader MJ, Bramlett MD, et al. Influences on children's oral health: a conceptual model. Pediatrics. 2007;120(3):510-20. doi: 10.1542/peds.2006-3084.
8. Vanobbergen J, Martens L, Lesaffre E, Bogaerts K, Declerck D. The value of a baseline caries risk assessment model in the primary dentition for the prediction of caries incidence in the permanent dentition. Caries Res. 2001;35(6):442-50.
9. Bonecker M, Cleaton-Jones P. Trends in dental caries in Latin American and Caribbean 5-6- and 11-13-year-old children: a systematic review. Community Dent Oral Epidemiol. 2003;31(2):152-7. doi: 10.1034/j.1600-0528.2003.00009.x.
10. Peres MA, Latorre MRO, Sheiham A, Peres KG, Barros FC, Hernandez PG, et al. Social and biological early life influences on severity of dental caries in children aged 6 years. Community Dent Oral Epidemiol. 2005;33(1):53-63. doi: 10.1111/j.1600-0528.2004.00197.x.
11. Maltz M, Barbachan e Silva B. Relationship among caries, gingivitis and fluorosis and socioeconomic status of school children. Rev Saúde Publica. 2001;35(2):170-6. doi: 10.1590/ S0034-89102001000200011.
12. Peres KG, Bastos JR, Latorre MRO. Severity of dental caries in children and relationship with social and behavioral aspects. Rev Saúde Publica. 2000;34(4):402-8. doi: 10.1590/S0034- 89102000000400014.
13. WHO. Basic methods. 4th ed. Geneva: World Health Organization; 1997.
14. Cardoso SV, Pereira SM, Tagliaferro EPS, Pereira AC, Meneghim MC. Condições de saúde bucal na cidade de Campinas: uma avaliação crítica. Arq Odontol. 2004;40(4):341-52.
15. Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988-1994. J Am Dent Assoc. 1998;129(9):1229-38.
16. Gillcrist JA, Brumley DE, Blackford JU. Community socioeconomic status and children's dental health. J Am Dent Assoc. 2001;132(2):216-22. 17. Hoffmann RHS, Cypriano S, Sousa MLR, Wada RS. Experiência de cárie dentária em crianças de escolas públicas e privadas de um município com água fluoretada. Cad Saúde Pública. 2004;20(2):522-8. doi: 10.1590/S0102-311X2004000200020.
18. Salina W, Nizam A, Naing L. The association of birth order and sociodemographic factors with caries experience among adolescents in Tumpat. Arch Orofacial Sci. 2007;2:45-50.
19. Wigen TI, Wang NJ. Caries and background factors in Norwegian and immigrant 5-year-old children. Community Dent Oral Epidemiol. 2010;38(1):19-28. doi: 10.1111/j.1600- 0528.2009.00502.x.
20. Tagliaferro EP, Ambrosano GM, Meneghim MC, Pereira AC. Risk indicators and risk predictors of dental caries in schoolchildren. J Appl Oral Sci. 2008;16(6):408-13. doi: 10.1590/S1678- 77572008000600010.
21. Casanova-Rosado AJ, Medina-Solis CE, Casanova-Rosado JF, Vallejos-Sanchez AA, Maupomé G, Ávila-Burgos L. Dental caries and associated facotrs in Mexican schoolchildren aged 6-13 years. Acta Odontol Scand. 2005;63(4):245-51.
22. Al-Hosani E, Rugg-Gunn A. Combination of low parental educational attainment and high parental income related to high caries experience in pre-school children in Abu Dhabi. Community Dent Oral Epidemiol. 1998;26(1):31-6. doi: 10.1111/j.1600-0528.1998.tb01921.x.
23. Campus G, Lumbau A, Lai S, Solinas G, Castiglia P. Socioeconomic and behavioural factors related to caries in twelveyear- old Sardinian children. Caries Res. 2001;35(6):427-34.
24. Gibson S, Williams S. Dental caries in pre-school children: associations with social class, toothbrushing habit and consumption of sugars and sugar-containing foods. Further analysis of data from the National Diet and Nutrition Survey of children aged 1.5-4.5 years. Caries Res. 1999;33(2):101-13.
25. Petersen PE, Esheng Z. Dental caries and oral health behaviour situation of children, mothers and schoolteachers in Wuhan, People's Republic of China. Int Dent J. 1998;48(3):210-6.
26. Ramseier CA, Catley D, Krigel S, Bagramian RA. Entrevista motivacional. In: Lindhe J, Lang NP, Karring T. Tratado de periodontia clínica e implantodontia oral. Rio de Janeiro: Guanabara Koogan; 2010. p. 669-77.
 Correspondence to:
Correspondence to:
MRTC ANDRADE
e-mail: marciathomas13@gmail.com
Received on: 21/6/2010
Final version resubmitted on: 14/11/2010
Approved on: 20/3/2011
