










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre Abr./Jun. 2012
ORIGINAL / ORIGINAL
Self-perception and oral health conditions of the elderly in a small town
Autopercepção e condições de saúde bucal de idosos em cidade de pequeno porte
Cezar Augusto CASOTTI I; Laís de Andrade LIMA II; Douglas Leonardo GOMES FILHO II; Kléryson Martins Soares FRANCISCO II
I Universidade Estadual do Sudoeste da Bahia, Programa de Pós-graduação em Enfermagem e Saúde. Av. José Moreira Sobrinho, s/n., Jequiezinho, 45206- 190, Jequié, BA, Brasil
II Universidade Estadual do Sudoeste da Bahia, Curso de Odontologia. Jequié, BA, Brasil
ABSTRACT
Objective
To evaluate the oral health status, self-perception, oral condition and access to dental services in elderly aged 65-74 living in the urban municipality of Manoel Vitorino, Bahia.
Methods
This is a cross-sectional epidemiological study. We used the DMFT index, and the use of and need for dental prosthesis, Geriatric Oral Health Assessment Index and a semi-structured questionnaire to assess the oral health status, self-perception of oral condition and access to dental services. Data were collected by a single standardized examiner in home visits with Community Health Workers, and were tabulated and analyzed using the software Epibuco and Epi-info.
Results
We examined 88 subjects, the mean DMFT and age being 28.9 and 68.89, respectively. It was found that 96.7% of teeth were lost, 68.2% were completely edentulous and 63.26% had unsatisfactory prostheses. The value of the Geriatric Oral Health Assessment Index was 27.21. Among the subjects examined, 19.3% had access to public dental services.
Conclusion
From the data obtained, we conclude that the oral health status of elderly residents in the urban area of Manoel Vitorino is unsatisfactory, the self-perception of oral health is low and access to public oral health care is inadequate.
Indexing terms: Aged. Oral health. Perception. Self concept.
RESUMO
Objetivo
Avaliar a condição de saúde bucal, autopercepção da condição oral e o acesso ao serviço odontológico de idosos com idade de 65 a 74 anos residentes na zona urbana do Município de Manoel Vitorino, Bahia.
Métodos
Trata-se de um estudo epidemiológico transversal, utilizando-se dos índices: CPO-D; uso e necessidade de prótese dentária; Geriatric Oral Health Assessment Index e de um questionário semi-estruturado para avaliar a condição bucal, autopercepção da condição oral e acesso aos serviços odontológicos. Os dados foram coletados por um único examinador padronizado, em visita domiciliar com Agentes Comunitários de Saúde, sendo tabulados e analisados nos programas Epibuco e Epi-info.
Resultados
Foram examinados 88 indivíduos, sendo a média do CPO-D e idade respectivamente 28,9 e 68,89. Verificou-se que 96,7% dos dentes estavam perdidos, 68,2% dos indivíduos eram edêntulos totais e 63,26% possuíam próteses insatisfatórias. O valor do índice Geriatric Oral Health Assessment Index foi de 27,21. Dos idosos examinados 19,3% tiveram acesso aos serviços públicos odontológicos.
Conclusão
A condição de saúde bucal dos idosos residentes na zona urbana do município de Manoel Vitorino é insatisfatória, a autopercepção da saúde oral é baixa e o acesso aos serviços públicos de atenção a saúde bucal é inadequado.
Termos de indexação: Idoso. Saúde bucal. Percepção. Auto-imagem.
INTRODUCTION
The absence of health policies in Brazil in times past contributed to the high rate of edentulism1, which has now become a public health issue and is generating a large demand from the population with needs for prosthetic treatment2. Over the years, the life expectancy of the Brazilian population has risen from 67 years in 1991 to 72.57 by 20073, which has prompted fresh studies focusing on the health of the elderly4.
Before health actions can take place, epidemiological surveys are essential to provide support for the development of the planning and organization of the services. The information supplied by these surveys can determine the frequency and distribution of diseases, as well as being low-cost and easy to analyze the data, thereby permitting comparisons in time and space and even evaluating the impact of each risk factor5-6.
By generating various functional problems with speech, mastication, nutrition and systemic geriatric illnesses, edentulism also creates a huge esthetic impact, pain and social frustrations that could result directly in reduced quality of life for the elderly population4,7.
The premature loss of teeth in the elderly may be interrelated with a number of different factors and may even be perceived, incorrectly, as a process arising from the physiological reactions of growing old1. However, recent studies have revealed that the main cause of edentulism is tooth decay, accompanied by periodontal problems and wear and tear caused by chewing4.
The majority of studies which assess changes in the state of oral health of individuals and populations, has been based on clinical indicators of the disease, there being relatively few evaluations of health and wellbeing based on the perception of the individual8. It is enormously important to understand how people perceive their own oral health, since behavior is determined by this self perception, by past experiences with the health services, by cultural values and the importance which is attributed to health. Thus it is understood that, even if a health service were to be offered which is both excellent and free of charge, the population would only seek help if they felt the need for treatment9.
Presuming the low socioeconomic and cultural level to be a determining factor in the difficulty of gaining access to health services, this study was carried out in the municipality of Manoel Vitorino, located in the south-central region of the state of Bahia, which in 2009 boasted an estimated population of 14,138 inhabitants10. The main feature of this municipality is its Human Development Index of 0.59 and illiteracy rate of 25% which, according to the Institute of Sustainable Development for Semi-Arid Regions (IDAN), contribute to widespread poverty in the population known as the "misery triangle" of the mid-section of the Contas River.
Moreover, bearing in mind the paucity of epidemiological studies that address the oral health condition of residents of the smaller municipalities, as well as taking into consideration the increase in the life expectancy of the Brazilian population, the present study seeks to evaluate the state of oral health, access to dental health services and the self-perception of oral health of individuals between the ages of 65 and 74, who are residents of the town and municipality of Manoel Vitorino, in the state of Bahia.
METHODS
This was a cross-sectional, epidemiological study carried out on individuals between the ages of 65 and 74, as advocated by the World Health Organization, registered with the two existing Family Health Centers in the town and municipality of Manoel Vitorino.
The municipality is located 342km (approx. 214 miles) from the state capital of Salvador and, according to information obtained from the department of health, it has a population living in the urban zone of approximately 5,231 inhabitants. There are two Family Health Centers in the town, responsible for servicing 100% of the urban population.
A simple random sample was selected, without replacement of the sampling elements, from all of the residents aged between 65 and 74, born between August 1st 1935 and July 31st 1945, residing in the two adjoining areas and registered with the Family Health Centers.
A total of 265 residents were identified as being in this age range. Of these, 132 were selected, of which 88 were examined. As far as the exclusion criteria are concerned, elderly individuals no longer living in the area were rejected, as were those who did not agree to be studied, those who were deceased or those who were functionally incapacitated. Individuals with non-serious chronic diseases, controlled via medication, were included. The response rate was 66.6%.
In order to locate the subjects of the study, appointments were made for home visits with each of the 12 Community Health Workers responsible for the families living in the town and municipality. The examiner took part in a workshop on the standardization of criteria in caries diagnosis and the use of and need for prosthetic devices (Kappa 95% and 98%).
In order to evaluate the oral health indicators, data were collected on dental caries, the need for dental treatment and the use of and need for dentures. The codes and criteria adopted during the examinations were those recommended by the World Health Organization and the Brazilian Ministry of Health11.
The clinical examination of the oral cavity was carried out with the aid of a flat mirror and a suitably sterilized WHO periodontal probe, in the patient's home and in a location which afforded adequate natural light. The universal biosafety guidelines were adopted for the protection of those individuals studied.
Dentures that met the clinical requirements of stability, adaptation, retention and integrity were classified as functional. A denture was considered not to be functional when at least one of these requirements was not met.
To evaluate self-perception of the elderly in relation to oral health, the Geriatric Oral Health Assessment Index was used. Access to dental services was evaluated by means of a questionnaire including 7 closed questions.
The Geriatric Oral Health Assessment Index comprises 12 questions involving the analysis of information supplied by the individuals themselves with regard to the influence their oral problems had on the physical/functional dimensions (e.g. diet, speech, swallowing), psychosocial/ psychological dimensions (e.g. dissatisfaction with their appearance, self-perception of oral health) and the pain/ discomfort dimension (e.g. mouth pain or the use of medication to relieve these sensations). For each response to these questions, scores were assigned of between 1 and 3 which, when added together, would come to the value of the index, and three of the questions (3, 5 and 7) were calculated with inverse values. The index has a maximum value of 36 and minimum of 12, where the higher the number the better the self-information with regard to oral health9.
The patients were grouped according to the Geriatric Oral Health Assessment Index as follows: "high perception" (34 to 36 points), "moderate perception" (30 to 33 points) and "low perception" (≤ 30 points)9 and the connection with the clinical diagnosis of caries and the use of functional prosthetics was studied by way of the Chisquare test or Fisher's exact test, with a level of significance of 5%.
The data obtained during the exam were copied to an index record card. The clinical variables and those relating to self-perception of oral health, were studied by means of a descriptive analysis using the software applications "Epibuco" (Eymar Souza Lopes) and "Epiinfo" version 3.2.2.
The study was approved by the Research Ethics Committee at the Southwest Bahia State University, filed under record nos. 038/2008 and 077/2009.
RESULTS
After two home visits, it was possible to evaluate the oral health condition of 88 elderly individuals. The average age was 68.89 (sd ±2.88), median age 68.5, mode 65, 1st quartile 66 and 3rd quartile 71.25. Of those elderly individuals examined, 34 (38.6%) were male and 54 (61.4%) were female.
The clinical examination of the oral cavity revealed that the mean of the DMFT index was 28.92 (sd± 5.78), median 32, mode 32, 1st quartile 27 and 3rd quartile 32. Analyzing the DMFT index by sex, the following values were obtained for men: mean 29.21 (sd± 4.43), median 32, mode 32, 1st quartile 27, 3rd quartile 32 and for women: mean 28.74 (sd± 6.52), median 32, mode 32, 1st quartile 28.25 and 3rd quartile 32.
When the composition of the DMFT index was analyzed, it was possible to ascertain that 3.3% of dental elements presented decay and 96.7% were lost. Only 270 (10.6%) teeth were found to be healthy and the mean number, per person, of teeth present in the oral cavity was 4.02. The composition of the DMFT index in male individuals was 3.52% with caries and 96.48% lost teeth; for the female sex the respective numbers were 3.16% and 96.84%.
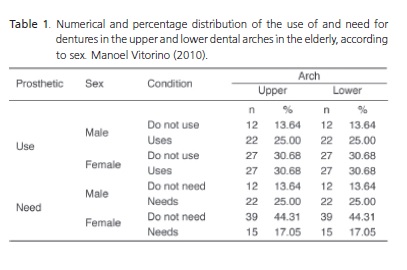
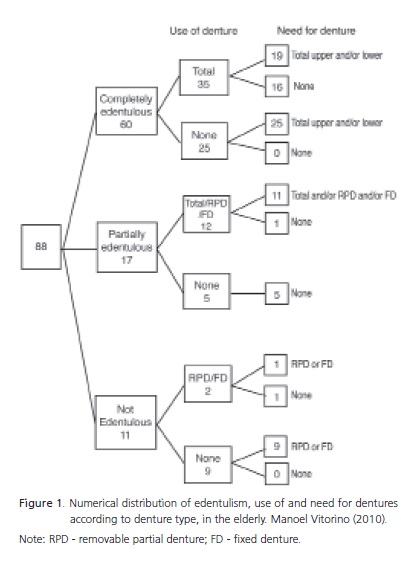
The analysis of edentulism demonstrated that 60 (68.2%) individuals were completely edentulous while 17 (19.3%) were partially edentulous. Of those who were partially edentulous, in 16 cases (94.1%), the edentulism occurred in the upper dental arch and 1 case (5.9%) in the lower arch. As far as sex is concerned, 21 males (61.8%) were completely edentulous and 9 (26.5%) partially edentulous, while in women, 39 (72.2%) were completely edentulous and 8 (14.8%) partially. Of the 49 individuals using some form of denture, 31 (63.26%) used dentures that were not fit for use.
A statistically significant difference was found between the need (or not) for upper dentures between the sexes (x2 = 11.6761 / p < 0.0005), as well as between the need (or not) for use between the upper and lower arches (x2= 24.2889 / p < 0.0001). Statistically significant differences were also found between the use (or not) of the prosthetic device and its location in the dental arch (x2= 9.2098 / p < 0.005).
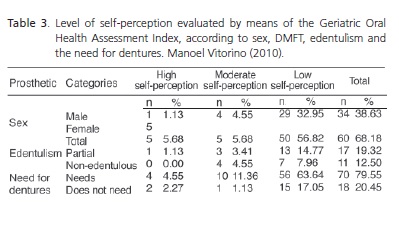
The Geriatric Oral Health Assessment Index of those examined revealed low self-perception (27.21). The relative frequencies (%) of the components of the Geriatric Oral Health Assessment Index can be seen in Table 2. In the subjective evaluation with regard to selfperception of oral health, determined using the Geriatric Oral Health Assessment Index, the disparity of the index according to the variables of sex and edentulism was relevant (Table 3).
Self-perception of the need for treatment revealed that 48 (54.54%) elderly individuals stated they did not need dental treatment. With regard to dental pain in the last 6 months, 6 (6.81%) reported recent painful symptoms. When evaluating access to dental services, it was found that 62 (70.45%) had had at least one dental appointment and in 43 of these cases (69.35%), it took place three or more years previously.
Turning to the access of the elderly to oral health services, when questioned with regard to the need to go to the dentist, 40 (45.45%) elderly individuals stated that it had been necessary to undergo dental treatment. As regards the presence of tooth pain in the last six months, only 6 (6.82%) elderly individuals reported being affected. With regard to the time that had elapsed since the last dental appointment, only 1 individual (1.13%) reported having visited the dentist within the previous year, 7 (7.95%) reported between one and two years and 43 (48.86%) three or more years previously. The place where the last dental appointment was carried out was reported as being a private consulting room by 25 (28.41%); public by 17 (19.32%) and other services by 18 (20.45%), which could signify treatment being carried out by unqualified professionals.
For 57 (64.78%) of these elderly individuals, the reason for them seeking dental treatment was the extraction of dental elements and 27 (30.68%) were unable to say. The self-perception of the elderly in relation to the quality of the treatment received showed that 13 (14.77%) rated it as very good; 41 (46.59%) as good and 30 (30.10%) were unable to say.

DISCUSSION
The increased life expectancy arising from the demographic shift in the population has symbolized a problem for the country. This is because the extra years acquired have not been lived under the best of conditions, thereby placing a greater burden on the National Health Service. This system is not yet ready to service, in a satisfactory manner, the elderly population which for the most part suffers from the consequences of chronicdegenerative diseases13.
The data obtained in the study confirm those of other authors4,7-8,13, where the majority of those examined were of the female sex. This may be explained by the difference in life expectancy between the sexes, as women are living, on average, eight years longer than men4. It was possible to note from this study that, as home visits were made during business hours, many of the men were out at work at the time of the visit, which could explain the higher percentage of women, giving rise to a high sample loss with individuals of the male sex.
The results of the clinical variables do not depart from other studies8-9,13 in which the DMFT value and the edentulism percentage are also high. The lack of public policy on oral health for the population might explain these values13, as well as the mutilation practices in the area of dentistry which still persist in many locations4, the socioeconomic conditions of the Brazilian population and the difficulty of getting access to public dental services in the municipality. In this study, it can be seen that the cultural aspects of the studied population probably contributed to dental loss, since for many of those interviewed, having no teeth equates to having no pain.
During the examinations, no restored teeth were observed, consistent with the reports of many of the elderly who stated that they had only ever been to a dentist to have teeth removed or to have dentures made up. The DMFT, therefore, was basically determined by the number of lost teeth (96.7%).
The analysis of the use of and need for dentures showed that the majority of the edentulous elderly were using dentures, however in over 60% of cases, these were not satisfactory. This may be explained by the low availability of dentures from the public services in the municipality in question, which means that they are not always accessible to all economic levels of society, and by the reluctance of the elderly to adapt to new dentures.
Results showed that women use dentures more than men, in both arches. The concern over esthetics is important for the oral condition, seeing as women reported preferring to use dentures rather than keep their esthetically less flattering, decayed teeth. This may even explain the higher number of elderly who use upper dentures than those who use lower dentures, as upper dentures have a greater direct influence on esthetics.
As regards the need for restorative treatment, men require more upper dentures (25%) than women (17%), which is also probably explained by the esthetic question. As for the lower dentures, women require more dentures (48.9%) than men (29.5%).
The Geriatric Oral Health Assessment Index rated the sample as having low self-perception, with a value of 27.2. This number was lower than that obtained in a separate survey conducted with a group of elderly people13. In this study, by linking the Geriatric Oral Health Assessment Index to the DMFT, it was possible to identify that individuals ranked as having high self-perception, presented the highest DMFT. Studies on perception show that most people perceive their oral condition to be good, even when they have an unfavorable clinical condition. This occurs due to the fact that clinical measurements of oral health used by professionals are weak predictors of people's selfperception9. So, many elderly people consider their condition to be a consequence of ageing13.
The elderly who need dentures, but do not use them or use unsatisfactory dentures, were the determining factors in the low Geriatric Oral Health Assessment Index, the majority of them being rated as low self-perception.
The percentage of elderly which reported never having had difficulty in chewing (51.1%), speaking (68.2%) or swallowing (93.2%) may be explained by the length of time they have been using the dentures, which has given rise to a solid, functional adaptation. Esthetics appear to be important as 45 (51.14%) reported not being happy with the appearance of their smile. As for the use of medication, 56 (63.64%) stated they had used some form of medication to reduce toothache. One hypothesis for this fact may lie with pulpitis generated by caries that affects a large part of the dental structure, causing pain in the majority of the population studied.
With regard to access to services, those examined who reported not needing dental treatment (51%), probably responded this way as they had few or no teeth at all in the arch and as they considered their dentures as adequate for use. The other questions revealed the lack of public dental services on offer, with the greater percentage of consultations being carried out privately (40.3%) or in practices (29%). The majority of those examined only visited the dentist to have teeth extracted, generally at least three years previously. This situation may be explained by the lack of preventive treatment and oral health promotion available in the past.
CONCLUSION
It is possible to conclude from the data obtained that the oral health condition of the elderly living in the urban zone of the municipality of Manoel Vitorino is precarious. Tooth loss accounts for almost the entire DMFT index and the need for dentures was shown to be high. The elderly demonstrated low self-perception of their oral condition and their access to public oral healthcare is not satisfactory.
It is clear, therefore, that the municipality needs to implement oral health programs focusing on both prevention and promotion and which meet the actual needs of the residents, so that in the future, better oral health conditions may be available for the elderly. At this point in time, it is necessary to establish oral rehabilitation policies so that the large elderly portion of the population that requires restorative treatment can be properly helped.
ACKNOWLEDGMENTS
To the Research Support Foundation in the state of Bahia for the Scientific Initiation grant and to the Southwest Bahia State University for funding the research project.
Collaborators
CA CASOTTI was responsible for the production of the project, examiner standardization, sample selection, data analysis and composition of the article. LA LIMA was responsible for the data collection and composition of the article. DL GOMES FILHO and KMS FRANCISCO were responsible for the analysis, data tabulation and composition of the article.
REFERENCES
1. Pucca Júnior GA. A saúde bucal do idoso: aspectos demográficos e epidemiológicos [texto na Internet]. In: Portal Educação [homepage na Internet]. Brasília: Portal Educação; 2008 [citado 2010 Mar 26]. Disponível em: < http://www.portaleducacao.com.br/odontologia/artigos/3050/a-saudebucal-do-idoso-aspectos-demograficos-e-epidemiologicos> [ Links ].
2. Murakami AMU, Moysés SJ, Moysés ST. Equidade frente a necessidade de prótese dentária na população de 65 a 74 anos de idade em Curitiba. Epidemiol Serv Saúde. 2007;16(2):139- 41. doi: 10.5123/S1679-49742007000200014.
3. Instituto Brasileiro de Geografia e Estatística. IBGE Planejamento [citado 2010 Maio 25]. Disponível em: <http://www.ibge.gov.br/home/presidencia/noticias/noticia_visualiza.php?id_noticia=1275&id_pagina=1>.
4. Caldas Júnior AF, Caldas KU, Oliveira MRM, Amorim AA, Barros PMF. O impacto do edentulismo na qualidade de vida de idosos. Rev Ciênc Med. 2005;14(3):229-38.
5. Narvai PC, Biazevic MGH, Junqueira SR, Pontes ERCJ. Diagnóstico da cárie dentária: comparação dos resultados de três levantamentos epidemiológicos numa mesma população. Rev Bras Epidemiol. 2001;4(2):72-80. doi: 10.1590/S1415-790X2001000200002.
6. Frias AC, Antunes JLF, Narvai PC. Precisão e validade de levantamentos epidemiológicos em saúde bucal: cárie dentária na Cidade de São Paulo, 2002. Rev Bras Epidemiol. 2004;7(2):144-54. doi: 10.1590/S1415- 790X2004000200004.
7. Colussi CF, Freitas SFT, Calvo MCM. Perfil epidemiológico da cárie e do uso e necessidade de prótese na população idosa de Biguaçu, Santa Catarina. Rev Bras Epidemiol. 2004;7(1):88-97. doi: 10.1590/S1415-790X2004000100011.
8. Silva DD, Sousa MLR, Wada RS. Autopercepção e condições bucal em uma população de idosos. Cad Saúde Pública. 2005;21(4):1251-9. doi: 10.1590/S0102- 311X2005000400028.
9. Silva SRC, Rosell FL, Valsecki Júnior A. Percepção das condições de saúde bucal por gestantes atendidas em uma unidade de saúde no município de Araraquara, São Paulo, Brasil. Rev Bras de Saúde Mater infant. 2006;6(4):405-10. doi: 10.1590/ S1519-38292006000400007.
10. Instituto Brasileiro de Geociências e Estatística. IBGE Cidades Planejamento [citado 2010 Maio 26]. Disponível em: <http://cidades.ibge.gov.br/xtras/home.php>.
11. Brasil. Ministério da Saúde. SB Brasil 2010 - Pesquisa Nacional de Saúde Bucal de 2010: proposta de projeto técnico para consulta pública [citado 2009 Set 14]. Disponível em: <portal.saude.gov.br/portal/arquivos/pdf/pesquisa_nacional_ bucal_0609.pdf>.
12. Atchison KA, Dolan TA. Development of the Geriatric Oral Health Assessment Index. J Dental Educ. 1990;54(11):680-7.
13. Dias CA, Rodrigues SM, Pereira VG, Oliveira LS, Cordeiro GP, Dias LCS. Interferência da saúde bucal do idoso em sua vida social e afetiva. In: XIII Seminário sobre Economia Mineira; 2008; Belo Horizonte. Anais, Belo Horizonte: Universidade Federal de Minas Gerais; 2008.
 Correspondence to:
Correspondence to:
CA CASOTTI
e-mail: casottica@hotmail.com
Received on: 28/3/2011
Approved on: 27/5/2011
