










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre Abr./Jun. 2012
ORIGINAL / ORIGINAL
Odontometric reliability of Root ZX II
Avaliação da confiabilidade odontométrica do Root ZX II
André Akira NAKATSUKA I; Cleber Keiti NABESHIMA I; Maria Letícia Borges BRITTO I
I Universidade Cruzeiro do Sul, Faculdade de Odontologia. Rua Galvão Bueno, 868, 01506-000, Liberdade, São Paulo, SP, Brasil
ABSTRACT
Objective
This study analyzed the reliability of the electronic apex locator Root ZX II (J. Morita Corp., Kyoto, Japan) in different roots using the apical locator with the rotary unit.
Methods
The working length of the roots of twenty-two upper molars was established 0.5 mm short of the apex visually, using a ruler. The teeth were fixed on an support and shaped using the ProTaper rotary system with the Root ZX II (J. Morita Corp., Kyoto, Japan) device calibrated to 0.5 Ncm and 500 rpm. Next, an F3 gutta-percha cone was introduced in the root canal and assessed visually. The data of the different canals, that is, mesiobuccal, distobuccal and lingual, were treated by the Chi-square test.
Results
The Root ZX II (J. Morita Corp., Kyoto, Japan) device located the working length correctly 79% of the time and no differences were observed among the different root canals (p>0.05).
Conclusion
When the Root ZX II apex locator is used with your rotary unit (J. Morita Corp., Kyoto, Japan) device, the percentage of clinically acceptable measurements is good, and the position of the root canal did not affect the working length.
Indexing terms: Endodontics. Odontometry. Root canal therapy. Tooth apex.
RESUMO
Objetivo
Analisar a confiabilidade do Root ZX II (J. Morita Corp., Kyoto, Japão) utilizando o localizador apical associado com sua unidade de instrumentação rotatória, variando o tipo de raiz.
Métodos
Vinte e dois molares superiores foram medidos visualmente com auxílio de uma régua, onde se estabeleceu a medição odontométrica visual em 0,5 mm aquém do limite apical. Assim os dentes foram adaptados num suporte confeccionado em resina acrílica, e instrumentados utilizando-se do sistema ProTaper em conjunto com o Root ZX II (J. Morita Corp., Kyoto, Japão) calibrado em torque 0,5 à 300 rpm no reverso automático em 0,5 mm. Após instrumentação, um cone principal foi introduzido e analisado visualmente. Os dados obtidos em diferentes raízes (mesial, distal e palatina) foram submetidos ao teste do Qui-quadrado.
Resultados
Os resultados mostraram um percentual de 79% de acerto na medida preestabelecida. A análise estatística não apresentou diferença significante entre a posição dos canais (p>0,05).
Conclusão
Pode-se concluir que o Root ZX II (J. Morita Corp., Kyoto, Japão) com unidade odontométrica acoplada à sua unidade rotatória apresenta bom percentual de medidas clínicamente aceitáveis, onde a posição do canal não influenciou no limite de trabalho.
Termos de indexação: Endodontia. Odontometria. Tratamento do canal radicular. Ápice dentário.
INTRODUCTION
Endodontics is the specialty area of dentistry that treats the root canal system. Inflammation and/or infection in the root canals may damage the pulpal tissue and periapex.
Among the stages of endodontic therapy, odontometry aims to determine the working length of a canal and root apex, promoting better healing of the periapical tissues and a more favorable postoperative period.
Many odontometric methods based on radiography are used to this day but determination of the real working length is a problem because radiographs are two-dimensional. This is evidenced when radiographs of instrumented and obturated teeth reveal that the obturation cone crossed the apex, showing that the radiographic location of the apex may be misleading1.
The first electronic device for determining the working length of a canal was introduced by Sunada in 1962. It basically consisted of a microamperimeter, a potentiometer and two electrodes. The working length was calculated after the device was calibrated and file placed in the canal, but the results were only accurate if the canal was dry2.
In the 1980s, the search began for new apex locators that would work in the presence of moisture, and the result was the APIT, launched in 1989. The APIT was tested in root canals irrigated with a sodium hypochlorite solution, and proved to have an accuracy of 98%3.
Since then, a variety of devices and generations emerged and studies tested their efficacies. Ex vivo comparison of the accuracy of the apex locators Root ZX, RomiApex D-30 and Ipex showed that they may have different reliability levels, depending on the estimated working length. The Root ZX seemed not to be negatively affected 1 millimeter short of the apical foramen, showing a reliability of 97.4%4. This device was also compared with the conventional radiographbased method, obtaining a higher rate of accurate apical measurements5-6.
Eventually, electronic odontometric devices were coupled with an rotary instrumentation unity, such as the Tri Auto ZX and Root ZX II (J. Morita Corp., Kyoto, Japan). The TRI Auto ZX was evaluated, and it was observed accuracy of 66.7% to 81% when the device was calibrated to working length 0.5mm short of the apical foramen7-8. In another study, using two distinct Tri Auto ZX calibrations, 1mm or 2mm beyond the apex, the 1mm calibration proved to be more accurate because of its greater proximity to the apical constriction9.
The Root ZX II (J. Morita Corp., Kyoto, Japan) was using odontometric and rotary units in single-rooted teeth. Its accuracy was 90.5% when calibrated 0.5mm short of the apex and 83.78% when calibrated 1 mm short of the apical foramen. However, the 0.5mm calibration resulted in more measurements in excess of the working length10.
The anatomical complexity of different tooth groups needs to be considered. The upper molars are among the most varying teeth, since they have three roots with canals of different shapes, diameters and inclinations, in addition to having a greater rate of endodontic indications than the anterior teeth and premolars.
The objective of the present ex vivo study was to test the accuracy of the Root ZX II (J. Morita Corp., Kyoto, Japan) electronic apex locator and its performance in different roots of upper molars.
METHODS
Twenty-two upper molars were used for the present study, totaling 66 canals. The coronal and middle thirds of all canals were previously enlarged by the Gates Glidden drills 1, 2 and 3 (Dentsply Maillefer, Ballaigues, Switzerland), followed by a K15 file (Dentsply Maillefer, Ballaigues, Switzerland) for inspection, aided by a magnifying glass. Visual working length was estimated 0.5mm short of the apical foramen.
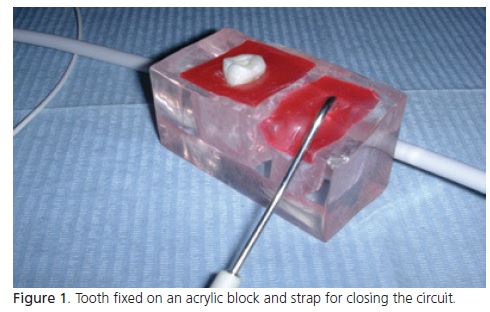
All teeth were fixed on an acrylic support containing saline (LBS Laborasa, São Paulo, Brazil) (Figure 1).
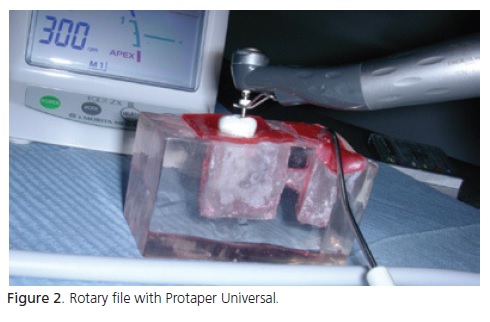
Instrumentation was done by the system Protaper (Dentsply Maillefer, Ballaigues, Switzerland) in the sequence SX-S1-F1-S2-F1-F2-F3, along with Endo- PTC (Fórmula & Ação, São Paulo, Brazil) and 1% sodium hypochlorite (Fórmula & Ação, São Paulo, Brazil). The Root ZX II (J. Morita Corp., Kyoto, Japan) odontometric device was used with the rotary unit, using a torque of 0.5Ncm at 300 rpm and automatic apical reverse activated 0.5 mm short of the apical foramen (Figure 2).
After instrumentation, a Protaper F3 gutta-percha cone (Dentsply Maillefer, Ballaigues, Switzerland) was fitted in the canal. The working length obtained visually before instrumentation and length of gutta-percha cone fitted post-instrumentation were used for classifying the gutta-percha cone tip position inside the canal.
The data were treated by the Chi-square test according to root (mesiobuccal, distobuccal and lingual), the level of significance was set at 5%.
The study complied with all the ethical principles set forth by the Declaration of Helsinki (2000) and Brazilian legislation, and was approved by the University Cruzeiro do Sul Research Ethics Committee, protocol number 050/06.
RESULTS
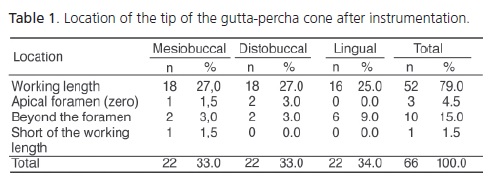
In general, 79% of the cones matched the working length and 21% were either short of the working length, reached the apical foramen or exceeded the apical foramen. The different positions of the canals are listed in Table 1.
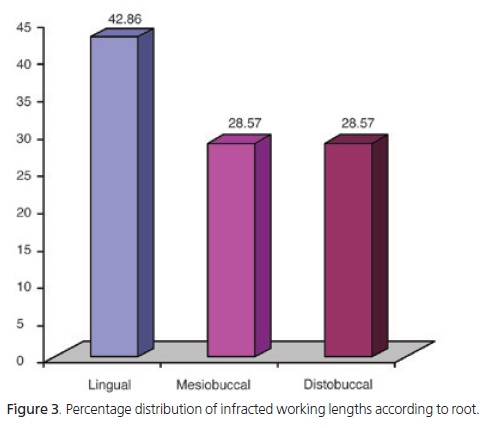
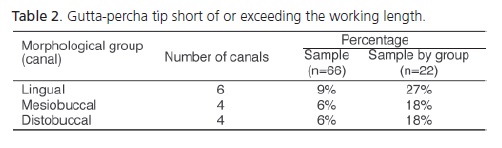
Of all the canals, 6 lingual, 4 mesiobuccal and 4 distobuccal were short of or exceeded the working length, corresponding to 9%, 6% and 6%, respectively, of a sample of 66 canals. Considering the roots individually (22 canals each), the tip of the gutta-percha cone was either short of the working length or exceeded it in 27% of the lingual canals, 18% of the mesiobuccal canals and 18% of the distobuccal canals (Table 2), but there was no significant difference among these percentages (p=0.6958).
Figure 3 shows the percent distribution of infracted working lengths according to root.
DISCUSSION
The determination of the actual tooth length and canal working length has been attempted for centuries by many methods, such as: pain when the periapical tissue is reached, radiographs, geometrical methods. However, electronic methods have been emerged in the last decades.
Working length estimation by electronic devices has been investigated because the two-dimensionality of radiographs sometimes prevents a clear view of the location of the apical foramen. Electronic apex locators are very effective3,8,11.
However, the two-dimensionality of radiographs is not the only problem. Other factors affect the measurement of the working length, such as root shape, depending on the instrumentation method12-13.
Many studies using electronic apex locators have reported high success rates, but their samples consisted of straight single-rooted teeth with developed apexes4,8,10,14-15. Therefore, studies on different teeth were needed, since the diameter of the apical foramen may also affect working length estimation11,16.
Along with the emergence of electronic apex locators, endodontics underwent another advance with the emergence of rotary files, since they shape canals more uniformly, wearing the coronal and middle thirds more, where most of the contamination is, and the apical third less, achieving good canal decontamination17.
This led to the proposal of uniting both technologies in a single device, a digital apex locator that uses a rotary file simultaneously. The efficacy of one such device, the electronic apex locator Root ZX II (J. Morita Corp., Kyoto, Japan), was tested. It uses a rotary file, which allows automatic instrumentation of the working length.
The ex vivo study design is justified because it would be impossible to extract a tooth for assessment or to determine the extent of instrumentation in vivo with conventional radiographic methods, since conventional radiography is two-dimensional and the two roots would superpose each other in the radiograph and prevent a clear view of the apex of interest. Hence, being able to look directly at the apex with a magnifying glass provided better assessments.
Many techniques and adaptations have been proposed for studying apex locators in vitro. In the oral cavity, one electrode is fastened at file and the other is kept in contact with the moist buccal mucosa to close the circuit and send the data to the meter. Therefore, when the study is done in vitro, a conductive medium is necessary to close the circuit, such as neutral or buffered salt agar15,18, sodium hypochlorite19 or alginate4-5,10,20. The present study used saline because it is electrically conductive.
The results were assessed according to the final position of the tip of the principal gutta-percha cone: short of the working length, at the working length, or beyond the working length, either reaching the apical foramen (known as zero) or exceeding it.
Only one cone tip among the 66 treated canals was short of the working length. This may be explained by the very small diameter of the apical third produced by last rotary file. Longer working-time using the last file could produces larger preparations.Situations where the tip of the cone reaches the apical foramen are clinically acceptable. But since the limit was defined as 0.5 mm short of the apical foramen, these situations were considered failures. The same is true for the single cone tip that stayed 1.5mm short of the apical foramen. This is also clinically acceptable because this distance is within the definition of working length20.
Therefore, if one considers that reaching the apical foramen and being short of the physiological foramen (constriction) are clinically acceptable, the percentage of successful results would be 85%, which can be considered a increase of satisfactory results obtained by the study apex locator.
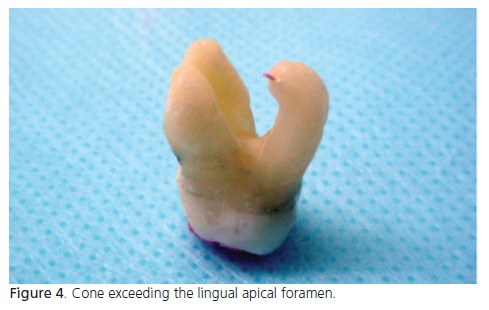
Almost half (42.86%) the cone tips that exceeded the apical foramen regarded the lingual root canal. This can be explained by the occasional apical to vestibular curvature of this root, which may also incline towards the other roots (Figure 4). However, the percentages of cone tips that exceeded the apical foramen of the different root groups were not significantly different.
A greater canal diameter can also affect the results since the absence of apical constriction reduces voltage, reducing impedance in the apical region and accuracy of the reading, especially in cases where the pulp is dead. Together, dead pulp and wider foramen may decrease accuracy14. Furthermore, the automatic reverse function of the rotary file has been questioned, since it may increase wearing and thereby, the diameter of the apical foramen21-22. However, the Root ZX II (J. Morita Corp., Kyoto, Japan) apex locator has many settings, including the deactivation of the automatic reverse function when the working length is reached, so future studies should test its accuracy when other settings are used.
CONCLUSION
Root ZX II (J. Morita Corp., Kyoto, Japan) using odontometric and rotary units has high success rate when clinically acceptable measurements are considered. Different root canal positions did no influence on the odonometric reliability of Root ZX II.
Collaborators
AA NAKATSUKA performed all the experimental work and wrote the article. CK NABESHIMA designed the methodology, helped to write the article and reviewed the text. MLB BRITTO supervised the literature search, methodology and helped to write the article.
REFERENCES
1. Machado MEL, Pesce HF. Estudo da região apical de dentes tratados endodonticamente até o vértice radiográfico da raiz. Rev Assoc Paul Cir Dent. 1981;35(6):534-7. [ Links ]
2. Sunada I. New method for measuring the length of root canal. J Dent Res. 1962;41(2):375-87. doi: 10.1177/00220345620410020801.
3. Nishiyama CK, Duarte MAH, Godoy FF, Moraes IG, Almeida CM. Avaliação clínica da eficiência de um aparelho eletrônico empregado na determinação da odontometria. Rev Bras Odontol. 1994;51(6):45-8.
4. Vasconcelos BC, Vale TM, Menezes AST, Pinheiro-Junior EC, Vivacqua-Gomes N, Bernardes RA, et al. An ex vivo comparison of root canal length determination by three electronic apex locators at positions short of the apical foramen. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(2):e57-61. doi: 10.1016/j.tripleo.2010.03.005.
5. Kaufman AY, Keila S, Yoshpe M. Accuracy of a new apex locator: an in vitro study. Int Endod J. 2002;35(2):186-92. doi: 10.1046/j.1365-2591.2002.00468.x.
6. Vieyra JP, Acosta J, Mondaca JM. Comparison of working length detrmination with radiographs and two electronic apex locators. Int Endod J. 2010;43(1):16-20. doi: 10.1111/j.1365- 2591.2009.01620.x.
7. Alves AMH, Felippe MCS, Felippe WT, Rocha MJC. Ex vivo evaluation of the capacity of the Tri Auto ZX to locate the apical foramen during root canal retreatment. Int Endod J. 2005;38(10):718-24. doi: 10.1111/j.1365-2591.2005.01007.x.
8. Altenburger MJ, Çenik Y, Schrrmeister JF, Wrbas K-T, Hellwig E. Combination of apex locator and endodontic motor for continuous length control during root canal treatment. Int Endod J. 2009; 42(4):368-74. doi: 10.1111/j.1365-2591.2008.01535.x.
9. Carneiro E, Bramante CM, Picoli F, Letra A, Silva Neto UX, Menezes R. Accuracy of root length determination using Tri Auto ZX and Protaper instruments: an in vitro study. J Endod. 2006;32(2):142-4. doi: 10.1016/j.joen.2005.10.030.
10. Versiani MA, Santana BP, Caram CM, Pascon EA, Souza CJA, Gabrielli JCG. Ex vivo comparison of the accuracy of Root ZX II in detecting apical constriction using different meter's reading. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(1):e41- 5. doi: 10.1016/j.tripleo.2010.03.005.
11. Giusti EC, Fernandes KPS, Lage-Marques JL. Medidas eletrônica e radiográfica digital na odontometria: análise in vivo. RGO - Rev Gaúcha Odontol. 2007;55(3): 239-46.
12. Machado MEL, Machado MLBBL, Antoniazzi JH. Eficácia da técnica seriada convencional e das técnicas escalonadas apicocervical e cervico-apical no preparo químico-cirúrgico de canais curvos. Rev Bras Odontol. 1998;55(2):52-5.
13. Pesce H, Machado MEL, Sydney GB. Variação da odontometria no preparo de canais curvos. Rev Univ São Francisco. 1986;4:19-22.
14. Ramos CAS, Bernardineli N. Avaliação in vivo da precisão de leitura de um modelo de localizador apical eletrônico. UNOPAR Cient Ciênc Biol Saúde. 2001;3:9-20.
15. Czerw RJ, Fulkerson MS, Donnely JC. In vitro evaluation of the accuracy of several electronic apex locator. J Endod. 1995;21(11):572-5. doi: 10.1016/S0099-2399(06)80988-X.
16. Ramos CAS, Bernardineli N. Influência do diâmetro do forame apical na precisão de leitura de um modelo de localizador apical eletrônico. Rev Fac Odontol Bauru. 1994;2:83-90.
17. Machado MEL, Sapia LAB, Cai S, Martins GHR, Nabeshima CK. Comparison of two rotary systems in root canal preparation regarding disinfection. J Endod. 2010;36(7):1238-40. doi: 10.1016/j.joen.2010.03.012.
18. Nahmia SY, Aurélio J, Gerstein H. An in vitro for evaluation of electronic root canal length measuring devices. J Endod. 1987;13:209-14.
19. Jenkins JA, Walker WA, Schindler WG, Flores CM. An in vitro evaluation of the accuracy of the Root ZX in the presence of various irrigates. J Endod. 2001;27:209-11.
20. Angwaravong O, Panitvisai P. Accuracy of an electronic apex locator in primary teeth with root resorption. Int Endod J. 2009;42(2):115-21. doi: 10.1111/j.1365-2591.2008.01476.x.
21. Felippe WT, Felippe MCS, Carmona JR, Crozoé FCI, Alvisi BB. Ex vivo evaluation of the ability of the ROOT ZX II to locate the apical foramen and to control the apical extent of rotary canal instrumentation. Int Endod J. 2008;41(6):502-7. doi: 10.1111/j.1365-2591.2008.01386.x.
22. Topuz Ö, Uzun Ö, Tinaz AC, Bodrumlu E, Görgül G. Accuracy of two apex-locating handpieces in detecting simulated vertical and horizontal root fractures. J Endod. 2008;34(3):310-3. doi: 10.1016/j.joen.2007.12.018.
 Correspondence to:
Correspondence to:
MLB BRITTO
e-mail: leticiabritto@globo.com
Received on: 4/12/2010
Final version resubmitted on: 11/7/2011
Approved on: 27/9/2011
