










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre Abr./Jun. 2012
ORIGINAL / ORIGINAL
Features of selective examinations for dentists in Brazil
Caracterização dos concursos públicos para cirurgiões dentistas no Brasil
Suzana Naomi MATSUMOTO I; Marcos Sérgio ENDO II; Raquel Sano Suga TERADA I; Luiz Fernando LOLLI III; Mitsue FUJIMAKI I
I Universidade Estadual de Maringá, Departamento de Odontologia. Av. Mandacaru, 1550, Bloco S-08, 87080-000, Maringá, PR, Brasil
II Universidade Estadual de Campinas, Faculdade de Odontologia, Departamento de Clínica Integrada. Piracicaba, SP, Brasil
III Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia, Departamento de Odontologia Preventiva e Social. Araçatuba, SP, Brasil
ABSTRACT
Objective
The aim of this work was to analyze the features of selective examinations offered by City Councils, to work as dental practitioners at Health Centers and/or become part of the Dental Health Team of the Family Health Program, presenting the number of vacancies offered, salaries, hours of work as well as the content of the test applied.
Methods
For this study, 272 examinations available on the internet were selected: 218 for general dental practitioners and 54 for the Family Health Program, offered by Municipalities in Brazil, in 2006. The number of vacancies offered, salary ranges, hours of work and content of the test applied were analyzed.
Results
It was found that 1,205 (71%) vacancies were to work at the Health Centers and 486 (29%) at the Family Health Program. Furthermore, the salaries paid by 64% of City Councils were below the basic minimum for dentists. As regards the tests, these varied in content, but all required specific knowledge ranging from 3% to 97% of test subject matter.
Conclusion
In 2006, there was a small number of vacancies offered for family health strategy; the salaries offered in most selective examinations were not attractive, which showed that a greater commitment by management, a higher investment in the National Health Service and appreciation of the workforce in these services is required with regard to consolidating the family health strategy.
Indexing terms: Dentistry. Family Health Program. Health Manpower. National Health System.
RESUMO
Objetivo
Analisar as características dos concursos públicos ofertados por Prefeituras Municipais, ou seja, para atuarem nas unidades básicas de saúde como clínico geral e/ou para integrar a Equipe de Saúde Bucal da Estratégia Saúde da Família, apresentando o número de vagas ofertadas, a faixa salarial, a carga horária de trabalho bem como o conteúdo das provas aplicadas.
Métodos
Neste estudo foram selecionados 272 concursos disponíveis em meio eletrônico, sendo 218 para cirurgião-dentista clínico geral e 54 para a Estratégia Saúde da Família, ofertados pelas Prefeituras Municipais do Brasil. Foram analisados o número de vagas ofertadas, faixa salarial, carga horária de trabalho e conteúdo das provas aplicadas.
Resultados
Observou-se que 1.205 (71%) vagas eram para atuação nas unidades básicas de saúde e 486 (29%) para a Estratégia Saúde da Família. Verificou-se também que o salário pago por 64% das Prefeituras Municipais não atingiu o piso salarial para cirurgião-dentista. Em relação às provas, o conteúdo exigido foi variado, porém todas requereram conhecimento específico que variou de 3% a 97% da constituição das mesmas.
Conclusão
No ano de 2006 houve uma pequena porcentagem das vagas ofertadas para cirurgião-dentista para a Estratégia Saúde da Família, os salários, na maioria dos concursos, não eram atrativos, mostrando ser necessário um maior empenho dos gestores na consolidação da Estratégia Saúde da Família e maior investimento e valorização para os trabalhadores do Sistema Único de Saúde.
Termos de indexação: Odontologia. Programa Saúde da Família. Recursos Humanos em Saúde. Sistema Único de Saúde.
INTRODUCTION
In recent decades, Brazil's health service has been faced with considerable changes1, ranging from a centralized, privatized system which in the 1970s excluded the most needy elements of the population from healthcare, to the significant changes that have occurred following the Health Reform Movement which culminated in the consolidation of the National Health System (SUS), enshrined in the 1988 Constitution2. Various discussions were had during the 1990s concerning the ways to implement a public health policy that would be complete and all-embracing, coping with the lack of financial support, the emergence of new technology and equipment, the lack of human resources prepared to be put to work in the national health system and, amongst the many other problems, the accelerated growth of private health companies.
In order to reorganize the practice of healthcare on new foundations and to replace the traditional welfare model, the Ministry of Health implemented, in 1994, the Family Health Strategy with the aim of bringing health and the family closer together and improving the quality of life of the Brazilian people. The Family Health Strategy was intended to be a tool to reorganize and restructure the public health system3. This program was consolidated in 1998 as a strategy for a healthcare model that prioritizes actions guided by the principles of territorialization, intersectorial activity, decentralization, joint responsibility and fairness, especially in those population groups with a higher risk of falling sick or dying, i.e. in harmony with the principles of the SUS4. The Family Health Strategy operates by means of the implementation of multi-professional teams in Basic Health Units, composed of one doctor, one nurse and between four and six community health workers. These teams are responsible for monitoring a specific number of families (around one thousand families per team). The teams work on activities that include health promotion, prevention, recovery, convalescence from the more frequent illnesses and ailments and maintaining health in the community.
As from 2000, following the introduction of directive 1444 of 28 December, Oral Health Teams5 were also included. So these professionals and the population being monitored create bonds of joint responsibility that help to identify and service health issues in the community. In addition, they encourage the organization of society to exercise social control over health actions and services; they operate on an intersectorial basis by way of partnerships established with a variety of social and institutional segments, so as to be able to intervene in situations that are outside the specific scope of the health sector. The Family Health Strategy and the Oral Health Teams represent a distinct, dynamized strategy by aiming principally at aspects of health promotion and maintenance.
With the creation of the Oral Health Teams, new selective examinations for the position of dental surgeon have emerged all over Brazil, in addition to those already offered for working in the Basic Health Units as general practitioners. In addition, the demand by professionals for public sector positions has also been on the rise in recent years, taking into account the saturated market in the private sector, and academics are already showing interest in undergraduates. However, as yet, no study has been conducted which characterizes the selective examinations administered in the country.
The aim of this study, therefore, was to analyze the characteristics of the selective examinations offered by city councils in 2006, both for working in the Basic Health Units as general practitioner and/or being part of the Family Health Strategy's Oral Health Team, by conducting a survey of the number of vacancies offered, salary bands, working hours, as well as the content of the selective examinations themselves.
METHODS
Choice of selective examinations
The search for selective examinations was carried out by accessing the three most frequently accessed websites for the publication of selective examinations in Dentistry: www.odontoconcursos.com.br, www.pciconcursos.com.br and www.concursosdeodontologia.com.br, which publish information on selective examinations for dental surgeons administered by city councils across the whole of Brazil. From these three websites, a total of 272 selective examinations administered in 2006 were selected, for the positions of general dental practitioner and dental surgeon for the Family Health Strategy. The examinations offered were checked against the respective publications to confirm the number of vacancies, salary and working hours. Those selective examinations which did not provide details of websites for the acquisition of further information were discarded. Examinations for any kind of specialist position were also discarded.
The salaries of those positions evaluated were transformed and standardized to assume a 40-hour working week in order to enable comparison.
Choice of tests
The tests available in electronic file format on the websites accessed, were selected for analysis. In total, 40 tests were evaluated, of which 30 were for the position of general dental practitioner and 10 for the position of dental surgeon for the Family Health Strategy. Each test was analyzed individually and the questions were subdivided into topics.
RESULTS
A total of 272 selective examinations were located: 218 for general dental practitioners and 54 for dental surgeons for the Family Health Strategy, all carried out in 2006. The working weeks for these positions varied between 10 and 45 hours.
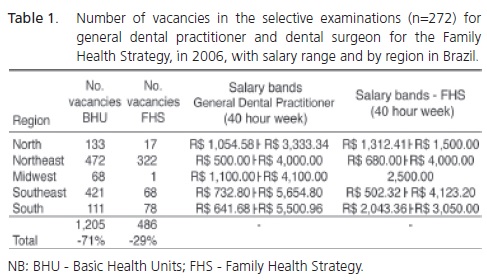
Table 1 shows the number of vacancies available for the position of dental surgeon to work in the Basic Health Units and to be part of the Family Health Strategies. There were around three times more vacancies for dental surgeons working in the Basic Health Units than those in the Family Health Strategy. The highest concentration of openings was found in the Northeast region, with a total of 794 vacancies. The salaries paid by the city councils for the position of dental surgeon working in the Basic Health Units and for the same position in the Family Health Strategy were computed assuming a 40-hour working week, in order to permit comparisons of salary amounts. As far as the former position is concerned, there was a large variance in the salary band in the various regions of Brazil, the lowest monthly salary being offered by the city council of Nova Floresta in the state of Paraíba, in the sum of R$500,00. The highest salary was found for the selective examination set by the city council of Mogi das Cruzes, in the state of São Paulo, which amounted to R$ 2,827.40 for a 20 hour working week, i.e. when prorated to a 40-hour working week, the salary would amount to R$ 5,654.80.
As for the position of dental surgeon for the Family Health Strategy, we also found a large variance in the salary structure, the lowest salary being R$ 502.32 for a 40-hour working week, paid by the city council of Raul Soares, in the state of Minas Gerais. The highest salary was found with the city council of Atibaia, in the state of São Paulo, amounting to R$ 4,123.20.
The means and percentage variances for the questions in the selective examinations, by topic, in the tests evaluated, are shown in Table 2. On average, the most common topic addressed (46% of the questions) was 'Specific Knowledge', with a variance of between 3% and 97% of the test questions. Of the 40 tests analyzed, only one contained questions relating to IT, thereby explaining the low percentage (0.3%). Another common subject was the Portuguese language, attaining a mean of 24% of all the tests evaluated and, in one test alone, equating to 47% of the questions.

DISCUSSION
The implementation of the National Health System (SUS), complying with its principles, in a country that possesses huge territorial dimensions and marked regional disparities, a federative political system composed of three spheres of government (Federal, State and Municipal) considered to be federative entities with administrative autonomy and without any hierarchical connections, as well as sharp inequalities and social exclusion, demands an intimate knowledge of the whole population, working in a decentralized fashion in accordance with the needs of each region. The insertion of oral health into the Family Health Strategy represents the creation of an area for practices and relationships to be built for the reorientation of the working process and for the proper operation of oral health within the scope of the health services. Accordingly, oral health care is beginning to dictate the shaping of a work team that can relate to the users and which can participate in the administration of services in order to respond to the actual demands of the population and expand access to the actions and services of oral health promotion, prevention and recovery by employing both collective and individual measures and through the establishment of a territorial connection. So, with the aim of restructuring the healthcare model and expanding access to oral health actions, thereby assuring complete care for individuals and families, Oral Health Teams have started to be included in the Family Health Strategy, regulated by Directive GM/MS 267 of 6 March, 2001.
There has been a significant growth in Family Health Teams and a consequent increase in the coverage of the population over recent years. By 2009, of the 5,564 municipalities in Brazil, a total of 5,248 depended on the Family Health Strategy (30,188 teams). Moreover, 4,698 municipalities possess a total of 18,820 Oral Health Teams (MS/SAS/DAB, 2012). However, when the number of dental surgeon vacancies was analyzed for the Family Health Strategy, in comparison with the number of vacancies to work as general practitioner, in 2006, it was found that the Family Health Strategy is still not the most predominant. Of the total number of vacancies, 71% are for working as general practitioner and 29% for the Family Health Strategy. Accordingly there seem to be some obstacles, difficulties to be surmounted before these numbers can approach ideal levels, despite all the financial incentives. Amongst the most recent National Health System operating directives is the Health Pact published through Directive/GM 399 of 22 February, 2006. It represents a set of institutional reforms of the National Health System agreed amongst the three spheres of government, with the aim of promoting innovation in the management tools and processes, with the aim of achieving greater efficiency and quality of response in the System. At the same time, the Pact restates the constitutional principles of social welfare and seeks equity. One of the policies of the Pact for Life is to consolidate and strengthen Basic Healthcare, prioritizing the Family Health Strategy5. Despite the fact that we found only 29% of the dental surgeon vacancies being for the implementation of Oral Health Teams, it is expected that this proportion has grown in recent years and that the administrators understand the need to change the healthcare model based on the strengthening of basic care and undertake a process of hiring professionals to work in the Family Health Strategy. Initially what is needed is to have a leveling out of the number of Oral Health Teams in relation to the Family Health Strategy, and subsequently the expansion and maintenance of both. At the present time, the total number of Family Health Strategy teams exceeds that of the Oral Health teams by more than 12,300. This process of change across the entire country began with the implementation of the program and it is believed that, with continuing investment in this strategy, we shall attain, over time, even more satisfactory numbers. In addition, a figure of 2 dental surgeons per Family Health Strategy6 has been recommended, as these teams handle an average of 3,000 people while the World Health Organization (WHO) advocates a ratio of 1 dental surgeon for every 1,500 inhabitants. These data show that there are unfilled vacancies for dental surgeons to work within the Family Health Strategy7.
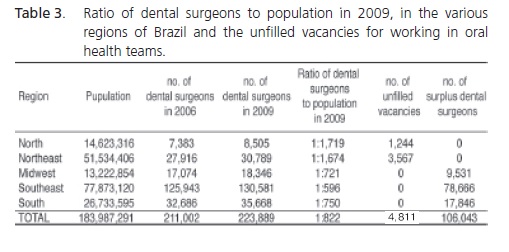
Moreover, it can be seen that the number of dental surgeons registered with the Federal Dental Council7 in the regions of the Midwest, South-East and South, exceeds the recommendation of the WHO as there is one dentist for every 721, 596 and 750 inhabitants, respectively (Table 3). The same applies, for example, in a more disparate fashion, in the city of Maringá where there is roughly 1 dental surgeon registered with the Federal Dental Council for every 366 inhabitants8-9. Besides the large number of dental surgeons in the marketplace today, we also have a large number of students graduating each year from the 191 dentistry faculties in the country8, with a great many of these looking to work in the public services. Bearing in mind the proportion recommended by the WHO of 1 dental surgeon per 1,500 inhabitants, the North and North-East regions are the ones that are still showing unfilled positions. On the other hand, the other regions demonstrate a saturation in the number of dental surgeons in the region. It is important to stress that these numbers reflect the average number of surgeons registered with the Federal Dentistry Council in a macro region and that each municipality may present specific situations. These numbers are alarming and provide support for considerations concerning the future of our profession, the direction of training and the future of dental schools. Other studies are needed so that they can adequately direct professionals towards qualification and help them to make an assertive choice with the aim of personal realization and professional success.
From the moment that the National Health System was institutionalized in the Federal Constitution of 1988, four items concerning its management have been frequently highlighted as fundamental for its implementation: decentralization, funding, social control and work management10. Of all of these, work management is the most complex and the one that has undergone the largest process of deregulation on the back of the reform policy of the State in the country. The lack of professional stimulus, the functional deviations, the double or even triple work shifts, where transgression of the law is the norm, are all commonplace, not to mention there is little or no opportunity for advancement provided by the employers9. Through this study, it can be seen that the positions offered by the city councils possess a broad salary band, the biggest difference being noted in the southeastern region, amounting to in excess of R$ 5,000 (Table 1). One possible explanation for this variance is the local conditions in the municipality. When we compare the Human Development Index (HDI) and the per capita Gross Domestic Product (GDP) of some of the municipalities, we also find discrepancies. Municipalities with the lowest salaries are: Umbuzeiro, Pernambuco (HDI = 0.539, GDP = R$ 1,928.43); Barra de Santa Rosa, Pernambuco (HDI = 0.575, GDP = R$ 2,031.69); and Nova Floresta, Pernambuco (HDI = 0.606, GDP = R$ 1,665.57). On the other hand, we see the highest salaries in the following municipalities10: Mogi das Cruzes, São Paulo (HDI = 0.776, GDP = R$ 7,236.53); Atibaia, São Paulo (HDI = 0.819, GDP = R$ 7,501.92); and Toledo, Paraná (HDI = 0.827, GDP = R$ 16,005.25). It is not abnormal for variances to occur, however the Salary Floor for the dental profession should be respected. Out of the 272 selective examinations evaluated, 174 (64%) offered a salary lower than the floor, i.e. three minimum salaries (R$ 1,050 as of 2006 and R$ 1,395 from 1 February, 2009, taking into consideration the Provisional Measure 456 of 30 January, 2009, which approved an increase in the minimum salary to R$ 465) for 20 working hours. According to the Union of Dental Surgeons, many municipalities do not respect these limits, as the established salary floor is only valid for the private sector. In the public sector, this floor is not established by law and each state or municipality is left to determine the value by means of a Bill in the Legislative Assembly11. In 1994, a Bill was proposed (Bill 4556/94) replacing Law 3999 of 15 December, 1961, amending the salary floor for dental surgeons to R$ 1,337.32. At this time, the bill is in the Chamber of Deputies ready to be voted upon in Plenary. However, as this project is limited to the alteration in the salary floor, it will continue to be restricted to the private sector. Accordingly, in order to guarantee that all professionals in this group are protected by this law, a new bill addressing both the private and public sectors is likely to be submitted. Certainly, the low salaries paid by some of the municipalities, as we have witnessed in this study, result in a lack of stimulus, motivation and commitment by professionals in the public system.
As regards the test questions, the most commonly found topic was 'Specific clinical knowledge', with an average of 46% of questions and a variance between 3% and 97%. This data agrees with the work of Gonçalo et al.12 which evaluated 16 selective examination tests for dental surgeons, noting that, on average, 48% of the questions in selective examinations for general practitioners focused on specific knowledge and 59.1% on Oral Health Teams. On the other hand, questions related to the National Health Service and Family Health Strategy showed a low prevalence both in the current study (8.1%) and in the study by Gonçalo (17.3% in selective examinations for general practitioners and 21.4% for Family Health Strategy). In spite of the fact that we noted, between 2006 and 2008, an increase in the percentage of questions about the National Health Service and Family Health Strategy, we still consider this to be a small number of questions on this topic in many tests, since these are average values and it can be seen that in some of the tests, there were no questions at all on this subject. In order to select professionals sufficiently trained for work in the National Health Service, it is essential to set tests in a manner commensurate with the desired candidate profile. In the past, many professionals graduated applying the model of the cure-based approach and this is still the case with some graduates to this day, focusing on procedure, specialties and so forth, not fully aware of what the National Health Service is, its breadth of coverage, how it functions and the main working strategy for improving the health of the population. Moreover, when selecting candidates, it is important that this is carried out by qualified institutions and includes the rating of specific titles in the area13.
By virtue of the diversity of selective examination questions, knowledge of the Portuguese language, IT, local knowledge, knowledge of the basic and clinical areas, the dental professional must be attuned to events occurring in our society, not just content acquired during undergraduate years, and be capable of exercising citizenship while exercising their profession.
Together with various other factors, the difficulty in leveraging the public health sector has also been related to the training of the professional to work in the public services. In the majority of schools, there exists a separation between the academic world and the world of health service provision. There is, at the present time, some concern over the reorientation of the academic training of health professionals so as to provide a broader vision and consequently offer to society professionals who are qualified to respond to the needs of the population and the functionality of the National Health Service. Through Inter-ministerial Directive 2101, jointly issued by the Ministry of Health and Ministry of Education, the National Program for the Reorientation of Professional Training in Health (PRÓ-SAÚDE) was launched on 3 November, 2005, encouraging the integration of the schools into the public health service in order to respond to the real needs of the Brazilian population in HR training, creation of knowledge and the provision of services directed towards strengthening the National Health Service13. The purpose of this initiative is to transform reality, based on the reorientation of the training of academics allied to appropriate interaction with public services and the community, with the aim of improving service quality, the satisfaction of professionals and users alike, and the management of the financial and human resources, so as to guarantee the sustainability of the SUS in terms of its universal and egalitarian policies.
CONCLUSION
Based on data collected from the examinations administered in 2006, it may be concluded that the number of dental surgeon vacancies for the Family Health Strategy was lower than the number of vacancies for working in the Basic Health Units, demonstrating that the family health strategy has still not become a priority in many municipalities.
The salaries paid by the majority of city councils did not reach, as a minimum, the salary floor established for the dental profession, which could generate demotivation of the professional working in the National Health Service, and working double or triple shifts.
It is fundamental for the selection of professionals trained to work in the National Health Service to set tests that are commensurate with the desired candidate profile.
Collaborators
SN MATSUMOTO and MS ENDO participated in the conception of the study, data analysis and composition of the article. RSS TERADA and LF LOLLI participated in the interpretation of data and the composition of the article. MF HAYACIBARA participated in the conception and design of the study, analysis and interpretation of data and the composition of the article.
REFERENCES
1. Lima APG. Os consórcios intermunicipais de saúde e o Sistema Único de Saúde. Cad Saúde Pública. 2000;16(4):985-96. doi: 10.1590/S0102-311X2000000400017. [ Links ]
2. Brasil, Constituição (1988). Constituição da República Federativa do Brasil. Brasília, DF: Senado Federal; 1988.
3. Viana ALD, Dal Poz MR. A reforma do sistema de saúde no Brasil e o Programa de Saúde da Família. Physis: Rev Saúde Coletiva. 1998;8(2):11-48.
4. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Programa Saúde da Família: ampliando a cobertura para consolidar a mudança do modelo de Atenção Básica. Rev Bras Saude Mater Infant. 2003;3(1):113- 25. doi: 10.1590/S1519-38292003000100013.
5. Brasil. Ministério da Saúde. Saúde da Família no Brasil: uma análise de indicadores selecionados 1998 -2004. Brasília: Ministério da Saúde; 2006.
6. Conselho Federal de Odontologia. Mais saúde bucal no Saúde da Família. J Cons Fed Odontol. 2006 Out 31; p. 20.
7. Conselho Federal de Odontologia. Mercado de trabalho. J Cons Fed Odontol. 2006 Out 31; Seção Destaque.
8. cfo.org.br [sítio na Internet]. Rio de Janeiro: Conselho Federal de Odontologia; c2009 [citado 2009 Ago 3]. Disponível em: <http://cfo.org.br/>.
9. IBGE. Contagem da população, 2007 [citado 2009 Fev 5]. Disponível em: <http://www.ibge.gov.br/home/estatistica/populacao/contagem2007/default.shtm>.
10. Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Princípios e diretrizes para a gestão do trabalho no SUS (NOB/ RH-SUS) [Internet]. 3ª ed. Brasília: Ministério da Saúde; 2005 [citado 2012 Mar 3]. Disponível em: <http://conselho.saude.gov.br/biblioteca/livros/nob_rh_2005.pdf>.
11. Federação Interestadual dos Odontologistas. Conheça seus direitos: legislação [citado 2009 Ago 3]. Disponível em: <http://www.fio.org.br/homefio.htm>.
12. Gonçalo CS, Vale RKS, Mialhe FL. Concursos públicos para a seleção do cirurgião dentista (CD): uma interferência negativa na consolidação do Sistema Único de Saúde (SUS)? Saúde Soc. 2008;17(supl. I):69.
13. Brasil. Ministério da Saúde. Programa Nacional de Reorientação da Formação Profissional em Saúde Pró-Saúde [citado 2009 Ago 3]. Disponível em: <http://www.prosaude.org>.
 Correspondence to:
Correspondence to:
MF FUJIMAKI
e-mail: mhayacibara@gmail.com
Received on: 26/8/2009
Final version resubmitted on: 21/11/2009
Approved on: 2/2/2010
