










 Inglés
Inglés




 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.2 Porto Alegre abr./jun. 2012
CLINICAL / CLÍNICO
Odontodisplasia regional
Amanda Silva de SOUSA I; Jorge Sá Elias NOGUEIRA I; Simone Lopes de MATTOS I; Sérgio de Melo ALVES JÚNIOR I
I Centro Universitário do Pará, Curso de Odontologia. Av. Nazaré, 630, Nazaré, 66040-143, Belém, PA, Brasil
ABSTRACT
The present article reports on a case of a dental development anomaly in an 18-month old patient whose parents sought treatment with the chief complaint of "missing teeth". The diagnosis of regional odontodysplasia or "ghost teeth" involving incisors and canine, both deciduous and permanent, of the upper right side of the mouth was based on radiographic features of the condition: marked reduction of enamel and dentin radiopacity, which are present in thin layers involving large pulp cavity of the teeth affected, usually belonging to a particular quadrant. At the age of three years and six months, the patient was still under observation, and received partial denture rehabilitation as a first step, since the clinical condition of the element 51 resulted in its extraction and the beginning of the child's school life required esthetic and functional rehabilitation. The other affected teeth were preserved, contributing to the alveolar development. The patient remains under regular follow-up and the treatment plan for the permanent dentition will depend on the degree of dental involvement.
Indexing terms: Odontodysplasia. Pediatric dentistry. Tooth deciduous. Tooth abnormalities.
RESUMO
O presente artigo relata um caso de anomalia de desenvolvimento dentário em paciente aos dezoito meses de idade, cujos pais buscaram atenção odontológica com a queixa de "falta de dentes". O diagnóstico de Odontodisplasia regional ou "dentes fantasma" envolvendo incisivos e canino, decíduos e permanentes, do quadrante superior direito foi baseado nas características radiográficas da condição: marcante redução na radiopacidade de esmalte e dentina, que se apresentam em finas camadas envolvendo ampla cavidade pulpar nos dentes afetados, geralmente pertencentes a um quadrante particular. Aos três anos e meio de idade, estando em controle periódico, a paciente recebeu prótese parcial removível como primeira medida reabilitadora, uma vez que a condição clínica do elemento 51 implicou sua perda, e o início da vida escolar da criança exigia reabilitação estética e funcional. Os demais dentes afetados foram conservados, contribuindo para o bom desenvolvimento alveolar. A paciente permanece em acompanhamento regular, sendo que o plano de tratamento para a dentição permanente dependerá do grau da anomalia em seus elementos.
Termos de indexação: Odontodisplasia. Odontopediatria. Dente decíduo. Anormalidades dentárias.
INTRODUCTION
On the list of dental anomalies, regional odontodysplasia represents a rare abnormality in development which affects all dental tissues, particularly the enamel and dentin. Its diagnosis is mainly established through the radiographic image known as "ghost teeth" on account of the marked reduction in the radiopacity of all the mineralized structures. The pulp chamber presents enlarged, and contoured by a thin layer of dentin and enamel with little contrast between these tissues1-2.
Clinically, the teeth involved in regional odontodysplasia may remain embedded or present delayed eruption, they may be hypocalcified, hypoplasic and stained. Histologically, there is a significant reduction in enamel and dentin, along with changes in orientation, density, size, shape and the distribution of the dentinal tubules. The pulp tissue contains loose or adhered calculus which may present tubules or consist of laminated calcifications3-4.
The pursuit of treatment involves either an acute condition, with pain and edema, developed via the degeneration of the pulp in the teeth involved4-13 or the absence of tooth eruption, which is linked to the paralysation of root formation1-2,14, with the deposit of a substance similar to cement on the enamel surface and with the absence of a continuous odontogenic epithelium around the crowns of the affected teeth10.
Vascular alterations during tooth development make up the theory most accepted in the etiology of regional odontodysplasia15. The number of teeth involved and the distribution pattern of this anomaly are variable, though it most commonly affects the contiguous teeth of the upper jaw, especially the incisors and canines, it being rare to see the involvement of more than two bone segments or the crossing of the midline2,8-9,11. If a deciduous tooth is involved in regional odontodysplasia, the successor is also probably affected, however permanent teeth with normal predecessors may exhibit the anomaly8,16.
In the oral rehabilitation of patients with regional odontodysplasia, the maintenance of the involved teeth depends on their clinical condition. Conservative options are desirable when the prognosis is favorable, as premature extraction of the affected teeth contributes adversely to the development of occlusion and the child's emotional state. Oral rehabilitation can involve endodontics, orthodontics, prosthetic restorations, autotransplantation and boneintegrated implants to improve function and esthetics2,12,17-19.
The present article reports on a clinical case of regional odontodysplasia in early childhood.
CASE REPORT
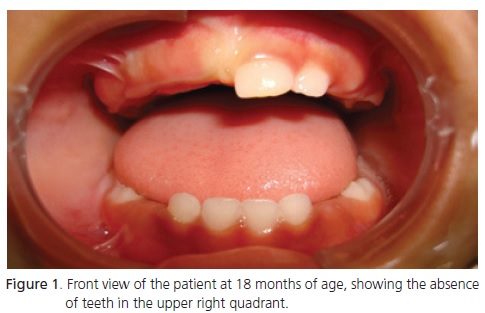
Female patient aged 18 months received treatment in the school clinic of a Dentistry Graduation Course in Belém, in the state of Pará. The main complaint reported by the mother was the non-emergence of some of the teeth. There were no significant data recorded in the medical records. The internal oral exam showed an asymmetry in the dental eruption in the upper arch with an absence of teeth in the right quadrant, as well as normal development of the dentition in the other regions, with the presence of the teeth expected for an individual of that age (Figure 1).
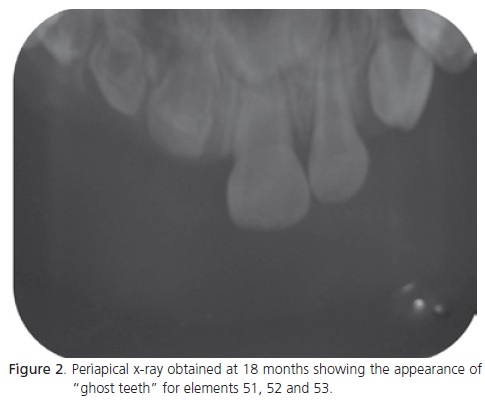
The x-ray showed the canine and upper incisors on the right side to be embedded, with a reduction in the radiopacity of the mineralized tissues and an ample pulp chamber (Figure 2).
The x-ray of the "ghost teeth", confirmed by a panoramic x-ray, permitted a diagnosis of regional odontodysplasia affecting teeth 51, 52 and 53, thus initiating the clinical observation of the case.
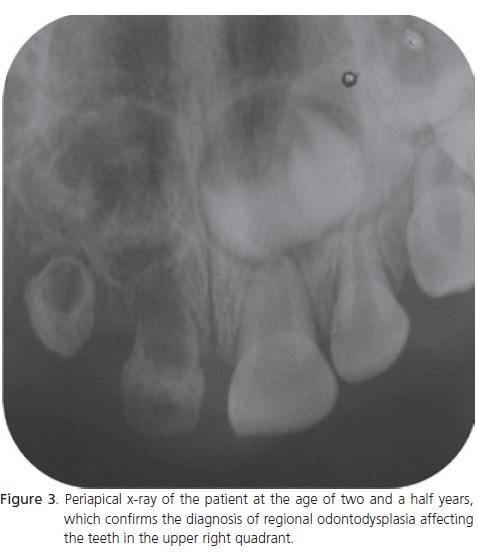
The patient returned to the dental clinic on reaching the age of two and a half. On this occasion, the internal oral exam showed the eruption of the right upper central incisor to be hypoplasic and the x-ray of the region affected by the regional odontodysplasia confirmed the presence of an anomaly in the permanent successors (Figure 3).
The patient returned again at three years of age, when the internal oral exam revealed the eruption of the right upper lateral incisor to be hypoplasic as well as the accentuated mobility of the right upper central incisor, which indicated it should be extracted. The histological examination of tooth 51 showed evidence of calcification in the pulp tissue and disorganized dentin (Figure 4).
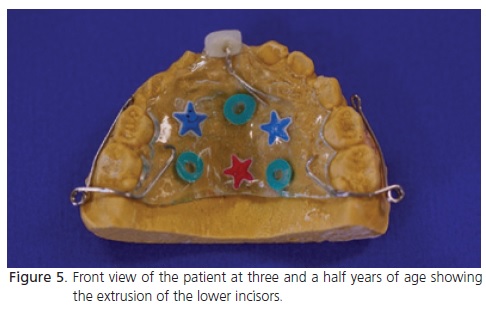
At a subsequent visit by the patient, now three and a half years old, the internal oral exam showed the eruption of the right upper canine and the extrusion of the lower incisors on the same side (Figure 5). So a functional and esthetic rehabilitation was planned using a partial, removable bridge and the preservation of teeth 52 and 53. The Free and Informed Consent Form was signed by the mother authorizing the treatment plan and the photographic documentation of the clinical case.
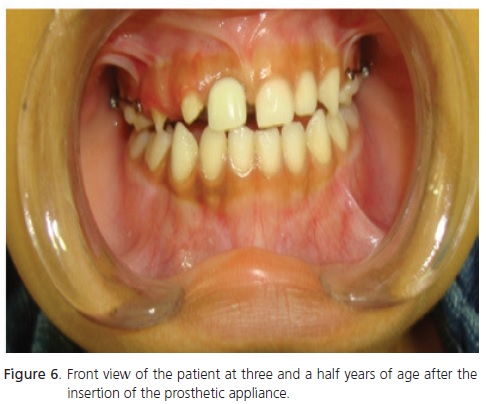
The dental bridge, constructed using stock teeth and a vestibular retainer, took well in the patient, who will remain under supervision during the development of the dentitions (Figure 6).

DISCUSSION
The present case has the characteristics most commonly observed in regional odontodysplasia, as far as prevalence and the clinical and histological characteristics of the anomaly are concerned. It attacks the front deciduous and permanent teeth of a quadrant in the upper arch in patients of the female sex. Other reports show less common presentations with regional odontodysplasia affecting more than one quadrant, crossing the midline or in non-adjacent quadrants4,18.
The radiographic characteristics, which include short roots, broad pulp chambers, wide apical foramens, marked reduction in enamel and dentin, present in this clinical case, confirm the "ghost teeth" diagnosis.
The histological analysis of tooth 51 showed the disorganization of the mineralized tissues and the presence of pulp calcification, which are frequent findings of this anomaly of dental development.
In this case, no local or systemic factor was identified as having the possibility of a connection with the regional odontodysplasia. This very observation has also been made by other authors4. On the other hand, there are reports of cases which associate regional odontodysplasia with vascular nevus in the area of the affected teeth, which supports the most accepted etiology for the anomaly, namely the alteration in the vascularization in the area15.
The teeth affected by regional odontodysplasia may exhibit various degrees of hypoplasia, which predisposes them to the development of caries, pulp pathologies and their after-effects. Accordingly, the diagnosis of the condition in the majority of cases is determined after having to seek urgent dental treatment. In this case, as in others that have been published, the search for dental care was occasioned by the clinical absence of the teeth13-14.
The scientific literature emphasizes the need for periodic monitoring of the development of dentitions in cases of regional odontodysplasia and stresses that decisions about therapy depend on the extent of the anomaly in each case. There has been one report published about the continuous formation of dentin in teeth affected by regional odontodysplasia, with a reduction in the pulp chamber and relative apical normalization, allowing the teeth to remain in the arch using esthetic and functional rehabilitation of the crown10. In the present case, treatment for the permanent denture cannot yet be predicted.
CONCLUSION
The dental professional who is dedicated to the treatment of children must be prepared to manage cases of dental anomalies, providing an opportunity for early diagnosis, adequate monitoring and treatment plans that minimize the after-effects on the patient's development. In cases of regional odontodysplasia, treatment depends on the extent of the involvement of the teeth and the individual functional and esthetic needs.
Collaborators
AS SOUSA contributed to the gathering of information for the review of the literature and the composition of the article. JSE NOGUEIRA was responsible for the dental treatment of the patient and the composition of the article. SL MATTOS contributed to the editing of the scientific article. SM ALVES JÚNIOR contributed to the histological analysis and composition of the article.
REFERENCES
1. Crawford PJ, Aldred MJ. Regional odontodysplasia: a bibliography. J Oral Pathol Med. 1989;18(5):251-63. [ Links ]
2. Yuan SH, Liu PR, Childers NK. An alternative restorative method for regional odontodysplasia: case report. Pediatr Dent. 1997;19(6):421-4.
3. Ribeiro AO, Dantas LP, Silva LCF. Odontodisplasia regional: relato de um caso clínico. Rev Port Estomatol Cir Maxilofac. 2008;49(3):159-63.
4. Carlos R, Contreras-Vidaurre E, Almeida OP, Silva KR, Abrahão PG, Miranda AMMA, et al. Regional odontodysplasia: morphological, ultrastructural, and immunohistochemical features of the affected teeth, connective tissue, and odontogenic remnants. J Dent Child. 2008;75(2):144-50.
5. Gomes MP, Modesto A, Cardoso AS, Hespanhol W. Regional odontodysplasia: report of a case involving two separate areas. J Dent Child. 1999;66(3):203-7.
6. Nicodemo RA, Moraes LC, Médici Filho E. Odontodisplasia regional: apresentação de um caso. Rev Paul Odontol. 1990;12(2):39-43.
7. Portela W, Coutinho TCL, Souza IPR, Costa MC, Soares DNS. Odontodisplasia regional: revisão de literatura e relato de caso clínico. Rev Bras Odontol. 1992;49(2):36-9.
8. Lowry L, Welbury RR, Soames JV. An unusual case of regional odontodysplasia. Int J Paediatr Dent. 1992;2(3):171-6.
9. Cabral LAG, Carvalho YR, Moraes E, Nogueira TO, Cavalcante ASR, Moares LC. Regional odontodysplasia: a report of three cases. Quintessence Int. 1994;25(2):141-5.
10. Gerlach RF, Jorge J, Almeida OP, Coletta RD, Zaia AA. Regional odontodysplasia: report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(3):308-13. doi: 10.1016/ S1079-2104(98)90014-2.
11. Chinn C, Kohli K. Regional odontodysplasia: a case report. N Y State Dent J. 2003;69(9):27-9.
12. Cahuana A, González Y, Palma C. Clinical management of regional odontodysplasia. Pediatr Dent. 2005;27(1):34-9.
13. Ferguson F, Schlissel E, Kucine A, Alexander S, DeSantis A, Hendricks R, et al. Long-term management of a child with regional odontodysplasia: a case report. Pediatr Dent. 2009;31(4):346-9.
14. Gondim JO, Pretel H, Ramalho LT, Santos-Pinto LA, Giro EM. Regional odontodyspalsia in early childhood: a clinical and histological study. J Indian Soc Pedod Prev Dent. 2009;27(3):175- 8. doi: 10.4103/0970-4388.57099.
15. Metha DN, Bailoor D, Patel B. Regional odontodysplasia. J Indian Soc Pedod Prev Dent. 2011;29(4):323-6. doi: 10.4103/0970- 4388.86380.
16. Quinderé LB, Cavalcante RB, Nonaka CFW, Miguel MCC, Souza LB. Regional odontodysplasia involving three quadrants of the jaws: a case report. Quintessence Int. 2010;41(1):13-6.
17. Gibbard PD, Lee KW, Winter GB. Odontodysplasia. Br Dent. J. 1973;135(12):525-32.
18. Melamed Y, Harnik J, Becker A, Shapira J. Conservative multidisciplinary treatment approach in an unusual odontodysplasia. J Dent Child. 1994;61(2):119-24.
19. Hamdan MA, Sawair FA, Rajab LD, Hamdan AM, Al-Omari LK. Regional odontodysplasia: a review of the literature and report of a case. Int J paediatr Dent. 2004;14(5):363-70. doi: 10.1111/j.1365-263X.2004.00548.x.
 Correspondence to:
Correspondence to:
AFL RIBEIRO
e-mail: arthurleal@gmail.com
Received on: 22/10/2010
Final version resubmitted on: 19/3/2011
Approved on: 26/7/2011
