










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.3 Porto Alegre Jul./Set. 2012
ORIGINAL / ORIGINAL
Social determinants and use of dental floss by 35-44-year-old adults
Determinantes sociais e o uso de fio dental por adultos de 35 a 44 anos de idade
Antônio Carlos FRIAS I; Alvaro Hiroyuki MYSUGUTI I; Thais Paragis SANCHEZ II; Gisele Lopes da Silva MANTOVANI II; Sônia Regina Cardim de Cerqueira PESTANA I
I Universidade de São Paulo, Faculdade de Odontologia. Av. Prof. Lineu Prestes, 2227, 05508-900, São Paulo, SP, Brasil
II Universidade de São Paulo, Fundação para o Desenvolvimento Tecnológico da Odontologia. São Paulo, SP, Brasil
ABSTRACT
Objective
To analyze social, economic and demographic variables associated with the use of dental floss by 35-44-year-old adults living in the district of Embu, 2008.
Methods
A cross-sectional type study in which an inquiry was applied and oral conditions were examined. The sample delineation was conglomeration probabilistic in two stages of random selection (censor sectors and eligible homes). The dependent variable was the use of dental floss in daily oral hygiene practices. The independent variables were social economic and demographic conditions, access to health services, habits and presence of caries and periodontal diseases. EPIINFO 06 and STATA 10 programs were used for Poisson regression analysis with adjustment for conglomeration sample.
Results
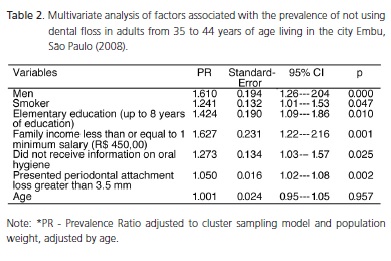
Of persons interviewed 52.1% stated that they did not use dental floss. In the multivariate model there was an association of non use of dental floss for men (PR=1,61 p=0,00), with those who declared having smoking habit (PR=1.24 p=0.04); with family income equal to or less than one minimum salary (PR=1.62 p=0.00); who had up to 8 years of schooling (PR=1.42 p=0.01); who did not receive information from the dentist about cleaning the teeth and gums (PR=1.27 p=0.02), and who presented severe periodontal diseases with clinical attachment loss >3.5mm (PR=1.05 p=0.00).
Conclusion
The research showed that the lack of dental floss use is a socially related behavior. Therefore, fair social policies is needed in order to minimize social inequalities, and ensure adult oral health educational programs.
Indexing terms: Adult. Dental devices, home care. Regression analysis. Socioeconomic factors.
RESUMO
Objetivo
Analisar as variáveis sócio econômicas e demográficas associadas ao uso do fio dental em adultos de 35 a 44 anos no município de Embu, 2008.
Métodos
Estudo do tipo transversal no qual foi aplicado um inquérito e realizado um exame das condições bucais. O delineamento da amostra foi probabilístico por conglomerado em dois estágios de sorteio (setores censitários e domicílios elegíveis). A variável dependente foi o uso do fio dental nas práticas diárias de higiene bucal. As variáveis independentes: condições sócio demográficas, sócio econômicas, acesso aos serviços, hábitos, presença de cárie dentária e doença periodontal. Empregou-se o programa EPIINFO 06 e o STATA 10, foi usado o modelo de regressão de Poisson com ajuste para amostragem complexas.
Resultados
A percentagem de pessoas relatando que não utilizavam o fio dental foi de 52,1%. No modelo de análise multivariável demonstrou que houve associação para o não uso do fio dental entre os homens (RP=1,61 p=0,00), que relataram o hábito de fumar (RP=1,24 p=0,04), com renda familiar menor ou igual a um salário mínimo (RP=1,62 p=0,00), que apresentavam até 8 anos de estudo (RP=1,42 p=0,01), que não receberam informação do cirurgião-dentista sobre higiene bucal (RP=1,27 p=0,02), e apresentam perda de inserção periodontal superior a 3,5mm (RP=1,05 p=0,00).
Conclusão
A pesquisa demonstrou que não usar o fio dental de maneira regular é um comportamento socialmente determinado, verifica-se a necessidade de elaboração de políticas socialmente mais justas que minimizem as iniquidades sociais, com ações de educação de saúde bucal voltadas para adultos.
Termos de indexação: Adulto. Dispositivos para o cuidado bucal domiciliar. Análise de regressão. Fatores socioeconômicos.
INTRODUCTION
According to epidemiological data on the adult population in the 35 to 44-year-old age group in Brazil in 2003, the prevalence of periodontal disease was 78.1% and mean number of teeth affected by dental caries identified by DMFT index = 20.1, with 65.7% of the index being composed of missing teeth, a fact representing a mean number of 13 teeth missing per adult1. These two diseases highly prevalent diseases are the leading cause of tooth loss in the population, leading to problems such as chewing, speech, and esthetic and socialization problems, factors accentuated by the difficulties economically and socially deprived individuals have in obtaining rehabilitation with dentures.
The determinant factors for the high incidence and prevalence of caries and periodontal disease are economic, social and educational conditions and not only biological factors that interact in their etiology. Inequality in caries experience and periodontal diseases are socially determined2.
Both caries and periodontal diseases are preventable and/or controllable diseases when proper oral hygiene is performed; there is control of sugar intake; systemic use of fluoride in the public water supply; regular use of toothpaste containing topical fluoride and access to oral health services is provided.
Oral hygiene practices such as brushing and flossing, when correctly performed daily are very important to prevent oral diseases, especially dental caries and periodontal disease. The habit of brushing teeth is one of the most effective ways to prevent caries and dental floss is the most indicated instrument to clean interdental spaces as it removes food residues and dislodges bacterial plaque, promoting oral hygiene and preventing caries and periodontal disease3-6.
The aim of this study was to analyze which of the demographic and socioeconomic variables are associated with the use of dental floss in adults between the ages of 35 to 44 years who live in the municipality of Embu, Brazil, 2008.
METHODS
The municipality
The municipality of Embu is located in the metropolitan area of São Paulo, SP, Brazil, with a population of 248,722 inhabitants and it occupies a land area of 70 km2. The Municipal Human Development Index (HDI) of the municipality is 0.772 and although it has a high level of wealth; the social indicators are not good. The illiteracy rate in the population over the age of 15 years in the city was 7.7% in 2000, while in São Paulo this rate was 6.6%, according to SEADE7. Moreover, the percentage of households with water supply network is 95.2%; sewage, 57.8%; and garbage collection serves 98.5% of households. Thus, the indicator of households with adequate internal urban infrastructure is 68.9%. In 2000, 17.6% of families had a per capita income of up to ½ minimum wage7.
Study
This was cross-sectional prevalence study based on statistical inference for population. A survey was used to identify oral hygiene habits, socioeconomic and demographic characteristics and to evaluate the conditions of caries and periodontal disease in adults between the ages of 35 and 44 years of age, residing in the municipality of Embu. The methodology used to examine the oral health conditions was that recommended by the World Health Organization, 4th edition8.
The sample was a two-stage cluster sampling design with random probability sampling: census sector and eligible household. In the first drawing stage 45 census sectors were drawn (Primary Sampling Unit - PSU), out of a total of 242 census sectors that comprised the municipality. In the second stage, the field sectors were grouped up and street sections with 10 households in each section were drawn (Secondary Sampling Unit - SSU), identifying eligible households in which it might possible to identify adults who were within the agerange of the research. Thus they were drawn according to adult/household crowding (3/1)9, for every three households drawn, it is possible to find one adult within the age-range.
To calculate the sample size the equation proposed by Lwanga & Lemeshow10 for the prevalence of caries and periodontal disease in infinite populations was used. The formula design effect (DEFF) was added, thereby adjusting the sample size for the two-stage cluster random sampling model. The non-reply rate was also included in the formula (NRR)11.
The fact that the sample was drawn in two stages, by cluster, with updating of the census sector size (number of households) in the grouping stage of the sector in the field sector, and drawing the street section with 10 homes, a difference was introduced in the probability of the adult belonging to sample drawn. The overall sampling fraction is multiplication of the random sampling fraction in the first and second stage [f = f1 * f2] and the sampling weight of the sampling plan was considered the inverse of the sampling fraction (w = 1/f)9. In addition to this resource, the design effect of the cluster design was taken into account in the statistical analysis process of the results.
Eight teams of examiners (dentists) and note takers (oral health assistants) were formed. Calibration was structured in two stages: a theoretical stage (8 hours) and a practical stage (32 hours). Calibration was carried out at a Basic Health Unit of the city of Embu. The Kappa coefficient was used to control reproducibility of observations and assessment of inter- and intra-examiner agreement of periodontal diseases, dental caries and implementation of the survey; in all, 64 subjects were examined and re-examined.
The aim of the calibration training was to ensure uniformity of interpretation, understanding and application of the criteria for the various conditions studied, ensure that each professional could perform the examination in a uniform and standardized way, and minimize variations among different examiners.
Ethical Considerations
The epidemiological survey followed the national and international research ethics guidelines involving human beings and it was approved by the Research Ethics Committee of the School of Dentistry, University of São Paulo, under protocol approval: 10/2008, March 31st 2008. After identifying the age groups of interest for the study in the households, the individuals were informed about the research and, after signing the term of free and informed consent, were interviewed and examined.
Data Collection
Data collection took place in June 2008. Previously, the Community Health Agents (CHA) of the areas covered by the Basic Health Units to which the census sector belonged visited the selected households and identified whether or not there was an adult within the age-range of the research. If there was, the adult was informed about the research and the date and time the residence would be visited by the team of examiners/note takers. During the visit, the adult would have all doubts clarified, and after signing the term of free and informed consent, the survey and examination would be carried out. The purpose of this previous visiting and scheduling procedure was to minimize the non-reply rate and to schedule a time when the adult of the household would be at home for the interview.
Appropriate places in the home with maximum use of natural light were chosen as the examination area. For examinations, 300 WHO CPI probes and 300 flat oral mirrors number 5 were used.
Variables
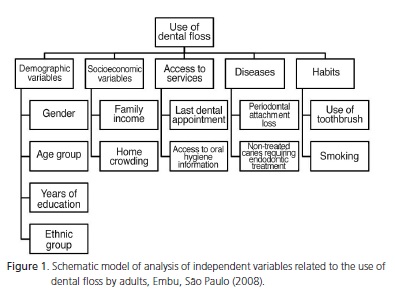
The dependent variable was the use of dental floss in the daily oral hygiene practice. The independent variables were: age group, sex, ethnicity, education, household crowding, family income, time of last appointment, access to oral hygiene information, periodontal attachment loss >3.5 mm, untreated caries requiring endodontic treatment, brushing habits, and whether the individual declared being a smoker.
The independent variables were categorized dichotomously. The sociodemographic variables were: age group (35-39 years/40-44 years of age); sex (male/ female); years of education (elementary/high school or higher); ethnicity (Afro-Brazilian and Mulatto/White). The socio-economic variables were: household crowding (1 or more persons per room/less than 1 person per room); family income (up to 1 minimum wage - R$450.00/more than 1 minimum wage). The access to services referred to: time of the last appointment (over 2 years/1 year or less); access to oral hygiene information (did not have access/had access). The diseases: periodontal attachment loss > 3.5 mm (present/absent); untreated caries requiring endodontic treatment (present/absent). The habits: use of toothbrush for oral hygiene every day (yes/no), smoker (yes/no).
Data analysis
For typing and verification of data, the EPIINFO 6 version 6.04, including the CSample module for bivariate data analysis from complex sampling designs, was used. The multivariate association of data was performed by STATA 10 using Poisson regression adjusted for cluster samples; the Taylor linearization adjusted for Primary Sampling Unit and population weight (weight) for twostage random sampling12. The selection of explanatory variables for the multivariate models used the criteria for biological plausibility and statistical adjustment.
The Figure 1 identifies the analysis model according to the outcome of adults that use dental floss in their daily oral hygiene practices and the variables in the model analyzed by the survey.
RESULTS
During the calibration process, the result of Kappa coefficient for inter-examiner agreement was 0.760 (0.713 to 0.806), a substantial agreement12, and the intra- examiner for Kappa coefficient was 0.935 (0.871 to 0.998). The indicators presented were considered adequate for the type of survey13-14. The non-reply rate was 9.5%.
A total of 345 adults between the ages of 35 and 44 years were interviewed. Of these, 240 (69.5%) were women; there were 214 (62.0%) individuals who identified themselves as Afro-Brazilians or Mulattoes; of the total number of respondents, 98.8% brushed their teeth regularly and every day and only 4 individuals reported that they did not brush their teeth; with regard to the use of dental floss, 180 (52.2%) individuals stated that they did not use it in their oral hygiene practice.
Of the variables identified in the analysis model, there was no statistically significant association when the habit of using dental floss was related to toothbrush use, and in relation to ethnic group and household crowding.
In Table 1, the results of the analysis of the variables in the bivariate model there was statistically significant association between the habit of using dental floss and the sociodemographic conditions. Men presented a higher prevalence of not using dental floss than women. The age group of 40 to 44 years of age used floss less than those in the 35 to 39-yearold age group. Those who reported being smokers used floss less than those who reported being non-smokers. Respondents who had a family income less than or equal to the minimum wage (R$ 450.00) used floss less than those who had a higher income. Those who had an unfavorable crowding condition of persons per room (one or more persons per room) used less floss than those with "less than one person per room."
There was also an association between individuals with low educational levels, individuals who had access to dental services two or more years ago, those who did not receive information on how to perform oral hygiene during the last dental appointment; with regard to diseases, those who had untreated caries in need of endodontic treatment and those with severe periodontal attachment loss >3.5 mm used floss less than those individuals who presented loss <3.5 mm or no loss.
The multivariable model adjusted for complex samples and population weight showed that there was association at a level of significance of 95% (Table 2). For the outcome of prevalence of not using dental floss, there was significant association for men who reported the smoking habit; those who had up to 8 years of education (elementary school); a household income less than or equal to the minimum wage; did not receive information from the dentist on how to clean their teeth and gums; had severe periodontal problems associated with severe periodontal attachment loss >3.5 mm. The final model was adjusted by age.

ANOVA statistical analysis followed by the Tukey test showed no statistically significant difference between the studied groups (p>0.05%).
Table 2 summarizes the average percentage of the obtained results. 100% of both studied microorganisms were eliminated when exposed in 0,25% peracetic acid. On the other hand, at 0,025% peracetic acid, 91.5% of the C. albicans strains and 68,65% of B. subtilis strains were eliminated.
DISCUSSION
Oral hygiene practices play an important role in the prevalence of oral diseases, particularly periodontal disease. Epidemiological studies have shown an association between oral hygiene and plaque; since there is substantial body of scientific evidence showing that periodontal diseases are associated with bacterial plaque15-16. However research conducted by Beirne et al.17 showed that there was no significant association between the amount of plaque and periodontal disease. Tooth brushing is the most common way to clean the teeth, being widely accepted by the population, as a desirable social behavior18. Furthermore, it has been recommended as the most practical and efficient way to prevent caries and periodontal disease.
The prevalence of individuals who do not use floss in their oral hygiene practice reflects an association with determinant factors of a biological, behavioral and socioeconomic order, as well as factors such as access to information and health services. This study identified the factors of association between the use of floss and socioeconomic variables (family income, household crowding), sociodemographic variables (gender, age group, education level, ethnic group), access to health services (the last dental appointment, access to oral hygiene information), diseases (periodontal attachment loss and untreated caries requiring endodontic treatment) and habits (smoking and use of toothbrush).
According to Silva et al.19, the appropriate use of dental floss is of fundamental importance for the good maintenance of oral health. In a study conducted among patients of a dental clinic at a university in Rio de Janeiro it was observed that 54% of patients showed the inability to use floss, in spite of having completed the proposed dental treatment. This study indicates that even when individuals have access to the oral health services, this does not guarantee that they will have access to information relative to the proper use of dental floss. As regards the adults in Embu, less than half (47.8%) of those who were interviewed used dental floss.
A study conducted by Araujo et al.20 observed that among college interviewees, 28% of them did not use floss or did not use it regularly; 21% said they had not received any information regarding its use; and of those who did obtain information, 20% had access through their parents, friends or on television programs. Even among the college students, the use of floss was not a regular practice and access to information was also limited and not appropriate.
According to the studies of Gift21, the regular use of dental floss is not a common habit for most of the population in industrialized countries, and only a limited number of people use it regularly.
Abegg22 in a research conducted with adults in the city of Porto Alegre, found no statistically significant differences with regard to gender, thus differing from the results of this study (Table 1 and 2), in which both in the bivariate model (PR = 2.09) and in the multivariate model (PR = 1.61) showed that women use floss more than men. This difference was statistically significant even when this variable was associated with other variables. These results reinforce the situation observed both in practice and in the literature: that these preventive habits are more common among women than men.
The socioeconomic conditions showed a series of influences on people's living conditions. These may reflect the habits and individual and family behaviors and point out the difficulty of access to oral hygiene products. With regard to the use of dental floss, one of the factors that reduces its regular use is the economic factor, since it is expensive and only affordable by a small portion of the population20-21.
A study conducted on the cost of oral hygiene products (toothpaste, toothbrushes and dental tape/floss) available in the supermarkets in the city of Cascavel in 2004 and 2006 showed that the average monthly expense per individual to purchase oral care products ranged from R$ 7.25 to R$8.66, with 61% of this cost related to the cost of dental floss23. In this study it was found that the socio-economic reality influences the use of floss because there is a lower prevalence of use among adults with a family income of up to one minimum wage (PR = 1.62) than among those with a higher family income, and it may be related primarily to its acquisition, making it unfeasible to use floss on a regular and continuous basis.
The fact that individuals declare they smoke and do not use dental floss may be a marker of negligence of their own health; alternatively, these individuals have a low level of education and have no access to information on how to maintain their oral health. The lack of access to oral health information, the habit of smoking and low level of education are variables correlated to one another and present a statistically significant association with the outcome, thus not using floss may indicate a lack of adequate information on how to maintain good habits to ensure health.
Studies have pointed out that even in low-income communities where oral health education activities have emphasized the need to remove bacterial plaque, positive results have been shown, according to a study conducted by Petry et al.24 One of the factors that hinder access to information in developing countries is access to public health services, emphasizing that access to information is a key factor for changing less favorable oral conditions and incorporating healthy habits25.
In an assessment of the effects of education and motivation with respect to knowledge and oral hygiene behavior in adults, a study conducted by Garcia et al.26 showed that after an educational program on oral hygiene behavior, more than half of the patients (74%) used dental floss appropriately, whereas before participating in the health education activity, only 36% used dental floss.
Fairer social policies minimize social inequalities. Ensuring educational programs focused on oral health for adults, particularly in lower-income communities, with regular and continuous distribution of oral hygiene products such as toothbrushes, toothpaste and dental floss, are all health actions with locoregional organization. Providing training for oral health education activities, not only to the dental staff of Basic Health Units, but also to Community Health Agents of the Family Health Program is a way of increasing and universalizing oral health education practices particularly with the use of teaching strategies appropriate for adults. According to Carvalho et al.27, the purpose of developing specific oral health programs for adults is to modify the current epidemiological scenario.
CONCLUSION
This research showed that among adults in the age-range between 35 and 44 years, who live in the municipality of Embu, the use of floss is less frequent and statistically significant in men who reported smoking; who had less than eight years of education; a family income less than or equal to the minimum wage; periodontal attachment loss >3.5 mm and had no access to o oral hygiene information from a dental appointment. These were determinant factors for the non use of dental floss in the daily oral hygiene practice of this group, and the results show that this behavior is socially determined.
Collaborators
AC FRIAS participated in the organization of the research, statistical analysis and writing of the article. GLS MANTOVANI participated in the field activity and writing of the article. AH MYSUGUTI, TP SANCHEZ, SRCC PESTANA participated in the literature review and writing the article.
REFERENCES
1. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Projeto SB Brasil 2003: condições de saúde bucal da população brasileira 2002-2003. Resultados principais. Brasília: Ministério da Saúde; 2004 [citado 2010 Ago 25]. Disponível em: < http://dtr2001.saude.gov.br/editora/produtos/livros/pdf/05_0053_M.pdf > [ Links ].
2. Bastos JL, Antunes JLF, Frias AC, Souza MLR, Peres KG, Peres MA. Color/race inequalities in oral health among Brazilian adolescents. 2009, Rev Bras Epidemiol. 2009;12(3):313-24. doi: 10.1590/S1415-790X2009000300003.
3. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cárie dentária no Brasil: declínio, iniqüidade e exclusão social. Rev Panam Salud Publica. 2006;19(6):385-93. doi: 10.1590/S1415- 790X2009000300003.
4. Loesche WJ. Cárie dental: uma infecção tratável. Rio de Janeiro: Cultura Médica; 1993.
5. Lisboa IC, Abegg C. Hábitos de higiene bucal e uso de serviços odontológicos por adolescentes e adultos do Município de Canoas, Estado do Rio Grande do Sul, Brasil. Epidemiol Serv Saúde. 2006;15(4):29-39. doi: 10.5123/S1679- 49742006000400004.
6. Chiapinotto GA, Meller D, Santos FB. Avaliação de meios mecânicos de limpeza. RGO - Rev Gaúcha Odontol. 2001;49(3):161-4.
7. Fundação Sistema Estadual de Análise de Dados. Perfil municipal [citado 2010 Ago 25]. Disponível em: <http://www.seade.gov.br/produtos/perfil/perfil.php>.
8. World Health Organization. Oral health surveys: basic methods. 4th. ed. Geneva: WHO; 1997.
9. Sousa MH, Silva NN. Estimativas obtidas de um levantamento complexo. Rev Saúde Pública. 2003;37(5):622-70. doi: 10.1590/ S0034-89102003000500018.
10. Lwanga SK, Lemeshow S. Sample size determination in health studies: a pratical manual. Geneva: World Health Organization; 1991.
11. Silva NN. Amostragem probabilística. São Paulo: Edusp; 1998.
12. Alves MCGP, Silva NN. Métodos de estimação de variância em amostras provenientes de inquéritos domiciliares. Rev Saúde Pública. 2007;51(6):938-46.
13. Landis JR, Kock GG. The measurement of observer agreement for categorical date. Biometrics. 1977;33(1):159-74.
14. Frias AC, Antunes JLF, Narvai PC. Precisão e validade de levantamentos epidemiológicos em saúde bucal: cárie dentária na Cidade de São Paulo, 2002. Rev Bras Epidemiol. 2004;7(2):144-54. doi: 10.1590/S1415-790X2004000200004.
15. Fischer RG. Controle mecânico e químico do biofilme dental. In: Tunes UR, Rapp GE. Atualização em Periodontia e Implantodologia. São Paulo: Artes Medicas; 1999.
16. Almeida JCS, Couto GBL, Gusmão ES. Escovação no controle da placa, avaliação do ensino e motivação em escolares. RGO - Rev Gaúcha Odontol. 2001;49(3):127-32.
17. Beirne PV, Worthington HV, Clarkson JE. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2005;(1):CD004625.
18. Levine R. The scientific basis of dental health education. 3rd ed. London: Health Education Authority; 1991.
19. Silva ACC, Santiago FC, Souza IPR. Avaliação da habilidade do uso do fio dental em adolescentes. Rev Bras Odontol. 2002;59(5):296-8.
20. Araújo CA, Deliberador T, Cruz ACC. O uso de fio dental por universitários. JBC J Bras Clin Odontol Integr. 2003;7(42):467- 71.
21. Gift HC. Current utilization patterns of oral hygiene practices: state-of-the-science review. In: Löe H, Kleinman DV. Dental plaque control measures and oral hygiene practices. Oxford: IRL; 1986. p. 39-71.
22. Abegg C. Hábitos de higiene bucal de adultos porto-alegrenses. Rev Saúde Publica. 1997;31(6):586-93. doi: 10.1590/S0034- 89101997000700007.
23. Santos LF, Hirata E, Mialhe FL, Silva DD, Silva RP. Custo da higienização bucal no município de Cascavel - PR. Rev Fac Odontol. 2008;13(2):12-6.
24. Petry PC, Victoria CG, Santos IS. Adultos livres de carie: estudo de casos e controles sobre conhecimentos, atitudes e práticas preventivas. Cad Saúde Publica. 2000;16(1):145-53. doi: 10.1590/S0102-311X200000010001.
25. Cordon JA, Garrafa V. Prevenção versus preventivismo. Divulg Saúde Debate. 1991;6:10-6.
26. Garcia P, Petromilli NS, Campos FP, Rodrigues JA, Santos PA, Dovigo LN. Avaliação dos efeitos da educação e motivação sobre o conhecimento e comportamento de higiene bucal em adultos. Ciênc Odont Bras. 2004;7(3):30-9.
27. Carvalho ES, Bastos RS, Rodrigues ADM, Melo WM, Lauris JRP, Bastos JRM, et al. Epidemiologia das doenças bucais em indivíduos na faixa etária entre 35 e 44 anos: o cenário epidemiológico do trabalhador. RGO - Rev Gaúcha Odontol. 2010;58(1):109-14.
 Correspondence to:
Correspondence to:
AC FRIAS
e-mail: acfrias@usp.br
Received on: 5/5/2010
Final version resubmitted on: 30/8/2010
Approved on: 9/9/2010
