










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.3 Porto Alegre Jul./Set. 2012
ORIGINAL / ORIGINAL
Prevalence and associated factors of malocclusion in the primary dentition
Prevalência e fatores associados à maloclusão na dentição decídua
Juliana Mariano MASSUIA I; Wladithe Organ CARVALHO II
I Universidade Estadual de Londrina, Faculdade de Odontologia. Rua Pernambuco, 540, Centro, 86020-070, Londrina, PR, Brasil
II Universidade Estadual de Londrina, Departamento de Saúde Coletiva. Londrina, PR, Brasil
ABSTRACT
Objective
To estimate the prevalence and factors associated with malocclusion in primary dentition.
Methods
A cross-sectional study consisting of all children living in areas covered by the Family Health Units in the municipality of Pedra Preta - Mato Grosso. Data collection consisted of two steps: an interview with the mother and / or guardian and the child's clinical dental examination. The interviews were conducted by two previously trained assistants and clinical examination by a dentist previously trained and calibrated (intrarater kappa = 0.96). A total of 374 children aged three to five years were examined. Criteria for classifying normal occlusions and malocclusions were: terminal relationship primary second molars, canine relationship, transverse relationship, goodwill and presence / absence of crowding.
Results
Was used the Poisson regression. The prevalence of malocclusion was 53.2% (95% CI: 48.3, 58.6). An association of malocclusion with the following variables: presence of oral habits, exclusive breastfeeding ≤ 3 months, facial profile of the type / concave and convex arc-shaped jaw V.
Conclusion
The prevalence of malocclusion in primary dentition was high, however some are associated with avoidable factors: early diagnosis and preventative measures can prevent and / or intercept the establishment of these changes, even in the primary dentition.
Indexing terms: Breast feeding. Dentition primary. Habits. Malocclusion.
RESUMO
Objetivo
Estimar a prevalência e fatores associados à maloclusão na dentição decídua.
Métodos
Estudo transversal constituído pelo total de crianças residentes nas áreas de abrangência das Unidades de Saúde da Família do município de Pedra Preta, Mato Grosso. A coleta de dados foi composta por duas etapas: entrevista com a mãe e/ou responsável e exame clínico odontológico da criança. As entrevistas foram realizadas por duas auxiliares previamente treinadas e o exame clínico por um cirurgião dentista previamente treinado e calibrado (Kappa intraexaminador: 0,96). Foram examinadas 374 crianças na faixa etária de 3 à 5 anos. Os critérios para classificar as oclusões normais e maloclusões foram: relação terminal dos segundos molares decíduos, relação de caninos, relação transversal, trespasses e presença/ausência de apinhamento.
Resultados
Utilizou-se a Regressão de Poisson. A prevalência de maloclusão foi de 53,2% (IC 95%: 48,3; 58,6). Verificou-se associação de maloclusão com as seguintes variáveis: presença de hábitos bucais, aleitamento materno exclusivo ≤ 3 meses, perfil facial do tipo côncavo/convexo e arco maxilar em forma de V.
Conclusão
A prevalência de maloclusão na dentição decídua foi elevada, entretanto alguns fatores associados são evitáveis: o diagnóstico precoce e medidas preventivas podem impedir e/ou interceptar o estabelecimento destas alterações, ainda, na dentição decídua.
Termos de indexação: Aleitamento materno. Dentição primária. Hábitos. Má oclusão.
INTRODUCTION
Malocclusion is a developmental anomaly of teeth and/or dental arches that may occur in both primary and permanent dentition, which causes esthetic discomfort in milder cases and functional damage and disability in more severe cases1. It is usually caused by the interaction of hereditary, congenital and acquired factors of a general or local order, and due to the presence of oral habits2.
Due to the high prevalence of malocclusion, the World Health Organization (WHO) considers it one of the major dental public health problems worldwide3. More importantly, it is possible to prevent and treat this alteration, which may cause a negative social impact by interfering with quality of life of the individuals affected, harming their social interaction and psychological wellbeing4-5. The reduction in the incidence of dental caries in children and adolescents over the last few decades has drawn more attention to other oral problems such as malocclusions5. Due to this, it is important to clearly define the factors associated with this condition in order to facilitate the planning of prevention and care actions.
The study of malocclusions and their etiology is of fundamental importance to dentists who can prevent and/ or intercept problems that are difficult to solve in the long term through early diagnosis and preventive measures, and by increasing patients and/or guardians' awareness of the problem6.
By identifying the prevalence and factors associated with malocclusion in primary dentition, this study is justified due to need of the public sector to obtain action parameters to prevent this condition, with the formulation of programs that include measures to prevent and intercept occlusal disorders in the initial period of orofacial development.
METHODS
The municipality
This is a cross-sectional study whose population consisted of children resident in the coverage area of Family Health Units (FHU) in the municipality of Pedra Preta - Mato Grosso. The city has 16,461 inhabitants7, three Family Health Units and three Family Health Program teams (FHP). The proportion of the population covered by the Family Health Program in 2009 was 73% with 3,720 families enrolled in the Primary Care Information System (Sistema de Informação da Atenção Básica - SIAB), totaling 12,015 people8. All families registered in the Primary Care Information System with children between the ages of 3 and 5 years were selected by community health agents (CHA) and the initial population was composed of 432 children.
The following exclusion criteria were adopted: children with permanent teeth, partially or fully erupted (mixed dentition); children with one or more teeth with extensive caries lesion (remnant of clinical crown limited to the gingival third), and children who have undergone or are undergoing orthodontic treatment.
Drop-outs were considered when the children refused to participate or their parents/guardians did not provide authorization; those who were not found at home after three attempts at different times; and those whose addresses were not found or were inexistent.
Data collection was performed in two stages: home interview with the mother and/or guardian; clinical dental examination conducted at school or day-care center or at home (for those children who did not attend school).
For the home interview, the residence was found using the address registered in the A Record of the Primary Care Information System. The clinical exam of occlusion was performed on another day by a dentist, previously trained and calibrated (intrarater Kappa: 0.96).
The children were evaluated during classes, seated on a school chair, in front of the examiner, in a room with natural light. When the examination was performed at home, the child remained seated on a chair. The oral exam was performed with aid of a disposable wooden spatula, black pencil No 2 and millimeter ruler. All information was noted on an individual clinical chart.
The morphological aspects of the children's occlusion were evaluated according to the classification of Baume9 for the anteroposterior relationship of the second deciduous molars, and Foster & Hamilton10 for the deciduous canine relationship. The following characteristics were also analyzed: horizontal overlap, vertical overlap, tooth crowding/spacing, anterior open bite, complete crossbite, unilateral or bilateral anterior and posterior crossbite. According to these conditions, occlusion was classified as normal or as malocclusion.
Occlusion was classified as normal when habitual maximum intercuspation of the child had the following characteristics: terminal plane relationship of second deciduous molars in a straight and/or mesial plan with canine in Class I; absence of crossbite and/or open bite; normal overjet and overbite; positive measurements up to 2 mm. The outcome of the study was the presence of malocclusion. The independent variables analyzed were: sex, age, type of birth, prenatal, respiratory disease diagnosed by a physician, dental appointment, sleep disorders, duration of exclusive breastfeeding, presence of oral habits and clinical aspects.
After performing the epidemiological survey, the data were digitized using the EPI INFO 3.3.2 software. The associations between the exposure and outcome variables were assessed at a level of significance of 95% by the Chisquare test (X2) and the Fisher's Exact test, when necessary, due to the reduced number of cases in an analysis category. The variables that presented a value of p < 0.20 by the X² test were pre-selected to compose the Poisson regression model. The multivariate analyses were performed by the Stata 8.0 program.
The study was approved by the Ethics Committee on Research in Human Beings of the Federal University of Londrina, in accordance with resolution No 196/6, in report No 252/08. For this purpose authorization of the local health authority was requested, and the children's legal guardians signed a term of free and informed consent authorizing the procedures to be performed in the children and their participation in the study.
RESULTS
Data collection occurred between April and June 2009. According to the census conducted, the list initially obtained contained 432 children, however, 33 (7.6%) were excluded during the research process: 10 had moved away from the coverage area of the Family Health Units, 6 had extensive caries with clinical crown remnant limited to the gingival third and 17 had mixed dentition. The non-reply rate was 5.8%, in which: eight children were not found after three visits or the address was not found, six guardians were unable to provide accurate information, five mothers/guardians refused participation, and six children refused to participate in the clinical examination.
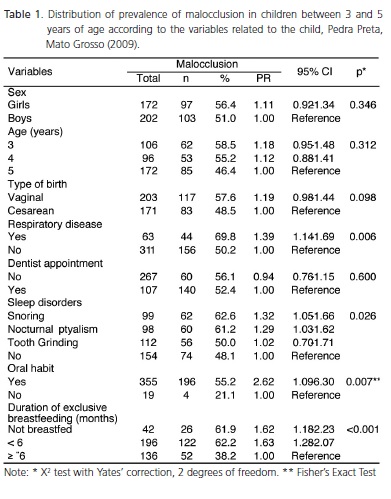
The mean age of the children was 4.2 years of age (±0.8 years) with a larger number of boys within the age group of 5 years (Table 1).
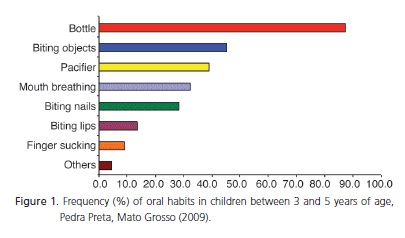
Mean time of exclusive breastfeeding (EMB) was 4.41 months and the mode was 6 months. The prevalence of one or more oral habits in children was 94.9% (95% CI: 92.0; 96.8). The most common oral habit was use of the feeding bottle (87.2%; 95% CI: 83.3; 90.4), followed by biting objects (45.2%; 95% CI: 40.1; 50.4) and use of a pacifier (39%; 95% CI: 34.1; 44.2), as shown in Figure 1.
Only 5.1% (95% CI: 3.2; 8.0) of the children did not present any type of oral habit. Of these children, 78.9% had normal occlusion and all received exclusive breastfeeding for three months or longer.
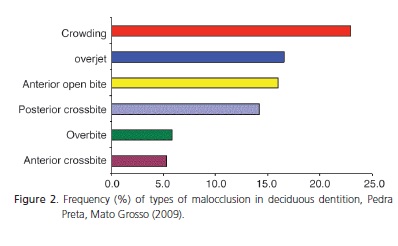
The prevalence of malocclusion was 53.2% (95% CI: 48.3; 58.6) and some types of malocclusion were concomitant. The most frequent types were crowding (23.0%; CI 95%: 18.9; 27.7) overjet (16.6%; 95% CI: 13.0; 20.8) and anterior open bite (16.0%; 95% CI: 12.6; 20.2), as shown in Figure 2.
With regard to the terminal plane relationship of the second deciduous molars, the highest frequency found was for the group with mesial step (47.1%) followed by the straight plane (43%) and distal step (4.8%). Approximately 5% of children presented an asymmetrical (left-right) molar relationship. The most prevalent canine relationship was Class I (76.5%), followed by Class II (14.7%) and Class III (8.8%).
The children's characteristics that were significantly associated (p<0.05) with malocclusion were as follows: physician-diagnosed respiratory disease, sleep disorders, ptyalism and/or snoring, presence of one or more oral habits and the fact that the child did not receive exclusive breastfeeding or to have been breastfed for less than six months (Table 1).
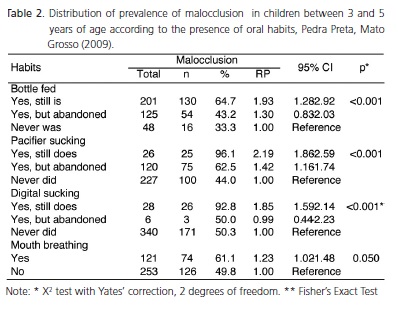
A significant relationship was found between malocclusion and the following habits: bottlefeeding, pacifier and finger sucking habits and mouth breathing (Table 2). For the variables bottle-feeding and finger sucking habits, the fact that the child did not abandon the habit, was why it was associated with malocclusion.
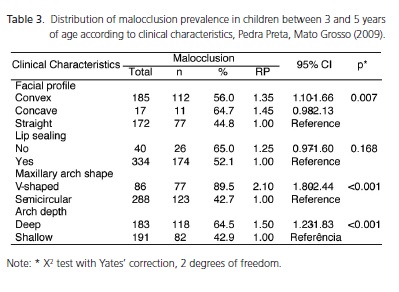
Considering the clinical aspects evaluated in the children, the convex facial profile, and the V-shaped and deep maxillary arch were significantly associated with malocclusion (Table 3).
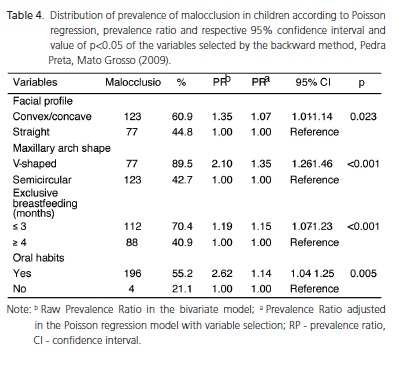
By the multivariate analysis, in the Poisson regression, it was found that the categories with negative association with malocclusion were as follows: the concave+convex facial profile in comparison with the straight profile, the V-shaped maxillary arch in comparison with the semicircular arch, and exclusive breastfeeding for ≤ 3 months ≥ in comparison with 4 months, and the presence of one or more oral habits in comparison with the absence of habits (Table 4).
DISCUSSION
Some studies conducted in Brazil have pointed out the high prevalence of malocclusions in the child population during the deciduous dentition period with values higher than 70%11-12. However, other studies have shown a similar tendency to the one found in the present study in which approximately 50% (95% CI: 48.3; 58.6) of the sample presented some type of malocclusion13-15.
The most frequent type of malocclusion reported in the literature is anterior open bite16-19. In the studied population, crowding, overjet and anterior open bite showed estimates per overlapping intervals, although the point estimate of crowding was higher. One supposes that this finding resulted from the following fact: the majority of children in this study never had some of the habits that have been established in the literature, such as those associated with anterior open bite - pacifier use and finger sucking; and the majority of children who previously had these habits, had abandoned them by the time of data collection (> 90%).
Although different methods are reported in the literature, the distribution of sagittal relationship in this study population is in agreement with some studies that have highlighted the predominance of mesial step, followed by the straight plane and distal step. However, the majority of studies in the existent literature show a greater prevalence of the straight terminal plane9,10,20-22. The prevalence of 8.8% of the relationship between canines in Class III shown in this study was higher than that found in the studies of Farsi & Salama22 - 3.3%, and Foster & Hamilton10. These differences might be due to the variations in the application of the methodology and also ethnicity, since Brazil is a country marked by miscegenation.
Many studies have shown an association between the presence of malocclusion and oral habits11-18,23-25, type of (breast/bottle) feeding13,16,23-25 and mouth breathing14,25. These associations were confirmed in the present study, in which the pacifier, predominantly mouth breathing, and current use of bottle and finger sucking were significantly associated with the presence of malocclusion.
In the literature, pacifiers have been reported as the predominant oral habit among children13, however, in the present study, the most frequent habit was the use of the feeding bottle, which is in agreement with the studies of Silva Filho et al.12. This datum draws attention to the fact that the pacifier has been offered to children less frequently, due to campaigns and/or awareness among parents; nevertheless, it clearly demonstrates that the problem related to the use of the feeding bottle persists and needs to be addressed.
The duration of breast/bottle feeding has a strong influence on the development of oral habits6,13,24. Considering the data shown in this study, it can be affirmed that exclusive breastfeeding for a period equal to or longer than six months has a positive influence, as a way to prevent the use of bottles and pacifiers, and the development of malocclusions.
The results confirm a high number of children who were exclusively breastfed, with an average of 4.41 months of breastfeeding, therefore, suggesting that the studied population received this protective effect of breastfeeding against oral habits and malocclusions.
Viggiano et al.23 observed the protective effect of breastfeeding on the development of posterior crossbite in deciduous dentition. Furtado and Vedovelho Filho24 also found that the duration of breastfeeding influenced the presence of malocclusion, because children who were breastfed for a longer period showed reduced frequency of malocclusion, corroborating the data obtained in this study.
The majority of studies on the prevalence of malocclusion in deciduous dentition refer to research conducted among schoolchildren11-15,17,19,21 and there are few population-based studies. The design of this study is outstanding because it included all the children living in areas covered by FHU in a small municipality. These data are therefore important for organizing dental services in similar communities that represent the majority of the type of which the country is composed. The present study was designed to provide data of prevalence and factors associated with malocclusion in the child population of a community. The data, however, show the dimension of the problem and the need for further longitudinal studies that deepen the understanding of the subject. This is required in order to provide better support for prevention strategies against factors associated with the development of malocclusions, which are controllable, in addition to obtaining assistance for this vulnerable population from the public sector.
CONCLUSION
The prevalence of malocclusion in children living in areas covered by the FHU in the municipality of Pedra Preta (MT) was high (53.2%) and the factors that were associated with malocclusion, using Poisson regression, were shown to be: presence of oral habits, exclusive breastfeeding ≤ 3 months, convex/concave facial profile and V-shaped maxillary arch.
Collaborators
JM MASSUIA participated in the literature review, developed the initial research, collected the data, interviewed the parents/guardians of the children, conducted dental examinations of all children, digitized the database, organized the statistical analysis of the results and wrote the article. WO CARVALHO participated in the literature review, reviewed the article, prepared the tables and figures, checked the database, organized the statistical analysis of the results and wrote the article.
REFERENCES
1. Almeida RR, Almeida Pedrin RR, Almeida MR, Garib DG, Almeida PCMR, Pinzan A. Etiologia das más oclusões-causas hereditárias e congênitas adquiridas gerais, locais e proximais (hábitos bucais). Rev Dent Press Ortodon Ortop Facial. 2000;5(6):107-29. [ Links ]
2. Moyers RE. Etiologia da maloclusão. In: Moyers RE. Ortodontia. 4ª ed. Rio de Janeiro: Guanabara Koogan; 1991. p. 156-66.
3. World Health Organization. What is the burden of oral disease? Geneva, 2010 (cited 2010 Jan 5). Available from: <http://www.who.int/oral_health/disease_burden/global/en/>.
4. Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004;31(1):20-7. doi: 10.1179/146531204225011364.
5. Peres KG, Traebert ESA, Mercenes W. Diferenças entre autopercepção e critérios normativos na identificação das oclusopatias. Rev Saúde Publica. 2002;36(2):230-6. doi: 10.1590/S0034-89102002000200016.
6. Leite ISG, Rodrigues CC, Faria AR, Medeiros GV, Pires LA. Associação entre aleitamento materno e hábitos de sucção não nutritivos. Rev Assoc Paul Cirur Dent. 1999;53(2):151-6. doi: 10.1590/S1413-81232011000500017.
7. Instituto Brasileiro de Geografia e Estatística. Cidades@ [citado 2010 Jan 12]. Disponível em: <http://www.ibge.gov.br/cidadesat/topwindow.htm?1>.
8. Brasil. Ministério da Saúde. Sistema de Informação de Atenção Básica. Cadastramento familiar - Mato Grosso [citado 2009 Jan 12]. Disponível em: <http://tabnet.datasus.gov.br/cgi/tabcgi.exe?siab/cnv/siabfMT.def>.
9. Baume LJ. Physiological tooth migration and its significance for the development of oclusion: I. The biogenetic course of the deciduous dentition. J Dent Res. 1950;29(2):123-30. doi: 10.1177/00220345500290020301.
10. Foster TD, Hamilton MC. Occlusion in the primary dentition. Br Dent J. 1969;126(2):76-9.
11. Leite Cavalcanti A, Medeiros Bezerra PK, Moura C. Breastfeeding, bottle-feeding, sucking habits and malocclusion in Brazilian preschool children. Rev Salud Pública. 2007;9(2):194- 204. doi: 10.1590/S0124-00642007000200004.
12. Silva Filho OG, Cavassan AO, Rego MVNN, Silva PRB. Hábitos de sucção e má oclusão: epidemiologia na dentadura decídua. Rev Clín Ortodontia Dental Press. 2003;2(5):57-74.
13. Gimenez CMM, Moraes ABA, Bertoz AP, Bertoz FA, Ambrozano GB. Prevalência de más oclusões na primeira infância e sua relação com as formas de aleitamento e hábitos infantis. Rev Dent Press Ortodon Ortop Facial. 2008;13(2):70-83. doi: 10.1590/S1415-54192008000200009.
14. Emmerich A, Fonseca L, Elias AM, Medeiros, UV. Relação entre hábitos bucais, alterações oronasofaringianas e maloclusões em pré-escolares de Vitória, Espírito Santo, Brasil. Cad Saúde Pública. 2004;20(3):689-97. doi: 10.1590/S0102- 311X2004000300005.
15. Tomita NE, Bijella VT, Franco LJ. Relação entre hábitos bucais e má oclusão em pré-escolares. Rev Saúde Pública. 2000;34(3):299-303. doi: 10.1590/S0034-89102000000300014.
16. Heimer MV, Katz CRT, Rosenblat A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod. 2008;30(6):580-5. doi: doi: 10.1093/ejo/cjn035.
17. Sousa RLS, Lima RB, Florêncio Filho C, Lima KC, Diógenes AMN. Prevalência e fatores de risco da mordida aberta anterior na dentadura decídua completa em pré-escolares na cidade de Natal/RN. Rev Dental Press Ortodon Ortop Facial. 2007;12(2):129-38.
18. Peres KG, Barros AJD, Peres MA, Victora CG. Efeitos da amamentação e dos hábitos de sucção sobre as oclusopatias num estudo de coorte. Rev Saúde Pública. 2007;41(3):343-50. doi: 10.1590/S0034-89102007000300004.
19. Chevitarese ABA, Valle DD, Moreira TC. Prevalence of malocclusion in 4-6 year old Brazilian children. J Clin Pediatr Dent . 2002;27(1):81-5.
20. Kataoka DY, Scavone Junior H, Vellini Ferreira F, Cotrim Ferreira FA, Sato V. Estudo do relacionamento ântero-posterior entre os arcos dentários decíduos, de crianças nipo-brasileiras, dos dois aos seis anos de idade. Rev Dent Press Ortodon Ortop Facial. 2006;11(5):83-92. doi: 10.1590/S1415-54192006000500009.
21. Shimizu RH, Michaelis G, Liu J, Shimizu IA, Ignácio AS. Estudo das características da dentição decídua em crianças entre 3 e 6 anos de idade. J Bras Ortodon Ortop Facial. 2003;8(44):124-31.
22. Farsi NMA, Salama FS. Characteristics of primary dentition occlusion in a group of Saudi children. Int J Paediatri Dent.1996;6(4):253-9. doi: 10.1111/j.1365-263X.1996. tb00254.x.
23. Viggiano D, Fasano D, Monaco G, Strohmenger L. Breastfeeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004; 89(12):1121-123. doi: 10.1136/adc.2003.029728.
24. Furtado ANM, Vedovelho Filho M. A influência do período de aleitamento materno na instalação dos hábitos de sucção não nutritivos e na ocorrência de maloclusão na dentição decídua. RGO - Rev Gaúcha Odontol. 2007;55(4):335-41.
25. Vázquez Nava F, Quezada Castillo JA, Oviedo Treviño S, Saldivar González AH, Sánchez Nuncio HR, Beltrán Guzmán FJ, et al. Association between allergic rhinitis, bottle feeding, non-nutritive sucking habits, and malocclusion in the primary dentition. Arch Dis Child. 2006; 91(10):836-40. doi: 10.1136/adc.2005.088484.
 Correspondence to:
Correspondence to:
JM MASSUIA
e-mail: julianamassuia@hotmail.com
Received on: 14/12/2010
Approved on: 7/6/2011
