










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.4 Porto Alegre Out./Dez. 2012
ORIGINAL / ORIGINAL
Accuracy of radiographic examination in determining the depth of approximal carious lesions in primary molars
Desempenho do exame radiográfico na determinação da profundidade de lesões de cárie proximais em molares decíduos
Ana Bárbara de Araújo LOIOLA I; Ana Luísa Botta Martins de OLIVEIRA II; Rita de Cássia Loiola CORDEIRO II; Lourdes Aparecida Martins dos SANTOS-PINTO II
I Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia. Araraquara, SP, Brasil
II Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia, Departamento de Clínica Infantil. Araraquara, SP, Brasil
ABSTRACT
Objective
The purpose of this study was to evaluate the accuracy of the depth of carious lesions on bitewing radiographs.
Methods
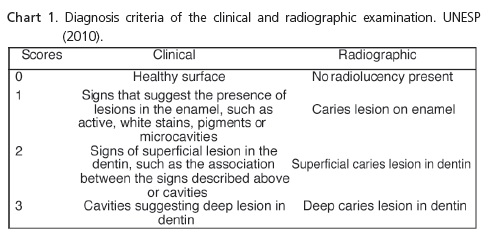
Recently extracted primary molars had their proximal surfaces evaluated visually (EC) and classified as healthy surface (0), signs that suggest the presence of carious lesions in enamel (1), signs of a superficial lesion in dentin (2) and carious lesions in deep dentin (3).
Results
The results were obtained by consensus between the investigators. The gold standard was determined by histological analysis. The values of sensitivity, specificity, accuracy and area under the ROC (Receiver Operating Characteristic) curve were evaluated. There was equilibrium between sensitivity (76.92% EC and 88.46% ER) and specificity (95.83% EC and 95.83% ER). Accuracy was 86.01% (EC) and 88.46% (ER). The Spearman correlation test was used to prove the correlation between clinical and radiographic examinations (0.886), for clinical and histological (0.736) and for radiographic and histological analysis (0.843).
Conclusion
The radiographic examination showed better performance in detection of proximal caries in primary teeth.
Indexing terms: Dental caries. Radiography bitewing. Tooth deciduous.
RESUMO
Objetivo
Avaliar a exatidão da profundidade da lesão de cárie em radiografias interproximais.
Métodos
Molares decíduos recentemente extraídos tiveram suas superfícies proximais avaliadas visualmente (exame clínico) e classificados como superfície hígida (0), sinais que sugerem presença de lesão de cárie em esmalte (1), sinais de lesão superficial em dentina (2) e cavidades sugerindo lesões profundas em dentina (3). As superfícies dentárias foram também examinadas em radiografias interproximais (exame radiográfico) e classificadas como ausência de radiolucidez (0), lesão de cárie em esmalte (1), lesão de cárie superficial em dentina (2) e lesão de cárie em dentina profunda (3).
Resultados
Os resultados foram obtidos por meio de consenso entre os examinadores. O padrão ouro foi determinado pela análise histológica. Foram avaliados os valores de sensibilidade, especificidade, acurácia e área sob a curva Receiver Operating Characteristic. Observou-se um equilíbrio entre os valores de sensibilidade (76,9% exame clínico e 88,4% exame radiográfico) e especificidade (95,8% exame clínico e 95,8% exame radiográfico). A acurácia foi de 86,0% (exame clínico) e 88,4% (exame radiográfico). O teste de correlação de Spearman foi utilizado para a comprovação da correlação entre os exames clínico e radiográfico (0,89), para clínico e histológico (0,7) e para os exames radiográfico e histológico (0,8).
Conclusão
O exame radiográfico apresentou melhor desempenho na detecção da lesão de cárie proximal em dentes decíduos.
Termos de indexação: Cárie dentária. Radiografia interproximal. Dente decíduo.
INTRODUCTION
Caries is a disease caused by the ecological imbalance of native microbiota, going through different stages of development, ranging from invisible demineralization to cavitation. The diagnosis of the lesion located on the approximal surfaces is still regarded as a challenge for dental surgeons by virtue of the difficulty in gaining access and the absence of a method that is capable of accurately identifying its presence, as well as the absence of the disease, making it difficult to plan treatment1-2.
The radiographic examination (x-ray) is considered to be an excellent aid to diagnosis. However, this method underestimates the extent of the lesion and is not able to determine the initial process of demineralization occurring in the enamel due to the dental anatomy and the overlapping of the tooth's mineralized tissues3-5. As a result of this limitation, it is only possible to observe the lesion when the demineralization has already affected at least 30% - 40% of the enamel, causing irreversible mineral loss6. Another difficulty inherent to this type of examination lies in the possibility of the occurrence of distortions caused by structures attached to the dental tissue, as well as the masking of the lesions by restorations close to the region being examined1. Moreover, the radiographic exam does not enable the detection of caries activity7.
Studies conducted by Palma-Dibb et al.5 demonstrate that, in proximal lesions in permanent teeth, the conventional clinical exam presents low sensitivity and high specificity and the caries lesions diagnosed on the enamel have, in the majority of instances, already enveloped the dentin. On the other hand, a strong correlation was observed between the increase in depth found in the radiographic exams and the clinical stage of the lesions in deciduous molars2.
Anatomical accidents inherent to the approximal surfaces of the deciduous molars determine ample contact and in an inverted half-moon format in the middle third of the surface, leveling off in the cervical direction8. This type of contact favors the appearance of caries lesions9 and makes it impossible to get a direct view of the surfaces10-11. Only when they attain greater proportions is the clinical detection of the lesions facilitated by the visual observation of signs such as transparency of the marginal crest, in occlusal view5,12.
The difficulty in diagnosing proximal caries lesions, mainly in the deciduous teeth, is a proven fact1,2,5,13. As the clinical signs are only observed at advanced stages of the lesion, the image observed by means of an x-ray is an important finding in determining its presence. Given the above, the objective of this study was to evaluate the accuracy of the bitewing radiograph in the determination of the depth of the caries lesion in the approximal surfaces of deciduous molars, as well as the effectiveness of its association with the clinical exam and consensus amongst professionals.
METHODS
This research study was approved by the Ethics in Research Committee of the Araraquara Faculty of Dentistry at the Júlio de Mesquita Filho State University (File 04/07).
This study included patients with deciduous molars with recommended extraction due to the advanced root resorption process, with more than 2/3 of the length of the root and which did not present large-scale destruction of the crown or restorations enveloping the approximal surfaces. The sample comprised the clinical examination of all the children frequenting the children's clinic at the Araraquara Faculty of Dentistry in 2009, and those who met with the inclusion criteria were selected.
One trained operator performed the bitewing radiography of the teeth using the Gnatus XR x-ray machine (Gnatus, Ribeirão Preto, SP, Brazil) operating at 60 kvp, 7ma and an exposure time of 0.35 seconds. To validate treatment, the x-rays were processed via the time/ temperature system and stored in tagged cartouches.
Immediately after the extraction, the teeth were placed in flasks containing water with the addition of thymol crystals to prevent bacterial growth12. Two examiners were calibrated by examining 15 extracted teeth and the respective x-rays. The results were analyzed by means of an intra-class correlation test and the examiners judged it appropriate to begin the study when intraexaminer and inter-examiner agreement was over 80%. The examinations were conducted over the course of just one day, under artificial lighting and after drying the dental surface being examined. Through the consensus of both examiners, scores were assigned classifying the surface as healthy or as having signs that suggest the presence and extent of caries lesions, according to Chart 1.
Two weeks after the latest clinical evaluation of the teeth, the x-rays were placed in a negatoscope in a darkened room and the approximal surfaces of the teeth were examined by the two examiners, at which time the scores were assigned based on the presence or absence of radiolucency (Chart 1), based on a consensus. This evaluation was repeated one week later.
Once the examinations were over, the teeth were sectioned in the region corresponding to the center of the approximal surface or in the middle of the site of the caries lesion, using an ISOMET 1000® precision saw (Buehler Ltd., Lake Bluff, Illinois, USA) and a low-speed diamond disc, with copious cooling. The sectioned surfaces were sanded lengthwise in a rotating electric polisher using wet carbide sandpaper with decreasing grits of 320, 400, 600, 1200 and 2000. The dental surfaces were subjected to a histological analysis in an optical microscope (10x magnification) for the evaluation of the presence and depth of the lesion, both in the enamel and the dentin. The sites were categorized, according to the extent of the caries lesion, as healthy (D0), caries lesion in the outer half of the enamel (D1), caries lesion in the inner half of the enamel (D2), caries lesion in dentin (D3) and deep caries lesion in dentin (D4), forming the sample's gold standard. The Spearman correlation test was used to prove the correlation between the scores and the gold standard. Sensitivity and specificity were also calculated to check the effectiveness of both methods.
RESULTS
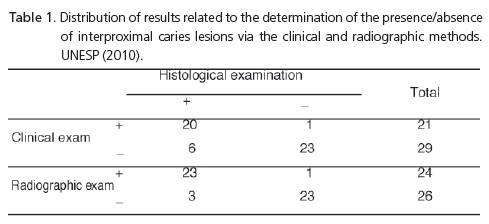
A total of 16 healthy teeth were found, 8 teeth with caries lesion in the enamel and 26 with lesion in the dentin. The comparison of data obtained, using lesion detection methods, with the histological data is shown in Table 1.
Agreement between the methods and the Gold Standard showed the following values: true positive 20/23, true negative 23/23, false positive 1/1 and false negative 6/3, for the clinical and radiographic exams, respectively.
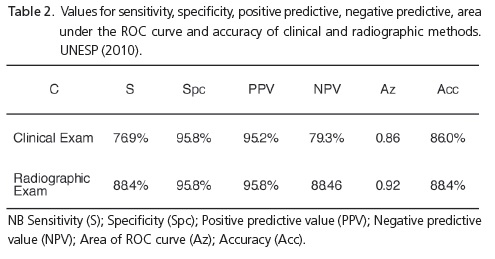
Table 2 shows the following values: sensitivity, specificity, positive predictive, negative predictive, area under the ROC curve and accuracy of clinical and radiographic methods.
High values were found both for Sensitivity and Specificity, indicating agreement between the methods, both for the presence of caries lesion and also for its absence. However, the radiographic examination demonstrated greater equilibrium between the sensitivity and specificity values.
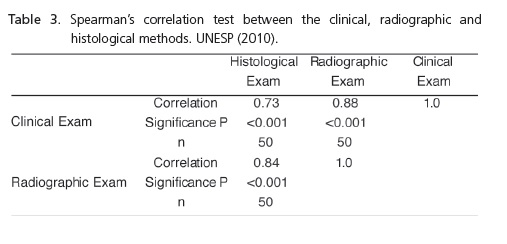
Using Spearman's correlation test, we obtained correlation between the scores of the clinical, radiographic and histological examinations. The results appear in Table 3.
DISCUSSION
The determination of the presence/absence, as well as the depth of the caries lesion, has been frequently investigated due to its importance in clinical practice and due to the fact that there is no single precise diagnosis method1,2,14. The methods analyzed in the present study are the ones most frequently used in the daily routine of dental surgeons, thereby justifying the need for an understanding of its advantages and also its limitations.
The diagnosis of proximal caries lesion is extremely difficult, mainly with primary teeth1,2,13, however its early detection enables the use of a more conservative therapy, with the adoption of preventive measures, instead of invasive measures such as restoration. The association of the clinical aspect of the approximal surfaces with the image observed radiographically is a hugely important finding, enabling the identification of the initial carious lesion.
Due to the difficulty of access and direct examination of the approximal surface, as a consequence of its anatomic contact, bitewing radiography becomes an effective, auxiliary method in the detection of caries lesions. According to Baelum et al.15, this technique allows for the observation of proximal lesions undetectable via clinical examination. In the present study, the values for accuracy in both methods were high (86.01% for the clinical examination and 88.46% for the radiographic examination). Authors such as Chaves et al.16 state that the association between the clinical and radiographic methods is essential for the greater accuracy of the diagnosis14. Our results agree with the abovementioned author (Spearman's correlation (0.88; p<0.001)
The comparison between the histological exam and the clinical and radiographic exams were in agreement for both the presence and the absence of caries lesion, a fact which resulted in high sensitivity and specificity values for both methods, confirming not only the ability of these methods to detect the presence of disease (sensitivity) but also the ability to identify its absence (specificity). The values for Az (0.86 and 1) confirm these results.
High values were found for the results of True Positive and True Negative and low values for False Positive and False Negative, for both methods, demonstrating that it would be unlikely for healthy surfaces to be restored or for diseased surfaces to be overlooked. It is believed that not only the experience of the examiners but also their consensus in the assignment of scores has led to these results. The dental surgeon's clinical experience, with radiographic interpretation and in determining clinical signs16, contributes positively to the diagnosis of caries lesions12, mainly in incipient lesions. In this way, the methods employed in this study were executed in detailed fashion, with the clinical and radiographic analyses being performed by two experienced examiners who, previously trained and in consensus, classified each of the evaluated surfaces according to the presence/absence and extent of caries lesions.
Despite the high values, the clinical examination showed lower sensitivity than the radiographic exam and also lower NPV values (79%). The findings that the clinical examination may have demonstrated lower sensitivity than other methods evaluated was also reported by Huysmans et al.17 when they compared bitewing x-rays via visual inspection and the electrical conduction system. On the other hand, Nytun et al.18 and Silva Neto et al.19 reported greater sensitivity in the clinical exam than in the radiographic exam, while the latter has greater specificity than the clinical exam. Primo et al.20 concluded, in their review of the topic, that the association of diagnostic methods enables an increase in sensitivity, maintaining high specificity, making the diagnosis more effective, and also stated that the visual inspection and the radiographic exam are more efficient in detecting interproximal caries lesion in situations of low prevalence of the disease. Chaves et al.16 stated that the bitewing radiographic exam has greater Sensitivity for the detection of cavitated lesions than that in examinations conducted on non-cavitated lesions or teeth with no visible cavities. The radiographic image underestimates the size of the lesion in such a way that the observed radiolucency never corresponds to its depth. Moreover, bitewing radiography has greater Sensitivity in the detection of lesions in dentin11,21.
Many studies are developed with the aim of ascertaining the reliability of the radiographic image. Feldens et al.13, in a study on the correlation between clinical and radiographic examinations, in proximal caries lesions in primary molars, concluded that there is a close correlation between the presence of radiolucency and the presence of cavitation on the approximal surface. Nevertheless, they observed that bitewing radiography demonstrates a lower ability to differentiate noncavitated lesions. Ratledge et al.22 confirmed that 85% of the lesions that presented radiographically in the outer third of the dentin, were clinically cavitated. In addition, they concluded that lesions whose x-ray images presented more than 0.5 mm from the dentino-enamel junction, had a greater probability of being cavitated. Wenzel et al.6 stated that, radiographically, the carious lesion is observed when the demineralization has already reached at least 30-40% of the enamel, there being an irreversible loss of mineral. Silva Neto et al.19, in their studies, found that the radiographic exam did not detect carious lesions that, histologically, were to be found on the enamel or on the outermost third of the dentin, and that only the surfaces clinically diagnosed as cavitated were detected in the radiographic exam, confirming that this method is not recommended for the detection of incipient lesions, being more effective in lesions that have already passed the dentino-enamel junction.
In this study, more than one half of the teeth examined (52%) had carious lesions in dentin. It is probable that this fact has contributed to the Sensitivity results found and to the agreement between the results of the clinical and radiographic exams.
Hopcraft & Morgan21 studied the association of the clinical and radiographic exams. When analyzed separately, just 30% of lesions were detected via the clinical examination while 95% were detected through the association of the two methods. DeJean et al.23, when evaluating the clinical exam and the bitewing radiographic exam, as means for diagnosing hidden caries, noted that the number of surfaces clinically diagnosed as being carious was greater than caries lesions observed radiographically and that 50% of the surfaces that had presented clinically as translucent, were radiographically carious, indicating a relative association between the presence of translucency and the presence of caries lesion.
Amongst the difficulties encountered in the present study, we would highlight the criteria for inclusion of teeth and the acquisition of quality x-rays. The limitations of a study carried out in vitro should also be taken into consideration, although all possible care was taken, both in the detailed performance of the taking of standardized x-rays and in the interpretation of the images.
IN the knowledge that early detection of caries is a challenge for dental surgeons, as Dentistry today focuses on adopting preventive measures rather than curative measures, the association between the visual and radiographic methods, as well as the abilities and technique of the professional, are of extreme importance to the success of the diagnosis and the consequent treatment plan.
CONCLUSION
The radiographic exam was seen to be more accurate in determining lesions of greater depth and the clinical exam more effective in lesions limited to the enamel. The association of the two methods was of extreme importance to correct diagnosis.
Collaborators
ABA LOIOLA and ALBM OLIVEIRA took part in the performance of the methodology, composition of the article and the bibliographical survey. RCL CORDEIRO and LAM SANTOS-PINTO took part in the statistical analysis, guidance in the research project and the composition of the article.
REFERENCES
1. Araújo RM, Araújo MAM, Vannucci MG. Comprovação clínica de cáries interproximais diagnosticadas radiograficamente. Rev Odontol UNESP. 1998;27(2):553-65. [ Links ]
2. Dhremer T, Figueiredo MC, Bárbara Z, Sampaio MS, Barreto VC. Estudo comparativo entre as densidades ópticas de superfícies proximais de molares decíduos com diagnóstico de hígidos e de lesão de cárie in vitro. Pesqui Bras Odontopediatria Clín Integr. 2006;6(2):189-97.
3. Allison PJ, Schwartz S. Interproximal contact points and proximal caries in posterior primary teeth. Ped Dent. 2003;25(4):334-40.
4. Heaven TJ, Firestone AR, Weems RA. The effect of multiple examinations on the diagnosis of approximal caries and the restoration of approximal surfaces. Oral Surg Oral Med Oral Pathol. 1999;87:386-91.
5. Palma-Dibb, Menato AL, Bocangel JS, Belsuzarri ALO, Matson E. Comparação clínica entre diferentes métodos de diagnóstico de cárie proximal. Braz Dent J. 1999;2(1):85-92.
6. Wenzel A, DrOdont, Haiter-Neto F, Gotfredsen E. Influence of spatial resolution and bit depth on detection of small caries lesions with digital receptors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(3):418-22. doi: 10.1016/j. tripleo.2006.05.016.
7. Pitts NB, Rimmer PA. An in vivo comparison of radiographic and directly assessed clinical caries status of posterior approximal surfaces in primary and permanent teeth. Caries Res. 1992;26(2):146-52.
8. Fejerskov O. Changing paradigms in concepts on dental caries: consequences for oral health care. Caries Res. 2004;38(3):182- 91. doi: 10.1159/000077753.
9. Baellum V, Machiulskiene V, Nyvad B, Richards A, Vaeth M. Application of survival analysis to carious lesion transitions in intervention trials. Community Dent Oral Epidemiol. 2003;31(4):252-60. doi: 10.1034/j.1600-0528.2003.00045.x.
10. Vanderas AP, Manetas C, Koulatzidou M, Papagiannoulis L. Progression of proximal caries in the mixed dentition: A 4-year prospective study. Pediatr Dent. 2003;25(3):229-34.
11. Zanin L, Assaf AV, Kozlowski FC, Meneghim MC, Pereira AC. Uma abordagem sobre novos e tradicionais métodos de diagnóstico para cárie dentária. ROBRAC. 2001;10(30):4-8.
12. Carmona GP, Devito KL, Pontual MLA, Haiter Neto F. Influência da experiência profissional no diagnóstico radiográfico de cáries. Cienc Odontol Bras. 2006;9(1):87-92.
13. Feldens CA, Tovo MF, Kramer PF, Feldens EG, Ferreira SH, Finkler M. An in vitro study of the correlation between clinical and radiographic examinations of proximal carious lesions in primary molars. J Clin Pediatr Dent. 2003;27(2):143-8.
14. Amore R, Anido AA, Moraes LC, Moraes MEL. Comparação entre diagnóstico clínico e radiográfico da cárie dental. Pós-Grad Rev Fac Odontol São José dos Campos. 2000;3:62-8.
15. Baelum V, Heidmann J, Nyvad B. Dental caries paradigms in diagnostic research. Eur J Oral Sci. 2006;114(4):263-77. doi: 10.1111/j.1600-0722.2006.00383.x.
16. Chavez LP, Fernander CV, Wang L, Barata TJE, Walter LRF. Cárie proximal - Fundamentos e recursos para diagnóstico precoce. Odontol Clín Cient. 2010;9(1):33-7.
17. Huysmans DNJM, Longbottom, Pitts NB. Electrical methods in occlusal caries diagnosis: an in vitro comparison with visual inspection and bite-wing radiography. Caries Res. 1998;32(5):324-9.
18. Nytun RB, Raadal M, Espelid I. Diagnosis of dentin involvement in occlusal caries based on visual and radiographic examination of the teeth. Scand J Dent Res. 1992;100(3):144-8.
19. Silva Neto JM, Santos RL, Sampaio MCC, Sampaio FC, Passos IA. Radiographic diagnosis of incipient proximal caries: an ex-vivo study. Braz Dent J. 2008;19(2):97-102. doi: 10.1590/S0103- 64402008000200002.
20. Primo L, Tostes M, Ando T, Rodrigues CRMD. Sensibilidade e especificidade de métodos de diagnóstico da lesão de cárie na superfície proximal. RPG Rev Pos-Grad. 1997;4(1):43-9.
21. Hopcraft MS, Morgan MV. Comparison of Radiographic and Clinical Diagnosis of Approximal and Occlusal Dental Caries in a Young Adult Population. Community Dent Oral Epidemiol. 2005;33:212-8.
22. Ratledge DK, Kidd EAM, Beighton DA. A clinical and microbiological study of approximal carious lesions. Part 1: The relationship between cavitation, radiographic lesion depth, the site-specific gingival index and the level of infection of the dentine. Caries Res. 2001;35:3-7. doi: 10.1159/000047423.
23. DeJean KS, Caldas LD, Góis DN, Souza CS. Lesão de cárie oculta: um estudo de diagnóstico e prevalência. Clínica e Pesquisa em Odontologia - UNITAU. 2009;1:7-13.
 Correspondence to:
Correspondence to:
ANR LOIOLA
e-mail: anabarbaraloiola@hotmail.com
Received on: 1/7/2010
Final version resubmitted on: 10/12/2010
Approved on: 11/3/2011
