










 Inglés
Inglés




 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.60 no.4 Porto Alegre oct./dic. 2012
ORIGINAL / ORIGINAL
Prevalence and distribution of tooth agenesis in a pediatric population: a radiographic study
Prevalência e distribuição de agenesias dentárias em pacientes pediátricos: um estudo radiográfico
Ana Sofia Estima da Cunha COELHO I; Viviana Marisa Pereira MACHO I; David José Casimiro de ANDRADE I; Ana Paula Coelho de Macedo AUGUSTO I; Cristina Maria Ferreira Guimarães Pereira AREIAS I
I Universidade do Porto, Faculdade de Medicina Dentária. Porto, Portugal
ABSTRACT
Objective
The purpose of this study was to assess the prevalence of hypodontia and its distribution by sex, arch and quadrant, through the analysis of panoramic radiographs from the pediatric population of the Faculty of Dentistry of the University of Oporto, in Portugal.
Methods
Panoramic radiographs of 1,438 patients of the Faculty of Dentistry of the University of Oporto (714 boys and 724 girls between the ages of 6 and 15) were evaluated to determine the occurrence and distribution of tooth agenesis. Chi-square and Fisher's Exact Tests were performed. The level of significance was set at 5%.
Results
The prevalence of hypodontia was 8% (excluding the third molar). Hypodontia was found in the mandible of 74 patients (64.3%). The most commonly missing teeth were the mandibular second premolars (28.6%). The maxilla had 52.3% of the dental agenesis detected. Similarity in the distribution of missing teeth between left and right sides of the dental arches was also detected. The prevalence of oligodontia was 0.42% and the average number of missing teeth per affected child was 2.31. There were no statistically significant differences between sexes.
Conclusion
In a pediatric population of 1,438 patients, the prevalence of hypodontia was 8% (excluding the third molar). The results are consistent with those previously described in different populations.
Indexing terms: Anodontia. Panoramic radiography. Prevalence.
RESUMO
Objetivo
Realizar um estudo epidemiológico sobre as agenesias dentárias, através da análise radiográfica de uma população pediátrica da Faculdade de Medicina Dentária da Universidade do Porto, definindo a sua prevalência e conhecendo a sua distribuição por sexo, arcada e quadrante.
Métodos
As radiografias panorâmicas de 1.438 pacientes da Faculdade de Medicina Dentária da Universidade do Porto (714 do sexo masculino e 724 do sexo feminino, de idades compreendidas entre os 6 e os 15 anos) foram analisadas para determinar a ocorrência e distribuição de agenesias dentárias. A análise estatística foi realizada através da aplicação do Teste do Qui-quadrado de independência e do Teste Exato de Fisher, utilizando o nível de significância de 5%.
Resultados
A prevalência de hipodontia foi de 8,0% (excluindo o 3º molar). Foram identificados 74 pacientes (64,3%) com agenesias na mandíbula. Os pré-molares inferiores foram os dentes com maior frequência de agenesia (28,6%). A maxila continha 52,3% das agenesias detetadas.Não foi detetada diferença estatisticamente significativa entre o lado esquerdo e direito das arcadas. A prevalência de oligodontia foi de 0,42% e obteve-se uma média de 2,31 dentes ausentes por paciente afetado. Não se encontraram diferenças estatisticamente significativas na variável sexo.
Conclusão
Numa população de 1438 pacientes pediátricos, 8,0% apresentaram agenesias dentárias (excluindo o 3º molar). Os resultados obtidos enquadram-se nos anteriormente descritos em diferentes populações.
Termos de indexação: Anodontia. Radiografia panorâmica. Prevalência.
INTRODUCTION
In the course of the development of the human dental organs, these undergo various histological, physiological and biochemical changes that are responsible for the physiological and functional maturation of the dentition1.
Odontogenesis, or tooth development, which begins around the 5thand 6th week of life inside the womb, comprises 4 phases: proliferation, histodifferentiation, morphodifferentiationand calcification1-2. Affecting both the dentitions, various alterations may occur during the distinct stages of tooth development, causing numerical anomalies if they occur in the first phase, and anomalies of size, shape, structure and color, if they occur in the other phases2.
Numerical anomalies are classified into hypodontia (congenital absence of one or more teeth), oligodontia (a subdivision of the first group, used in cases of agenesis of six or more teeth, except for the 3rdmolar), anodontia (complete absence of teeth) and hyperdontia (growth of excessive number of teeth)1,3.
Hypodontia is one of the more common tooth anomalies and, with the exception of the 3rd molar, mostly affects the mandibular second premolars and maxillary lateral incisors. Among the various studies, again excluding the 3rdmolar, the prevalence of agenesis varies between 0.03%and 12.6% in the permanent dentition and, according to some authors, is more common in the female sex4-5. Unilateral occurrence predominates, with the exception of the agenesis of the maxillary lateral incisors, which is often bilateral3,6.There is a correlation between agenesisof temporary teeth and permanent teeth, being more common in the latter7-8.
Hypodontiais generally associated with microdontia, i.e. alterations in shape, ectopia, delayed formation and eruption of the teeth, diastemas, reduction in alveolar growth, infraocclusion of the deciduous molars and enamel hypoplasia9-12.
The various clinical manifestations of hypodontia demonstrate its genetic and phenotypical heterogeneity. Many cases of hypodontiaseem to be autosomal dominant with incomplete penetration and variable expressiveness, but autosomal recessive cases or cases linked to gender have also been described. There are recognized mutations of genes MSX1, PAX9 and AXIN211,13-14. Other mutations were also identified in hereditary syndromes that most often exhibit dental agenesis, as is the case of Trisomy 21 (absence of one or more teeth) and Ectodermal Dysplasia (total or substantial absence of teeth)11-12.
Patients with a cleft lip and/or palate exhibit a greater prevalence of tooth anomalies of number, with a particular predominance of absent maxillary lateral incisors, explained by the anatomical location and the timingof development. The prevalence of agenesis away from the site of the malformation is also higher than in the general population15-16.
The radiographic study, more specifically panoramic radiography, is a complementary means of diagnosis which is essential for a global view of the maxillo-mandibular structures which it provides and which frequently exhibit pathological characteristics that go undetected using other means1,17.
Early identification of dental agenesis and appropriate intervention, can reduce or prevent a number of complications, permitting adequate development and growth, achieving functional, occlusal and esthetic harmony.
As the existence of studies on dental agenesis are scarce in Portugal, and bearing in mind the interest and importance of the topic to a clinical practice that is more complete and aware of the diverse aspects that the theme encompasses, the aim of the present study is to carry out an epidemiological study of these anomalies, via a radiographic analysis of the pediatric population at the Faculty of Dental Medicine of the University of Oporto, by defining the prevalence of agenesis found in the studied population and finding out its distribution by sex, arch and quadrant.
METHODS
A research study was conducted on the database of the FMDUP clinic, by selecting patients between 6 and 15 years of age. A total of 2,031 patients resulted.
The cases of the selected patients were analyzed between October 2010 and March 2011, and the required information was recorded in a database, with recourse to the software Microsoft Office Access 2007® (Microsoft®), containing the following information: patient code, sex, place of abode, date of birth, date the panoramic x-ray was taken, presence of syndromes and existence of dental agenesis, excluding the 3rd molar. The identification of absent teeth was performed using the two-digit notation adopted by the World Dental Federation (FDI).
Those patients who had never had a panoramic x-ray or who had only had one prior to the age of 6, were excluded from the study.Any x-rays poor in technical quality were also excluded. Accordingly, a total of 1,438 patients made up the study.
In order to prevent incorrect diagnosis through the extraction of the tooth in question, and when there were several x-rays relating to the same patient, the oldest x-ray was selected, although all of them were evaluated in order to confirm the diagnosis.
A tooth was regarded as being absent when it was not possible to identify, in the x-ray, the mineralization of the crown or indeed any evidence of extraction.
Ten per cent of the x-rays were reanalyzed by another examiner under the same conditions of interpretation, having ascertained a Kappainter-observer coefficient of 1.0.
The rules of conduct adopted by the Declaration of Helsinki were observed as well as the prevailing domestic legislation, ensuring the required confidentiality of the personal information collected.
The present study was approved by the Research Ethics Committee of FMDUP, and filed under opinion number 880387.
Statistical analysis
The statistical analysis was performed using the software package Statistical Package for the Social Sciences® (SPSS®) v19. In order to carry out the hypothesis tests on theindependence of the variables, the Chi-square test of Independence or the Fisher Exact Test were applied, as appropriate. A level of significance of 5% (p=0.05) was used for all the tests.
RESULTS
Of the 1,438 panoramic radiographs analyzed, 714 (49.7%) belonged to male patients and 724 (50.3%) to female patients. Their ages ranged from 6 to 15, the average age being 8.82 years (σ = 2,18).
A total of 9 patients were identified as having Trisomy 21 (8 male and 1 female).
Excluding the 3rd molar, the prevalence of agenesis in the permanent dentition in the population studied was 8% (115 patients). Of these, 49.6% were male and 50.4% female, there being no statistically significant difference between the sexes (p=0.984).
A total of 266 cases of agenesis were identified with an average of 2.31 absent teeth per affected child.
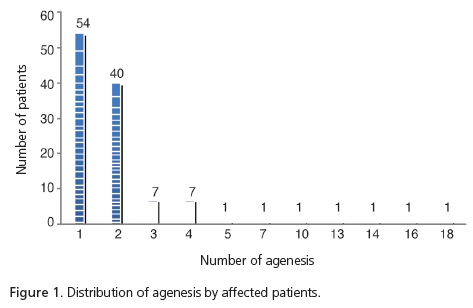
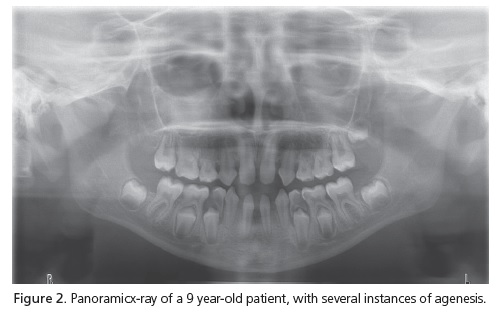
Amongst the 115 patients with agenesis, 54 (47%) had just one agenesis while 61 (53%) had two or more. The most frequent cases of isolated agenesis were those of teeth 45 and 35. Six patients (0.42%) exhibited oligodontia –of these, four had Trisomy 21 and one was about to undergo a genetic study. The distribution of agenesis by affected patient is represented in Figure 1. In Figure 2, a panoramic x-ray can be seen of a patient with several instances of agenesis.
Of the 115 patients with agenesis, 62 (53.4%) had them in the maxilla. In these patients, there were 139 cases of agenesis distributed identically in both quadrants (51.1% in the 1st and 48.9% in the 2nd). The maxilla was involved in 52.3% of the detected cases of agenesis.
Seventy-four patients (64.3%) were identified with agenesis in the mandible. They accounted for 127 cases (45.7% in the 3rd quadrant and 54.3% in the 4th).
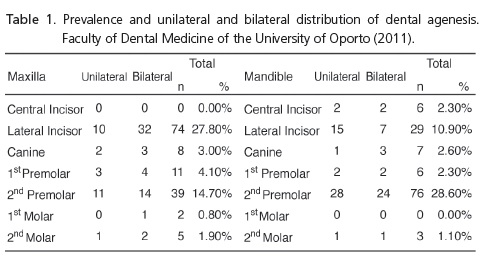
Table 1 shows the prevalence and unilateral and bilateral distribution of dental agenesis.
Theinstances of agenesis most frequently found were in the mandibular second premolars (28.6%), followed by the maxillary lateral incisors (27.8%) and the maxillary second premolars (14.7%).
Bilateral agenesis of the maxillary lateral incisors occurred more frequently than unilateral agenesis (76.2% and 23.8%, respectively). In situations of agenesis of the mandibular lateral incisors, the opposite was true, with 68.2% of cases exhibiting unilateral agenesis. As regards the remaining teeth, there was no significant unilateral or bilateral predominance. In total, 55.6% of the cases of agenesis detected were bilateral. Of the 9 patients with Trisomy 21, 8 (88.9%) presented with agenesis. The difference between this value and that found in patients without syndromes is statistically significant (p=0.00).
DISCUSSION
Various studies exist in respect of theprevalence of dental anomalies of number, demonstrating the variation that exists between populations, continents and races.
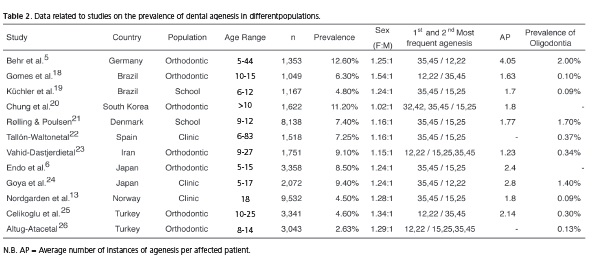
In the present study, the prevalence of dental agenesis was 8%. The value obtained lies within the parameters found in other studies (Table 2). The studies shown in Table 2 were selected according to the following criteria: sample size over 1,000; diagnosis made via radiographic examination; presentation of the prevalence of agenesis except for the 3rd molars; presentation of the prevalence of agenesis with the exclusion of the temporary dentition. The required information was taken from the tables, figures or text, it being necessary on occasion to perform a number of calculations. The identification of the teeth was conducted using the two-digit notation of the FDI.
The wide range of prevalence of agenesis reported in the various studies may be attributable to the differences in the samples (age, sex, ethnicity, population) as well as the type of radiographic examination analyzed. Theprevalence of agenesis varies between 2.63%in a population in Turkey26 and 12.6%, in a population in Germany5.
The age at which the diagnosis is carried out is of paramount importance. The calcification of the crown in the mandibular second premolars, the last to undergo the process of mineralization, with the exception of the third molars, is generally complete by the age of 6. The non-identification of the dental germs in these teeth,by radiographic examination, before the age of 6, could lead to hasty diagnosis. Being older can also lead to an incorrect diagnosis through the extraction of the tooth in question4,8,24.
As the majority of existing studies on the prevalence of tooth anomalies of number has been carried out on populations in need of orthodontic treatment5-6,18,20,23,25-26, it should be borne in mind that patients with agenesis frequently present other dentoalveolar alterations, thus demonstrating a greater need for orthodontic treatment, with a possible increase in prevalence of dental anomalies in these studies3.
Although the female sex seems to be more susceptible to tooth agenesis, a statistically significant difference between the sexes has not been reported5-6,14,18-26. Theprevalence of agenesis in the female sex is between 1.02 and 1.54 times higher than with the male sex18,20.
The mandibular premolars were identified as the most frequent agenesis (28.6%). Although the majority of studies are in agreement with the results found5-6,14,19,21-22,24, other studies argue that agenesis of the maxillary lateral incisors is the most common18,23,25-26. Though not corroborated by the other studies, Chung et al.20, in a South Korean study of a population in need of orthodontic treatment, considered agenesis of the mandibular lateral incisors to be as prevalent as that of the mandibularpremolars, having obtained a prevalence of 20.4% for each of the groups of teeth.
No cases of agenesis were found in the maxillary central incisors or the mandibular first molars. Just one case of bilateral agenesis was detected in the maxillary first molars, representing 0.8% of the cases of agenesis identified. There have been many studies that present this tooth as being the most stable on account of the limited number of cases of agenesis found18-20,24,27. Different studies also report that the maxillary central incisors and mandibular canines have the least frequent agenesis5,18-21.
In total, 55.6% of the cases of agenesis detected were bilateral. Although Goya et al.24 have also found a predominance of bilateral situations (74.6%), several studies have reported cases of unilateral agenesis as being the more common19-21.
Oligodontia is rare and its prevalence varies between 0.09% and 2%5,14,19, the present study obtaining a value of 0.42%.
A total of 266 cases of agenesis were found, with an average of 2.31 absent teeth per affected patient. This value is located between the averages reported by other studies, varying between 1.23 and 4.055,23.
The maxilla presented in52.3% of the detected cases of tooth agenesis. This predominance, though small, is in agreement with some of the studies that have been published18,23,25. As for Endo et al.6, Kückler et al.19 and Chung et al.20, these reported a higher prevalence of agenesis in the lower arch. None of these results, however, present statistically significant differences.
There have also been some studies on the prevalence of tooth agenesis in the Portuguese population. In these studies, the prevalence of agenesis varies between 5.6% and 7.4%28-30. Although the populations studied are quite small, the results are in harmony with studies carried out on other populations. The present study found a slightly higher prevalence (8%) than those found in Portugal up to the present time.
Contrary to previous studies, which reported predominance in the female sex, however without there being statistically significant differences between the sexes, Leitão29 did find a statistically significant difference for agenesis of the mandibular second premolars, where the male sex was more affected. However, considering his sample as a whole, the difference found for this variable cannot be expressed statistically.
CONCLUSION
In a population of 1,438 pediatric patients, 8% presented with dental agenesis (excluding the 3rdmolars). The mandibularpremolars were the teeth with the highest frequency of agenesis.
Dental agenesis presents with significant prevalence and is often associated with various dentoalveolar problems. Early diagnosis of these anomalies is imperative to successful treatment, by restoring the dental esthetic, occlusion and function and minimizing the risk of possible complications.
Collaborators
ASEC COELHO was responsible for the conception and composition of the article. VMP MACHO, JC ANDRADE, APCM AUGUSTO and CMFGP AREIAS were responsible for the critical review of the intellectual content and for the composition of the article.
REFERENCES
1. Guedes-Pinto AC. Odontopediatria. 8ª ed. São Paulo: Editora Santos; 2010. [ Links ]
2. Costa ALM, Paiva E, Ferreira LP. Saúde oral infantil: uma abordagem preventiva. Rev Port Clin Geral. 2006;22(3):337-46.
3. Polder BJ, Van't Hof MA, van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32(3):217-26. doi: 10.1111/j.1600-0528.2004.00158.x.
4. Mattheeuws N, Dermaut L, Martens G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod. 2004;26(1):99-103. doi: 10.1093/ejo/26.1.99.
5. Behr M, Proff P, Leitzmann M, Pretzel M, Handel G, Schmalz G, et al. Survey of congenitally missing teeth in orthodontic patients in Eastern Bavaria. Eur J Orthod. 2011;33(1):32-6. doi: 10.1093/ejo/cjq021.
6. Endo T, Ozoe R, Kubota M, Akiyama M, Shimooka S. A survey of hypodontia in Japanese orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129(1):29-35. doi: 10.1016/j. ajodo.2004.09.024.
7. Pinkham JR, Casamassimo PS, Fields HW, McTigue DJ, Nowak A. Pediatric dentistry: infancy through adolescence. 4th ed. EUA: Mosby; 2005.
8. Campos V, Cruz R, Mello H. Diagnóstico e tratamento das anomalias da odontogênese. São Paulo: Editora Santos; 2004.
9. Garib D, Alencar B, Lauris J, Baccetti T. Agenesis of maxillary lateral incisors and associated dental anomalies. Am J Orthod Dentofacial Orthop. 2010;137(6):732.e1-732.e6. doi: 10.1016/j. ajodo.2009.12.024.
10. Uslenghi S, Liversidge HM, Wong FSL. A radiographic study of tooth development in hypodontia. Arch Oral Biol. 2006;51(2):129-33. doi: 10.1016/j.archoralbio.2005.06.004.
11. Bailleul-Forestier I, Molla M, Verloes A, Berdal A. The genetic basis of inherited anomalies of the teeth: Part 1: Clinical and molecular aspects of non-syndromic dental disorders. Eur J Med Genet. 2008;51(4):273-91. doi: 10.1016/j.ejmg.2008.02.009.
12. Garib D, Alencar B, Ferreira F, Ozawa T. Associated dental anomalies: the orthodontist decoding the genetics which regulates the dental development disturbances. Dental Press J Orthod. 2010;15(2):138-57. doi: 10.1590/S2176- 94512010000200017.
13. De Coster PJ, Marks LA, Martens LC, Huysseune A. Dental agenesis: geneticandclinicalperspectives. J Oral Pathol Med. 2009;38(1):1-17. doi: 10.1111/j.1600-0714.2008.00699.x.
14. Shimizu T, Maeda T. Prevalence and genetic basis of tooth agenesis. Jpn Dent Sci Rev. 2009;45(1):52-8. doi: 10.1016/j. jdsr.2008.12.001.
15. Bartzela TN, Carels CEL, Bronkhorst EM, Ronning E, Rizell S, Kuijpers-Jagtman AM. Tooth agenesis patterns in bilateral cleft lip and palate. Eur J Oral Sci. 2010;118(1):47-52. doi: 10.1111/j.1600-0722.2009.00698.x.
16. Akcam M, Evirgen S, Uslu O, Memikoğlu U. Dental anomalies in individuals with cleft lip and/or palate. Eur J Orthod. 2010;32(2):207-13. doi: 10.1093/ejo/cjp156.
17. Rajab LD, Hamdan MAM. Supernumerary teeth: review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12(4):244-54.
18. Gomes RR, Fonseca JAC, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010;32(3):302-6.
19. Küchler EC, Risso PA, Costa MC, Modesto A, Vieira AR. Studies of dental anomalies in a large group of school children. Arch Oral Biol. 2008;53(10):941-6. doi: 10.1016/j. archoralbio.2008.04.003.
20. Chung CJ, Han J-H, Kim K-H. The pattern and prevalence of hypodontia in Koreans. Oral Dis. 2008; 14(7):620-5. doi: 10.1111/j.1601-0825.2007.01434.x.
21. Rølling S, Poulsen S. Agenesis of permanent teeth in 8138 Danish schoolchildren: prevalence and intra-oral distribution according to gender. Int J Paediatr Dent. 2009;19(3):172-5. doi: 10.1111/j.1365-263X.2008.00958.x.
22. Tallón-Walton V, Nieminen P, Arte S, Carvalho-Lobato P, Ustrell- Torrent JM, Manzanares-Céspedes MC. An epidemiological study of dental agenesis in a primary health area in Spain: Estimated prevalence and associated factors. Med Oral Patol Oral Cir Bucal. 2010;15(4):e569-74. doi:10.4317/medoral.15. e569.
23. Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N. Non-syndromichypodontia in an Iranian orthodontic population. J Oral Sci. 2010;52(3):455-61. doi: 10.2334/josnusd.52.455.
24. Goya HA, Tanaka S, Maeda T, Akimoto Y. An ortopantomographie study of hypodontia in permanent teeth of Japanese pediatric patients. J Oral Sci. 2008;50(2):143-50.
25. Celikoglu M, Kazanci F, Miloglu O, Oztek O, Kamak H, Ceylan I. Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med Oral Patol Oral Cir Bucal. 2010;15(5):e797-801. doi:10.4317/medoral.15.e797.
26. Altug-Atac AT, Erdem D. Prevalence and distribution of dental anomalies in orthodontic patients. Am J Orthod Dentofacial Orthop. 2007;131(4):510-4. doi: 10.1016/j.ajodo.2005.06.027.
27. Abe R, Endo T, Shimooka S. Maxillary first molar agenesis and other dental anomalies. Angle Orthod. 2010;80(6):1002-9. doi: 10.2319/020210-69.1.
28. Cruz JP. Prevalência da oligodontia numa amostra da clínica ortodôntica privada. Rev Port Estomatol Cir Maxilofac. 1989;30:71-4.
29. Leitão P. Prevalência da má oclusão em crianças de 12 anos da cidade de Lisboa. Rev Port Estomatol Cir Maxilofac. 1993;33:193-201.
30. Carvalho S, Mesquita P, Afonso A. Prevalência das anomalias dentárias de número numa população portuguesa: estudo radiográfico. Rev Port Estomatol Med Dent Cir Maxilofac. 2011;52(1):7-12.
 Correspondence to:
Correspondence to:
ASEC COELHO
e-mail: anasofiacoelho@gmail.com
Received on: 28/6/2011
Final version resubmitted on: 20/9/2011
Approved on: 23/11/2011
