










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.1 Porto Alegre Jan./Mar. 2013
ORIGINAL / ORIGINAL
Relationship of the hyoid bone and posterior surface of the tongue for class II division 1 orthodontic patients
Posição do osso hióide e da superfície posterior da língua em melanodermas com maloclusão de classe II divisão 1
Elizete Nejm CARVALHOI; Darcy Flávio NOUERII; Ivana Uglik GARBUII; Paulo Roberto Aranha NOUERI
I Faculdade São Leopoldo Mandic, Curso de Odontologia, Programa de Pós-Graduação em Ortodontia
II Universidade Estadual de Campinas, Faculdade de Odontologia, Departamento de Odontologia Infantil, Piracicaba, SP, Brasil
ABSTRACT
Objective
The objective of this study was to evaluate the hyoid bone position in the sagittal and vertical planes, on dolichoprosopic, brachyprosopic and mesoprosopic facial types.
Methods
Individuals with Angle Class II Division 1 malocclusion were compared with a control group (Class I). Lateral teleradiographs of 45 dark-skinned individuals (experimental group) were selected from the scientific archives of the São Leopoldo Mandic College of Dentistry. The control group comprised 22 dark-skinned individuals with Angle Class I malocclusion, selected from the same archives. The cephalometric distances ANS-PNS, ANS-PH, PT-PoPh, BV-PoPh, AH-PoPh were used for evaluation of hyoid bone position in the sagittal plane; in the vertical plane, the cephalometric distances evaluated were H-SN; H-FH; H-MP; H-PP; H-OP. The intraclass correlation coefficient (ICC) calculated from control group data to evaluate observer reliability was 0.91. Statistical analysis performed using one-way ANOVA and Tukey's test at a 5% level of significance.
Results
No significant statistical differences were found for the position of the hyoid bone in individuals with Angle Class II Division 1 malocclusion, in both sagittal and vertical planes, when comparing all the facial types. When the groups of individuals with Angle Class I and II malocclusion were compared, differences were statistically significant in relation to the following vertical measurements H-SN; H-FH; H-PP; H-OP. However, there was no significant statistical difference for the H-MP cephalometric distance. Considering the sagittal measurements, only the distance ANS-PNS differed statistically between the groups.
Conclusion
In accordance with the absence of statistical differences among the facial types, it appears that an adaptation of the tegumentary tissue exists around the hyoid bone.
Indexing terms: Cephalometry. Hyoid bone. Malocclusion, Angle Class II. Orthodontics. Tongue.
RESUMO
Objetivo
Localizar o osso hióide no sentido sagital e vertical, nos três tipos faciais (braquifacial, mesofacial e dolicofacial), em indivíduos com maloclusão Classe II, divisão 1 de Angle, comparando-os a um grupo controle com oclusão clinicamente normal.
Métodos
Foram utilizadas telerradiografias de cabeça em norma lateral de 45 indivíduos com maloclusão Classe II divisão 1 (grupo experimental) melanodermas, selecionados do arquivo científico da Faculdade São Leopoldo Mandic. Como grupo controle, foi utilizada uma amostra de 22 indivíduos melanodermas com oclusão clinicamente normal, selecionada do mesmo arquivo. Foram avaliadas as grandezas cefalométricas para a determinação do posicionamento sagital do osso hióide: ENA-ENP, ENA-PH, PT-PoPh, BV-PoPh, AH-PoPh e para a avaliação do posicionamento vertical do osso hióide: H-SN; H-FH; H-MP; H-PP; H-OP. A fim de estimar a reprodutibilidade do operador, foi utilizado o Coeficiente de Correlação Intraclasse (CCI), a partir dos dados do grupo controle, e o valor obtido foi 0,91, considerado ótimo. As análises estatísticas utilizadas foram: teste t, ANOVA e Tukey, com nível de significância de 5%.
Resultados
Não houve diferença estatisticamente significante no posicionamento do osso hióide, tanto no sentido sagital como no vertical, nos indivíduos melanodermas de Classe II divisão 1, comparando os tipos faciais. Quando foram comparados os grupos com maloclusão Classe I e II, os resultados mostraram uma diferença estatisticamente significante quanto às medidas verticais: H-SN; H-FH; H-PP; H-OP. Já com relação à medida H-MP, não houve diferença significativa. Quanto às medidas sagitais, somente ENA-ENP apresentou diferença significante entre os dois grupos.
Conclusão
A ausência de diferença estatística entre os tipos faciais sugere haver uma característica adaptativa dos tecidos tegumentares ao redor do osso hióide.
Termos de indexação: Circunferência craniana. Osso hióide. Má oclusão de Angle Classe II. Ortodontia. Língua.
INTRODUCTION
According to Berquó1, the mixed-race population has been growing and, when we add this group to the black population, the numbers are almost identical to those of the white population. Given these Figures, Brazil would be close to being defined as a primarily black nation, which clearly creates a current need to study samples of dark-skinned individuals. According to the author, color is a piece of selfidentification information that is as important as age and gender.
Lee et al.2 investigated to see if the variations in gender and ethnicity existed in measurements of the tegumentary and skeletal tissues, by way of a cephalometric analysis. They concluded that, in dark-skinned individuals, the SNA angle was greater than in Caucasians and, with SNB values, dark-skinned individuals and Hispanics showed the highest values, when compared to the Caucasian group.
The position of the hyoid bone in individuals with malocclusion and with normal occlusion has been studied and, according to Stepovich3, the position of the hyoid bone varies with the movement of the head and lower jaw, and also with functional movements such as chewing, swallowing, breathing and phonation; in cases of atypical swallowing, the hyoid bone seems to be positioned differently when compared to cases of typical swallowing.
Yamaoka et al.4 observed that the position of the hyoid bone is influenced by the position of the genioglossus muscle, which leads us to believe it is important to evaluate the position of the hyoid bone in relation to the tongue at the beginning of orthodontic treatment so that, during this treatment, its position may be directed. Based on the studies of various authors, and even with the limitations of lateral teleradiography of the head, which only displays two dimensions, the size of the tongue may be evaluated as well as its position in relation to other structures, the hyoid bone, lower jaw and upper pharynx.
Ferraz et al.5 observed that the position of the hyoid in Angle class I, II, III malocclusions, is the reflection of the strain in the muscles, ligaments and fascia.
The functions of the tongue and lower jaw muscles alter craniofacial growth and development. The study of the location, shape and function of the hyoid bone in Angle Class I, II, III individuals is important since the hyoid bone, supported by muscle, does not have a bone connection with the skull and the lower jaw, its position being dependent on the equilibrium of the surrounding tegumentary tissue6.
The position of the hyoid bone may be an important guide to diagnosis as the malocclusion could be caused by deleterious oral habits such as atypical swallowing and mouth breathing7. According to the author, if the hyoid bone stays in the same position both before and after the orthodontic treatment, there could be a reduced chance of reversion, on account of the tissue forces surrounding it. However, if the position of the hyoid bone is altered, a lengthy use of retainers might be recommended.
Given the above, the aim of this study was to evaluate the position of the hyoid bone in dark-skinned individuals with Angle Class II division 1 malocclusion, for the three facial types (brachyprosopic, mesoprosopic and dolichoprosopic), and to compare these with a control group with clinically normal occlusion which has not been subjected to orthodontic treatment.
The aim of the present study was to evaluate dark-skinned individuals by way of an analysis of lateral teleradiography of the head: a) to compare the position of the hyoid bone in the sagittal plane in individuals with clinically normal occlusion and Class II div.1 occlusion (control group and experimental group); b) check for the presence of differences in the vertical position of the hyoid bone between the two groups studied; c) to compare the position of the hyoid bone in the sagittal and vertical planes in individuals with Class II division 1 malocclusion (experimental group) for the different facial types.
METHODS
This research study was approved by the Ethics & Research Committee of the São Leopoldo Mandic Orthodontic Research Center, under filing no. 038709, in accordance with directives for the protection of research participants, established by Resolution 196/96 of the Ministry of Health's National Health Board.
The experimental group consisted of 45 darkskinned individuals, selected from the São Leopoldo Mandic Orthodontic Research Center scientific archives, in an age range between 8 and 15, in which 27 were male and 18 female, and with Angle Class II division 1 malocclusion. Lateral teleradiographs of the head were taken in the natural head position.
The group was divided as follows: 19 individuals with a mesoprosopic pattern, 9 brachyprosopic and 17 dolichoprosopic.
For the control group, a sample of 22 dark-skinned individuals was established with clinically normal occlusion, also selected from the scientific archives of the São Leopoldo Mandic Faculty; lateral teleradiographs of the head were taken for these subjects.
Sample inclusion criteria of individuals in Class II, division 1
a) Male and female, dark-skinned subjects aged between 8 and 15 - with Angle Class II division 1 malocclusion ascertained from the ANB angle (Riedel8)≥4.5º; b) mixed or permanent dentition; c) absence of extensive carious lesions; d) absence of radiographic distortions; e) individuals with the following facial types: mesoprosopic: evaluated using the cephalometric value SNGoGN (Steiner9) - angle computed from the intersection of the SN lines with the GoGN line, considered to be mesoprosopic in the range 32˚±4˚; dolichoprosopic: evaluated by the SNGoGN value of >36˚; brachyprosopic: evaluated using the measurement SNGoGN<28˚.
Sample inclusion criteria of individuals with Angle Class I occlusion
a) male and female dark-skinned individuals aged between 8 and 15; b) Class I molar relation; c) Positive ANB angle < 4.5º (Riedel8); d) mixed or permanent dentition; e) clinically normal occlusion.
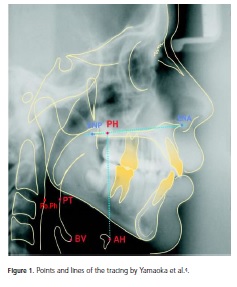
The cephalograms were manually charted by one researcher, twice at an interval of 10 days, in accordance with the methodology prescribed by Midtgard et al.10. The SNA, SNB, ANB, SNGoGN cephalmometric values used in the sample selection were acquired. The analysis to define the horizontal positioning of the hyoid bone was based on the work of Yamaoka et al.4 (Figure 1); the following points were defined: point AH: representing the most anterior superior point of the body of the hyoid bone; point PH: representing the point of intersection between the line ENA-ENP and the perpendicular line running from the most anterior superior point of the body of the hyoid bone (AH) to the extension of the line ENA--ENP; point PT: representing the rearmost point of the tongue contour, formed by a depression which, in radiographic terms, is situated below the mandibular rim, between the 2nd and 3rd cervical vertebra; point BV: representing the posterior point of the base of the epiglottis; point Po. Ph: representing the posterior wall of the pharynx.
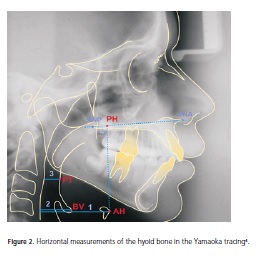
Horizontal values4 (Figure 2): a) perpendicular line from point AH to the posterior wall of the pharynx (PoPh); b) perpendicular line from point BV to the posterior wall of the pharynx (PoPh); c) perpendicular line from point PT to the posterior wall of the pharynx (PoPh); d) line of extension ENA-ENP with point AH, forming a perpendicular with point PH.
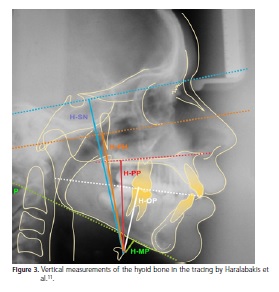
As a guide, the evaluation of the vertical positioning of the hyoid bone used the work of Haralabakis et al.11 (Figure 3): H-SN: distance from the hyoid bone ( M o s t anterior superior H-point of the hyoid bone) in the direction of the sella turcica perpendicular to the plane SN; H-FH: distance from the hyoid bone to the Frankfurt plane; H-PP: distance from the hyoid bone to the palatal plane; H-MP: distance from the hyoid bone to the mandibular plane; H-OP: distance from the hyoid bone to the occlusal plane.
All of these distances were obtained from the angle measurement of the right perpendicular with the planes SN, PP, FH, OP.
As a guide, the evaluation of the vertical positioning of the hyoid bone used the work of Haralabakis et al.11 (Figure 3): H-SN: distance from the hyoid bone (Most anterior superior H-point of the hyoid bone) in the direction of the sella turcica perpendicular to the plane SN; H-FH: distance from the hyoid bone to the Frankfurt plane; H-PP: distance from the hyoid bone to the palatal plane; H-MP: distance from the hyoid bone to the mandibular plane; H-OP: distance from the hyoid bone to the occlusal plane.
All of these distances were obtained from the angle measurement of the right perpendicular with the planes SN, PP, FH, OP.
Statistical methodology
Equipped with the values of each variable, we proceeded to calculate the means and standard deviations for each parameter, followed by a statistical comparison. With the aim of estimating the reproducibility of the operator, based on data from the control group, the Intraclass Correlation Coefficient (ICC) was used. In comparing the measurements of the control group and experimental group, the (unpaired) Student t test was employed.
A significance level of 5% was set for all the analyses. For comparisons of the hyoid bone and the mesoprosopic, brachyprosopic and dolichoprosopic facial types, the variance analysis (ANOVA) was used, followed by the Tukey test.
RESULTS
For the evaluation of operator error, based on data from the control group, the Intraclass Correlation Coefficient (ICC) was used, achieving, as a result, an ICC = 0.91.
The results of the present study are listed in "mm" in the Tables below (1 to 4).
The facial types of the individuals in the experimental group (Angle Class II division 1 malocclusion) were compared according to the horizontal and vertical positioning of the hyoid bone, with results computed in Tables 1 and 2.
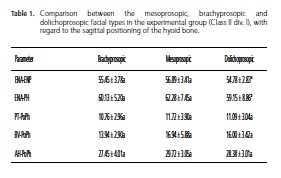
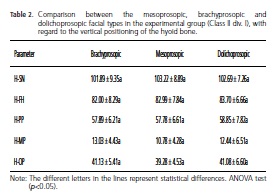
By means of the results obtained, as described above, the absence of statistically significant differences can be seen with the measurements related to the positioning of the hyoid bone and facial types.
The results from the comparison of the sagittal and vertical positioning of the hyoid bone, between the experimental group (Class II div. 1) and the control group (Class I), are exhibited in Tables 3 and 4 below:
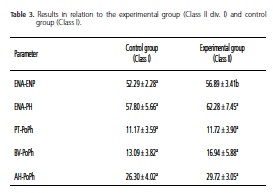
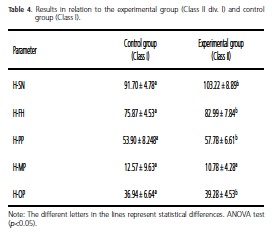
In the results described in tables 3 and 4, it may be considered that there were statistically significant differences for the following parameters: H-SN (p=0.004), H-FH (p=0.0043), H-PP (p=0.0021), H-OP (p=0.044) and ENA-ENP (p=0.004); as for the measurements ENA-PH, PTPoPh, BV-PoPh, AH-PoPh and H-MP, the difference was not significant (p>0.005) as, from the vertical parameters, the hyoid bone was positioned further down in Class II div.1 individuals.
DISCUSSION
With regard to the position of the head, in radiographic terms, Stepovich3 argued that perhaps, due to the position of the head not being totally controlled, in most cases the position of the hyoid bone cannot be duplicated on radiographic film in one and the same individual. Malkoc et al.12 observed that the airway dimensions, the position of hyoid bone and tongue are reproducible in successive radiographs, if greater attention is paid to the reproducibility of the head position. Rocabado13 presented a cephalometric method which enabled the interaction between the skull, cervical column, lower jaw and hyoid bone as a functional biomechanical unit, provided that these variables are taken into account, concluding that the hyoid bone depends more on the cervical curvature than on the mutual craniocervical relationship.
According to Kuroda et al.6, Adamidis& Spyropoulos14, Galvão15, Haralabakis et al.11 and Yamaoka et al.4, the position of the hyoid bone may vary according to the different malocclusions. Studying the position of the hyoid in Angle Class I, II, III malocclusions, Stepovich3 reported that its position is a reflection of the relative strain of the mutually interconnected muscles, ligaments and fascias, considering the position of the hyoid bone to be constant in the three types of malocclusion, suggesting that it is the musculature and not the occlusion of the teeth that determines the position of the hyoid bone.
Kuroda et al.6, observed significant differences in the position of the hyoid bone in relation to the cranial base (HNS), between the Angle Class I, II div.1 and Class III groups. The body of the hyoid bone was located a little to the rear in relation to the base of the skull in Class II, and a little to the front in the Class III group, when compared with the Class l group; as regards the lower jaw, the position of the hyoid bone was constant in the three groups. They are in agreement in their studies, when they relate the dental Classes with the sagittal position of the hyoid bone; Adamidis & Spyropoulos14, who ascertained that in individuals with Class III malocclusion, the hyoid bone tended to remain in a more forward position, mainly in male individuals. The authors concluded that the hyoid bone is altered by the whole craniofacial complex and that the function of the suprahyoid and infrahyoid muscles plays a part in establishing the direction of mandibular growth; Abu Allhaija & Al-Khateeb16 noted differences in dimensions of the pharynx, in skeletal Class I and III individuals, in the position of the hyoid bone and the width of the air space of the pharynx, an important though weak correlation with the change in the ANB angle. In the present study, it was possible to observe that the position of the hyoid bone, between Angle Classes I and II, showed no significant difference in the ENA-PH sagittal relation (table 3) and the only statistically relevant difference was the ENA-ENP measurement, (table 4). The results of this study are in agreement with Stepovich3, who found no difference in the anterior posterior positioning amongst the malocclusions studied. When the position of the hyoid bone is related to the different facial types, Ingervall17 argued that the lower jaw movements between the intercuspal position and the normal position, associated with the movement of the hyoid bone, are correlated with the facial and dental morphology. There was a significant negative correlation between the movement of the hyoid bone and the movement of the lower jaw from the intercuspal to the normal position, if the height of the face is short, the hyoid bone moved further down and if it is long, the hyoid bone moved upwards. In addition, Opdebeeck et al.18, when studying individuals with short face syndrome (SFS) and long face syndrome (LFS) via the distance between H1 and Me, observed that this was significantly lower in the LFS group than in the SFS group (H1.Me- 57.11 in the SFS, 44.02 in the LFS). Cuozzo& Bowman19; Gobeille & Bowman20; Tourné Luc21 observed the movement of the hyoid with the lower jaw, using lingual appliances. They found that all the individuals who adapted to the lingual appliance had displacement of the hyoid bone downwards and to the rear, and in the position of rest, the hyoid bone was close to the mandibular rim. This displacement may have occurred via tongue stimulus, caused by the lingual appliance, being instrumental in maintaining the passage of air at the level of the base of the tongue, in agreement with the studies of Opdebeeck et al.18 which state that the rotation of the hyoid bone has an influence on the position of the tongue.
In the present study, the groups were evaluated in the intercuspal position, with no significant difference being registered amongst the facial types, in the positioning of the hyoid bone, with both horizontal and vertical measurements (Tables 1 and 2). However there was agreement with Opdebeeck et al.18 when it came to observing that the hyoid bone moves in conjunction with the lower jaw and the pharynx, which might suggest as the outcome observed in this study, when the non-existence of significant differences in the measurements PT-PoPh, BVPoPh, AH-PoPh, (Table 3) was confirmed, and by means of measurement (H-MP), (Table 4).
As regards the vertical position of the hyoid bone, Galvão15 concluded that in Class II individuals, via the linear measurement (PNS-H), the hyoid bone is situated a little above and close to the mandibular rim, while in the Class III malocclusion group, it is to be found lower down and further away from the mandibular rim; Haralabakis et al.11 investigated adult individuals with open bite by comparing them to a control group with Class I and concluded, using vertical measurements, that only the distance from the hyoid bone to the palatal plane (H-PP) was seen to be significantly greater in male individuals with open bite, due to the position of the palatal plane in the development of this dento-skeletal malocclusion. The authors' results suggest that the hyoid bone moves in conjunction with the pharynx, cervical column, mandibular plane and the tongue in individuals with different skeletal types. In addition, Kollias & Krogstad22 conducted a longitudinal investigation into alterations in the craniofacial morphology and the position of the hyoid bone, at intervals of 10 years, revealing that, with age, the hyoid bone assumed a lower position when related to the AH-S, AH-FH, AH-C3, in both sexes. In this study, as regards the vertical position of the hyoid bone, there was also agreement with the abovementioned authors in relation to the parameters H-SN, H-FH, H-PP (table 4), which demonstrated a statistically significant difference between Angle Classes I and II, as in Class II individuals, the vertical location of the hyoid bone was lower, though in relation to parameter H-MP there was no statistical difference. It seems that the hyoid bone accompanies the movement of the lower jaw.
As regards the hyoid bone relationship with the posterior wall of the pharynx, Hellsing23, Muto et al.24, by way of lateral teleradiography of the head, evaluated the pharynx and neighboring structures in different head postures, and concluded that the level of increase in the airway of the pharynx depends on how the individual extends his head. Valenzuela et al.25, however, showed that there was no relevant association between head posture and the anterior posterior position of the head, the anterior posterior position of the hyoid bone and the vertical position of the hyoid bone. Smith & Battagel26, meanwhile, demonstrated that the change in the individual, from standing position to supine, resulted in a reduction in the oropharyngeal space, and in the supine position, with protrusion of the lower jaw, this space increased. Nevertheless, when the relationship of the hyoid bone with the oropharynx is studied in individuals with natural head posture (NHP), the studies by Solow & Tallgren27, Kollias& Krogstad22 and Yamaoka et al.4 demonstrated that there was no statistical difference in the horizontal parameter of the hyoid bone with the oropharynx, nor did the size of the latter change. In the present study, there was agreement with the abovementioned authors that the oropharynx remains constant in terms of the parameters ENA-PH, PTPoPh, BV-PoPh, AH-PoPh presented in Tables 1 and 3.
The lack of statistically significant difference between the facial types suggests there is a neuromuscular adaptive pattern in the tegumentary tissues around the hyoid bone.
CONCLUSION
Considering the methodology employed and the meticulous analysis of the data presented, it was possible to conclude that, as far as the vertical position of the hyoid bone is concerned, the values H-SN, H-FH, H-PP and H-OP are higher for Class II malocclusion patients than for those in Class 1 and, as regards the facial types in the experimental group (brachyprosopic, mesoprosopic, and dolichoprosopic),there was no statistically significant difference of the hyoid bone in the sagittal relationship nor in the vertical relationship.
Collaborators
EN CARVALHO, DF NOUER, IU GARBUI and PRA NOUER took part in all stages of the preparation of this article.
REFERENCES
1. Berquó E. Jornal da rede feminista de saúde [citado 2008 Maio 10]. Disponível em: <http://www.redesaude.org.br/home> [ Links ].
2. Lee JJ, Ramirez SG, Will MJ. Gender and racial variations in cephalometric analysis. Otolaryngol Head Neck Surg.1997;117(4):326-9. doi: 10.1016/S0194-5998(97)70121- 9. [ Links ]
3. Stepovich ML. A cephalometric positional study of the hyoid bone. Am J Orthodont. 1965;51(12):882.-90 [ Links ]
4. Yamaoka M, Furusawa K, Uematsu T, Okafuji N, Kayamoto D, Kurihara S. Relationship of the hyoid bone and posterior surface of the tongue in prognathism and micrognathia. J Oral Rehabil. 2003;30(9):914-20. doi: 10.1046/j.1365-2842.2003.01069.x. [ Links ]
5. Ferraz MJPC, Nouer DF, Teixeira JR, Berzin F. Avaliação cefalométrica da posição do osso hióide em crianças respiradoras bucais. Rev Bras Otorrinolaringol. 2007;73(1):47- 52. doi: 10.1590/S0034-72992007000100008. [ Links ]
6. Kuroda T, Nunota E, Hanada K, Ito G, Shibasaki Y. A roentgenocephalometric study on the position of the hyoid bone. Bull Tokyo Med Dent Univ. 1966;25(1):31-8. [ Links ]
7. Bibby RE. The hyoid bone position in mouth breathers and tongue-thrusters. Am J Orthod. 1984;85(5):431-3. doi: 10.1016/0002-9416(84)90164-7. [ Links ]
8. Riedel RA. The relation of maxillary structures of cranium in malocclusion and in normal occlusion. Am J Orthod. 1952;22:142-5. [ Links ]
9. Steiner CC. Cephalometric for you and me. Am J Orthod. 1953;39(10):729-55. [ Links ]
10. Midtgard J, Bjork G, Linder-Aronson S. Reproducibility of cephalometric landmarks and errors of measurements of cephalometric cranial distances. Angle Orthod. 1974;44(1):56- 61. [ Links ]
11. Haralabakis NB, Toutountzakis NM, Yiagtzis SC. The hyoid bone position in adult individuals with open bite and normal occlusion. Eur J Orthod. 1993;15(4):265-71. doi: 10.1093/ ejo/15.4.265. [ Links ]
12. Malkoc S, Usumez S, Nur M, Donaghy CE. Reproducibility of airway dimensions and tongue and hyoid positions on lateral cephalograms. Am J Orthod Dentofac Orthoped. 2005;128(4):513-6. doi: 10.1016/j.ajodo.2005.05.001. [ Links ]
13. Rocabado, M. Relaciones biomecánicas de las regiones craneales, cervicales e hioideas. Ortodoncia. 2005;58(115):51-6. [ Links ]
14. Adamidis IP, Spyropoulos MN. The effects of lymphadenoid hypertrophy on the position of the tongue, the mandible and the hyoid bone. Eur J Orthod. 1983;5(4):287-94. doi: 10.1093/ejo/5.4.287. [ Links ]
15. Galvão CAAN. Estudo cefalométrico da posição do osso hióide em indivíduos com oclusão normal e portadores de maloclusão. Rev Odont UNESP. 1983;12(1/2):143-52. [ Links ]
16. Abu Allhaijaes E, Al-Khateeb SN. Uvulo-glosso-pharyngeal dimensions in different anteroposterior skeletal patterns. Angle Orthod. 2005;75(6):1012-8. [ Links ]
17. Ingervall B, Carlsson GE, Helkimo M. Change in localization of hyoid bone with mandibular positions. Acta Odontol Scand. 1970;28(3):337-61. [ Links ]
18. Opdebeeck H, Bell WH, Eisenfeld J, Mishelevich D. Comparative study between the SFS and LFS rotation as a possible morphogenic mechanism. Am J Orthod. 1978;74(5):509-21. doi: 10.1016/0002-9416(78)90026-X. [ Links ]
19. Cuozzo GS, Bowman DC. Hyoid positioning of the tongue. Am J Orthod. 1975;68(5):564-9. [ Links ]
20. Gobeille DM, Bowman DC. Hyoid and muscle changes following distal repositioning of the tongue. Am J Orthod. 1976;70(3):282- 9. [ Links ]
21. Tourné Luc PM. Growth of the pharynx and its physiologic implications. Am J Orthod Dentofac Orthop. 1991;99(2):129- 39. doi: 10.1016/0889-5406(91)70115-D. [ Links ]
22. Kollias I, Krogstad Ol. Adult craniocervical and pharyngeal changes, a longitudinal cephalometric study between 22 and 42 years of age. Part I: morphological craniocervical and hyoid bone changes. Eur J Orthod. 1999;21(4):333-44. doi: 10.1093/ejo/21.4.333. [ Links ]
23. Hellsing E. Changes in the pharyngeal airway in relation to extension of the head. Eur J Orthod. 1989;11(4):359-65. [ Links ]
24. Muto T, Takeda S, Kanazawa M, Yamazaki A, Fujiwara Y, Mizoguchi I. The effect of head posture on the pharyngeal airway space (PAS). J Oral Maxillofac Surg. 2002;31(6):579-83. doi: 10.1054/ijom.2002.0279. [ Links ]
25. Valenzuela S, Miralles R, Ravera MJ, Zúñiga C, Santander H, Ferrer M, et al. Does head posture have a significant effect on the hyoid bone position and sternocleidomastoid electromyographic activity in young adults? Cranio. 2005;23(3):204-11. [ Links ]
26. Solow B, Tallgren A. Natural head position in standing subjects. Acta Odontol Scand. 1971;29(5):591-607. [ Links ]
 Correspondence to:
Correspondence to:
PRA NOUER
Rua José Rocha Junqueira, 13, Swift, 13045-755, Campinas, SP, Brasil
e-mail: nouerp@gmail.com
Received on: 11/11/2008
Final version resubmitted on: 2/6/2009
Approved on: 14/6/2009
