










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.1 Porto Alegre Jan./Mar. 2013
ORIGINAL / ORIGINAL
Dental caries associated factors in 12 year-old schoolchildren from a municipality in the state of São Paulo, Brazil
Fatores associados à cárie dentária em escolares aos 12 anos em um município do estado de São Paulo, Brasil
Soraya Fernandes MESTRINERI; Monica Andrade MORRAYEII; Andrea Porto AGUILAII; Antonio Sergio FERRAUDOIII; Wilson MESTRINER JÚNIORI
I Universidade de São Paulo, Faculdade de Odontologia, Departamento de Clínica Infantil, Odontologia Preventiva e Social
II Universidade de Franca, Pós-Graduação em Promoção de Saúde. Franca, SP, Brasil
III Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Ciências Agrárias e Veterinárias de Jaboticabal. Jaboticabal, SP, Brasil
ABSTRACT
Objective
To analyze the possible association between dental caries, fluorosis and the need for treatment in 12 year-old schoolchildren and the socioeconomic conditions of parents/guardians in the city of Franca, in the state of São Paulo.
Methods
A random sample of schoolchildren aged 12 was obtained from the school records in Franca, using a systematic random technique. The epidemiological survey was carried out by a single calibrated examiner, on 258 public and private schoolchildren in order to obtain the prevalence of dental caries, the need for treatment and the severity of dental fluorosis. Parents/guardians were also interviewed to assess their socioeconomic conditions (education and per capita income). We used multiple correlation analysis to investigate associations between category variables.
Results
It was possible to identify two distinct groups, with associations between the variables: the first group, represented by schoolchildren with average prevalence of caries, need for treatment, low level of parental education and income; and a second group represented by schoolchildren with low prevalence of caries, no need for treatment, high parental education and income. The two dimensions explained approximately 35% of total inertia. The factors within each group are related.
Conclusion
High income and parental education are associated with the low prevalence of dental caries but there is no association with dental fluorosis.
Indexing terms: Dental caries. Dental fluorosis. DMF index. Epidemiology. Oral health. Socioeconomic factors.
RESUMO
Objetivo
Analisar as possíveis associações entre cárie dentária, fluorose e necessidade de tratamento de escolares aos 12 anos de idade e fatores sócio-econômicos dos pais ou responsáveis, no Município de Franca, São Paulo.
Métodos
Foi obtida uma amostra probabilística, através da técnica de sorteio ponderado de estabelecimentos de ensino do cadastro das escolas do município de Franca, cujos elementos amostrais foram identificados através da técnica casual sistemática. Os exames epidemiológicos foram realizados em 258 escolares de unidades de ensino público e privados, por um único examinador calibrado, para obtenção da prevalência de cárie, necessidade de tratamento e severidade da fluorose dental. Foram também realizadas entrevistas com os pais ou responsáveis para avaliação sócio econômica (escolaridade e renda familiar). Com base nesses dados foi realizada uma análise de correspondência múltipla para a busca das associações entre variáveis categóricas. Foi obtida uma amostra probabilística, através da técnica de sorteio ponderado de estabelecimentos de ensino do cadastro das escolas do município de Franca, cujos elementos amostrais foram identificados através da técnica casual sistemática. Os exames epidemiológicos foram realizados em 258 escolares de unidades de ensino público e privados, por um único examinador calibrado, para obtenção da prevalência de cárie, necessidade de tratamento e severidade da fluorose dental. Foram também realizadas entrevistas com os pais ou responsáveis para avaliação sócio econômica (escolaridade e renda familiar). Com base nesses dados foi realizada uma análise de correspondência múltipla para a busca das associações entre variáveis categóricas.
Resultados
A análise permitiu identificar dois grupos discrepantes, os quais possuem associações entre as variáveis: Grupo 1, escolares com prevalência média de cárie, baixa escolaridade dos pais, com necessidade de tratamento e baixa renda familiar; e Grupo 2, escolares com prevalência baixa de cárie, alta escolaridade dos pais, sem necessidade de tratamento e renda familiar média. As duas dimensões explicaram 35% aproximadamente da inércia total. Os fatores dentro de cada grupo estão associados.
Conclusão
A escolaridade e renda alta dos pais ou responsáveis estão associadas à baixa prevalência de cárie dentária e não há associação com a fluorose dentária.
Termos de indexação: Cárie dentária. Fluorose dentária. Índice CPO. Epidemiologia. Saúde bucal. Fatores socioeconômicos.
INTRODUCTION
Over the years, dental caries has been regarded as the primary problem in the field of social dentistry. This stems from its frequency, the seriousness of the damage caused, the possibility of effective action, the per capita cost of treatment and the level of interest of the public at large1.
Moreover, dental caries may have an adverse effect on the quality of life of a large number of people, causing pain and infection. Without proper treatment, it could even produce or aggravate other common illnesses as well as increase the financial burden on the health services2.
In the 1970s, studies considered dental caries to be a "democratic" disease affecting all classes of society indiscriminately3. The predominance was noted of components relating to the need for treatment in the least privileged layers of society, while in the population that enjoyed higher levels of income, with greater access to dental services, a predominance of already performed treatment was observed.
With the decline in the prevalence of caries disease, which occurred globally as from the end of the 70s and early 80s, this picture began to change. The epidemiological surveys subsequently carried out already demonstrate inequality of caries experience between the classes4. The experience of caries was reduced as a whole but there are still groups of individuals that present a large number of dental surfaces experiencing caries5. These people usually belong to the lower income strata of the population. The lower purchasing power involves a set of factors that relate to access to health services, level of education, lifestyle, conditions of hygiene, housing and access to products, amongst others6.
Significant transformations in living conditions occurred in particular regions of the globe in the 20th century. These changes are linked to the models of social and economic development engendered in each region. In many regions, there was wider access to treated water, growth in education and in services networks and an increase in income with better housing conditions and food. A variety of aspects, separately or in combination, have contributed to the transformations in the health conditions of human populations, changing both the population structure and the patterns of morbi-mortality7.
By describing and comparing the trends of manifestation of dental caries observed in each country, or even within one municipality, as is the case of this study, it allows us to explore connections between the rates of occurrence of this disease over the course of time and more general aspects linked to industrialization, human development, socioeconomic conditions and, consequently, to contribute to the refinement of social policies8.
METHODS
The reference population for the study comprised schoolchildren of 12 years of age from the municipality of Franca, in 2004. The city, with approximately 304,000 inhabitants, is situated in the northwestern region of the state of São Paulo, in Brazil. A total of 98% of households enjoy a system of treated, fluorinated water (0.7 to 1 ppm)9.
The study was approved by the Ethics in Research Committee at the University of Franca (filing no. 010/02B).
The study presents a prevalence study with a crosssectional, observational design. For the probability sample10, as the basis for calculating sample size, the variable "attack of dental caries" was adopted, measured via the CPO-D (better known as DMF-T in English-speaking countries) index (2.8) produced in Franca in 199811, considering a level of significance of 95%, a design effect equal to 2 and assuming a loss of 20%. The sampling units were drawn using the systematic sampling technique and the sampling elements were identified by applying systematic random sampling.
The epidemiological examinations of oral health condition were carried out on 256 schoolchildren by a calibrated dental surgeon using the codes and criteria advocated by the WHO12, and CPO_D index data were obtained, classified as Low (CPOD_B), with values between 0 and 3, Medium (CPOD_M), with values between 4 and 8 and High (CPOD_A), being greater than 8; the level of fluorosis, classified as Normal (FLU_N), Questionable (FLU_Q) and Light (FLU_L); and the need for treatment classified as Needs Treatment (TRAT_nece) or Does Not Need Treatment (TRAT_ñ nece).
The socioeconomic evaluation was obtained by means of interviews in which the oral healthcare questionnaire13 was used in which the variables included here were: level of education of parents/guardians and family income.
Level of education, represented by the number of years of study of the parents/guardians interviewed, was obtained based on the grade to which the individual was currently studying or had studied, taking into account the last grade completed and passed. The following categorieswere used: Low (ESC_0-4), parents/guardians with 0 to 4 years of study; Medium (ESC_5-8), between 5 and 8 years of study; and High (ESC_+9), 9 or more years of study.
The value used for monthly family income was the sum of the monthly earnings of all the components of the Family Unit. Income was designated by minimum salary. Monthly family income was classified as low income (RENDA_B), where income was between 0 and 4 minimum salaries; high income (RENDA_A), income greater than or equal to 8 minimum salaries; and average income (RENDA_M), between 4 and 8 minimum salaries.
The checking of intra-examiner agreement, Kappa coefficient, was obtained from the practice of examining, in duplicate, 10% of the epidemiological examination sample14.
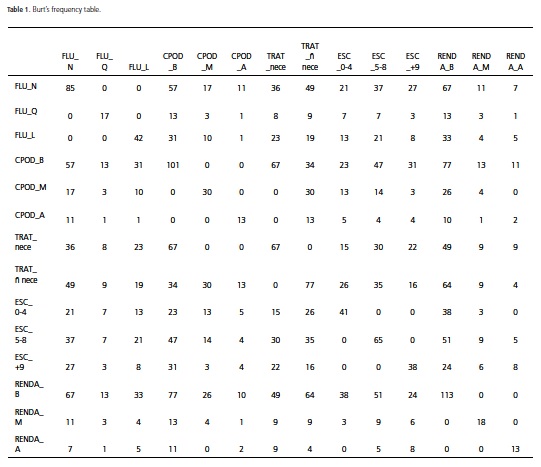
Multiple correspondence factor analysis (MCA) was employed to investigate the existence of an association between the category variables15 studied based on the table X'X, known as the Burt Table, which contains all frequencies related to the intersection of all categories of response from the records obtained. X is the original data matrix (Table 1). The line points and/or column resulting from the association between the variables in table X are displayed in two-dimensional maps called perceptual maps which facilitate the viewing of relationships that exist between the variables. The quality of the perceptual maps is measured by the values of inertia retained in each eigenvalue responsible for the generation of the individual dimensions. The analyses were processed using the software application Statistica® version 7.
RESULTS
Of the 300 schoolchildren drawn out, an epidemiological exam was performed on 256 of them, representing 85.33% of schoolchildren drawn and a loss of 14.67%.
The intra-examiner agreement percentages obtained in the epidemiological examination of the dental caries condition was 99% and the Kappa Coefficient was 0.98.
The average CPOD in the 12 year-old index was 1.69 (ranging from 1.41 to 1.96), confidence interval of 95% for the population average. The percentage of schoolchildren without caries was 46.06% and the prevalence of caries in the studied population was classified as "low".
Interviews were carried out with the parents/guardians of 144 of the schoolchildren taking part in the study. The average age of the parents/ guardians was 40 (sd = 7.42), 90% being between 30 and 50 yearsold. The average number of years of schooling of the parents/guardians was 6.9; 17.4% were still studying. Approximately 78.47% of interviewees had an average family income of between 1 and 4 minimum salaries; 12.5% between 4 and 7; and 9.2% had income of 8 or more minimum salaries.
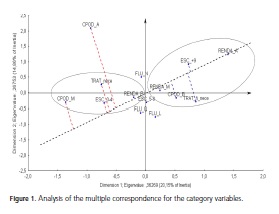
Figure 1 shows the graphical representation of the MCA in a two-dimensional plane. A clear division can be noted into two groups of variables, guided by the distance between the points that represent the category variables.
In Figure 1, a pseudo diagonal was constructed passing through the center of dimensions 1 and 2 and RENDA_A. By projecting the points on the perceptual map on to this diagonal, two contrasting groups can be observed, as follows: GROUP 1 (CPOD_M, ESCO_0-4, TRAT_nece and RENDA_B) and GROUP 2 (RENDA_A, ESC_+9, TRAT_ñ nece, RENDA_M and CPO_B). The factors within each group are connected. The most extreme factors (most inert) possess greater discriminatory power (RENDA_A, CPOD_M, CPOD_A). The two dimensions corresponded approximately to 35% of the total inertia contained in the original data. Although the value seems low, it was possible to explain the associations between factors.
DISCUSSION
Epidemiological studies16-17 have obtained percentages of overall intra-examiner agreement and a Kappa index similar to those observed in this study, values which are considered by Landis & Kock18 to be a near perfect agreement, which demonstrates a high degree of reproducibility in relation to the CPOD and affords a guarantee of statistical reliability to the results.
The prevalence of caries is low in 12 year-old schoolchildren in the municipality of Franca, similar to that in other cities in Brazil17 and comparable to that found in industrialized countries; a continuing decline in caries has been observed; in 199811, the average CPOD was 2.8. According to Pine et al.19, the decline in the prevalence of caries has been accompanied by changes that have occurred in the pattern and distribution of the disease.
The decline in the prevalence of dental caries amongst children and adolescents has been reported in various studies19-20; however individuals in this age range still display high caries values; this is known as the polarization phenomenon. There needs to be, therefore, a honing of oral healthcare strategies aimed at these groups19.
The uneven distribution of dental caries can be seen even in countries with a low prevalence of caries, whose CPOD values are considered by the WHO to be very low (CPOD at 12 years of age ≤ 1.2)21. In addition, studies have been finding significant associations between social, economic, behavioral and environmental variables and the experience of caries, in socially deprived individuals and areas22-23.
These differences are being well reported by various authors and they characterize significant inequality in health that requires the attention of the authorities and adequate public health intervention8.
The association between socio-economic drivers and the presence of dental caries6,16,24-25, amongst others, has shown that the worst conditions of oral health cannot be divorced, in particular, from the disparity in incomes and the level of schooling, factors which are indicative of social levels25-26.
Taking into consideration the socioeconomic aspects, in a study conducted with schoolchildren of 7, 12 and 14 years of age in the city of Ceuta (Spain), the prevalence of caries in schoolchildren of a low socioeconomic level and with the father unemployed, was 1.8 times greater than in schoolchildren with working parents16. For Peres et al.25, family income was the most relevant socioeconomic factor. Children whose family income was less than 5 minimum salaries were 4.18 times more likely to present with a high severity of caries when compared to those who had a family income above 5 minimum salaries. In the population studied in the municipality of Franca (in the state of São Paulo), we found a greater correspondence between high family incomes and levels of schooling of parents/guardians and low prevalence of caries.
However, in a study carried out with 1,000 schoolchildren in Porto Alegre, a local association was observed between schoolchildren with more than four affected surfaces and parents who did not complete primary education. Schoolchildren without caries were locally associated with parents who had completed higher education, as observed in the present study.
Moreover, for Pine et al.26, in a large-scale study conducted in Europe, North America, Africa and Asia, the level of understanding and the attitudes of parents in relation to their own oral health and that of their children is associated with the chances of their children developing caries.
The present study, as with that by Meneghim et al.27, on evaluating the relationship between socioeconomic classification and the prevalence of caries and dental fluorosis in Piracicaba, São Paulo, Brazil, only found, with regard to socioeconomic class, a statistically significant association with dental caries.
In a more recent study, also conducted in the municipality of Piracicaba, Pereira et al.26 concluded that socioeconomic variables are only associated with a greater prevalence of the disease at an individual level.
The decline in the prevalence of caries in Franca could also be associated with the use of fluorides, bearing in mind that 98% of households in the municipality have access to treated, fluoridated water28.
Peres et al.29, comparing the indices of caries in districts with treated, fluoridated water, in Brazil, with those of districts that do not have this resource, concluded that the fluoridated water was related to an improvement in the indices of caries and, accordingly, it is considered to be an effective strategy for the control of the disease.
According to Balbani et al.16, upon analyzing the relationships between dental caries and socio-economic factors in the Brazilian state of Paraná, it was noted that the higher the percentage of households connected to the fluoridated water system, the lower the CPO-D values in the municipalities; in this regard, the importance of this benefit was underscored, not only as a resource for the reduction of levels of caries, but also to soften the impact of socioeconomic inequalities on the prevalence of dental caries.
For Maltz & Barbachan6, however, there are few studies that discuss the relationship of prevalence of fluorosis and socioeconomic levels and these generally present conflicting results. In theory, as fluorosis is the result of the combined effects of diverse sources of fluorine, the population with greater access to fluoridated products could present with a higher prevalence of fluorosis, irrespective of socioeconomic levels and the level of schooling of parents, as observed in this study. Similar results were reported by other authors16-17,30, who attribute to this measure, the ability to substantially reduce the negative impact of socioeconomic equality on the prevalence of dental caries, even though, notwithstanding, they are not able to neutralize them.
CONCLUSION
Advanced levels of education and high incomes of parents/guardians are associated with a low prevalence of dental caries and the absence of required treatment; however no association was found with dental fluorosis.
The population in this study presented a low level of dental caries, however, inequalities can be observed and they are associated with socioeconomic conditions; this requires the attention of the authorities and adequate public health strategies.
We would emphasize the need for complementary studies to check for the presence of correlation in areas with greater social privation that exist in the municipality.
Collaborators
SF MESTRINER, MA MORRAYE, AP AGUILA and W MESTRINER JÚNIOR took part in all stages of the preparation of the article. AS FERRAUDO participated in the statistical analysis, interpretation of data and the composition of the article.
REFERENCES
1. Chaves MM. Odontologia social. 3rd ed. Rio de Janeiro: Artes Médicas; 1986. [ Links ]
2. Murray JJ. O uso correto de fluoretos na saúde pública. São Paulo: Editora Santos; 1992. [ Links ]
3. Barmes DE. Features of oral health care across cultures. Int Dent J. 1976;26(3):353-68. [ Links ]
4. Al-Mohammadi SM, Rugg-Gunn AJ, Butler TJ. Caries prevalence in boys aged 2, 4 and 6 years according to socio-economic status in Riyadh, Saudi Arabia. Community Dent Oral Epidemiol . 1997;25(2):184-6. doi: 10.1111/j.1600-0528.1997.tb00920.x. [ Links ]
5. Burt BA. Prevention policies in the light of the changed distribution of dental caries. Acta Odontol Scand.1998;56(3):179-86. [ Links ]
6. Maltz M, Barbachan BS. Relação entre cárie, gengivite e fluorose e nível socioeconômico em escolares. Rev Saúde Pública. 2001;35(2):170-6. doi: 10.1590/S0034-89102001000200011 [ Links ]
7. Pereira AC. Odontologia em saúde coletiva: planejando ações e promovendo saúde. Porto Alegre: Artmed; 2003. [ Links ]
8. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cárie dentária no Brasil: declínio, polarização, iniqüidade e exclusão social. Rev Panam Salud Pública. 2006;19(6):385-93. doi: 10.1590/S1020-49892006000600004. [ Links ]
9. São Paulo (Estado). Prefeitura Municipal de Franca. Plano Municipal de Saúde [citado 2004 Abril 25]. Disponível em: <www.franca.sp.gov.br> [ Links ].
10. Silva NN. Amostragem probabilística. São Paulo: Edusp; 1998. [ Links ]
11. São Paulo (Estado). Secretaria de Estado da Saúde. Faculdade de Saúde Pública da Universidade de São Paulo. Levantamento epidemiológico em saúde bucal, Estado de São Paulo (SP) - 1998: relatório. São Paulo: Universidade de São Paulo; 1999. [ Links ]
12. WHO. Oral health surveys: basic methods. Geneva: World Health Organization; 1997. [ Links ]
13. Brasil. Ministério da Saúde. Secretária de Políticas de Saúde, Departamento de Atenção Básica, Área Técnica de Saúde Bucal. Projeto SB 2000: condições de saúde bucal da população brasileira no ano de 2000: manual do examinador. Brasília: Ministério da Saúde; 2001. [ Links ]
14. Hair JF, Anderson RE, Tatham RL, Black W. Análise multivariada de dados. 5ª ed. Porto Alegre: Bookman; 2005. [ Links ]
15. García VMN, García MAN, Remigio JRL, Martín LA. Salud oral de los escolares de Ceuta. influencias de la edad, el género, la etnia y el nivel socioeconómico. Rev Esp Salud Pública. 2001;75:541-
9.
16. Baldani MH, Narvai PC, Antunes JLF. Cárie dentária e condições sócio-econômicas no Estado do Paraná, Brasil, 1996. Cad Saúde Pública. 2002;18(3):755-63.1 [ Links ]
17. Landis WJ, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-74. [ Links ]
18. Ruiz LA, Rihs LB, Sousa MLR, Hildebrand L, Felizatti RC. Declínio da cárie dentária em escolares entre 1998 e 2004 em Leme, São Paulo, Brasil. RGO - Rev Gaúcha Odontol. 2009;57(2):145-50. [ Links ]
19. Pine C, Burnside G, Craven R. Inequalities in dental health in the North-West of England. Community Dental Health. 2003;20(1):55-6. [ Links ]
20. Pitts NB, Evans DJ, Nugent ZJ, Pine CM. The dental caries experience of 12-year-old children in England and Wales. Surveys coordinated by the British Association for the Study of Community Dentistry in 2000/2001. Community Dental Health. 2002;19:46-53. [ Links ]
21. Campus G, Lumbau A, Lai S, Solinas G, Castiglia P. Socioeconomic and behavioural factors related to caries in twelveyear-old Sardinian children. Caries Res. 2001;35(6):427-34. [ Links ]
22. Nicolau B, Marcenes W, Bartley M, Sheiham A. Associations between socio-economic circumstances at two stages of life and adolescents' oral health status. J Public Health Dent. 2005;65(1):14-20. [ Links ]
23. Peres KGA, Bastos JRM, Latorre MRO. Severidade de cárie em crianças e relação com aspectos sociais e comportamentais. Rev Saúde Pública. 2000;34(4):402-8. doi: 10.1590/S0034-89102000000400014. [ Links ]
24. Fadel CB, Saliba NA. Aspectos sócio-dentais e de representação social da cárie dentária no contexto materno-infantil. RGO - Rev Gaúcha Odontol. 2009;57(3):303-9. [ Links ]
25. Peres MA, Peres KG, Traebert J, Zabot NE, Lacerda JT. Prevalence and severity of dental caries are associated to the worst socioeconomic conditions: a Brazilian cross-sectional study among 18-year old males. J Adolesc Health. 2005;37(2):103-9. doi: 10.1016/j.jadohealth.2004.08.016. [ Links ]
26. Pine CM, Adair PM, Nicoll AD, Burnside G, Petersen PE, Beighton D. International comparisons of health inequalities in childhood dental caries. Community Dental Health. 2004;21(Supplement):121-30. [ Links ]
27. Meneghim MC, Kozlowski FC, Pereira AC, Ambrosano GMB, Meneghim ZMAP. Classificação socioeconômica e sua discussão em relação à prevalência de cárie e fluorose dentária. Ciênc Saúde Coletiva. 2007;12(2):523-9. doi: 10.1590/S1413- 81232007000200028. [ Links ]
28. Brasil. Ministério da Saúde. DATASUS. 2004 [citado 2004 Jul 20]. Disponível em: <http//www.datasus.gov.br> [ Links ].
29. Peres MA, Antunes JLF, Peres KG. Is water fluoridation effective in reducing inequalities in dental caries distribution in developing countries? Recent findings from Brazil. Soz Preventivemed. 2006;51(5):302-10. [ Links ]
30. Jones CM, Worthington H. Water fluoridation, poverty and tooth decay in 12-year-old children. J Dent. 2000;28(6):389-93. doi: 10.1016/S0300-5712(00)00005-1. [ Links ]
 Correspondence to:
Correspondence to:
SF MESTRINER
Av. Bandeirantes, 3900, Monte Alegre, 14040-900, Ribeirão Preto, SP, Brasil
e-mail: somestri@forp.usp.br
Received on: 8/9/2009
Final version resubmitted on: 4/1/2010
Approved on: 12/4/2010
