










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.1 Porto Alegre Jan./Mar. 2013
ORIGINAL / ORIGINAL
Radiographic prevalence of unerupted and supernumerary teeth
Prevalência radiográfica de dentes não irrompidos e supranumerários
Vanessa Bobig dos SANTOSI; André Barbisan de SOUZAII; Vitor Marques SAPATAII; Giovani de Oliveira CORREAI; Fabiano Carlos MARSONI; Cléverson de OLIVEIRA E SILVAI
I Faculdade Ingá, Curso de Odontologia
II UUniversidade Estadual de Maringá, Curso de Odontologia. Maringá, PR, Brasil
ABSTRACT
Objective
The objective of this study was to evaluate the prevalence of unerupted third molars and supernumerary teeth in patients from Maringá and region.
Methods
Panoramic radiographs of patients treated in the Dental Clinic at Ingá School of Dentistry during 2009, were evaluated. The third molars were classified according to Pell and Gregory1 and Winter2 and the supernumerary teeth according to Garvey et al.3. The results were submitted to chi-square statistical testing (p<0.05).
Results
Of a total of 411 panoramic x-rays evaluated, 113 subjects had unerupted third molars and 5 patients had supernumerary teeth. For the maxillary third molars the highest prevalence was in the A vertical position (p<0.05), and for mandibular third molars it was the mesio-angular position, class 1A (p<0.05). As for the supernumerary teeth, three were canines and two incisors, 2 being in the normal position, 2 inclined and 1 inverted.
Conclusion
Based on the outcomes of the present study, it can be concluded that there is a high prevalence of unerupted third molars and a low prevalence of supernumerary teeth in the studied population.
Indexing terms: Impacted tooth. Oral surgery. Supernumerary tooth.
RESUMO
Objetivo
Avaliar a prevalência dos terceiros molares não irrompidos e dentes supranumerários em indivíduos de Maringá e região.
Métodos
Foram avaliadas as radiografias panorâmicas de pacientes atendidos na clínica odontológica da Faculdade Ingá durante o ano de 2009. A posição dos terceiros molares foi classificada de acordo com Pell & Gregory1 e Winter2 e os dentes supranumerários de acordo com Garvey3. Foram calculadas as frequências absolutas e relativas das variáveis estudadas e aplicado o teste Qui-quadrado (p<0.05).
Resultados
De um total de 411 panorâmicas avaliadas, 113 indivíduos apresentavam terceiros molares não irrompidos e 5 pacientes tinham dentes supranumerários. Para os terceiros molares da maxila a maior prevalência foi da posição vertical A (p<0.05), e para a mandíbula foi posição mesioangular, classe 1A (p<0.05). Quanto aos dentes supranumerários, 3 eram caninos e 2 incisivos, sendo 2 na posição normal, 2 inclinados e 1 invertido.
Conclusão
De um total de 411 panorâmicas avaliadas, 113 indivíduos apresentavam terceiros molares não irrompidos e 5 pacientes tinham dentes supranumerários. Para os terceiros molares da maxila a maior prevalência foi da posição vertical A (p<0.05), e para a mandíbula foi posição mesioangular, classe 1A (p<0.05). Quanto aos dentes supranumerários, 3 eram caninos e 2 incisivos, sendo 2 na posição normal, 2 inclinados e 1 invertido.
Termos de indexação: Dente impactado. Cirurgia bucal. Dente supranumerário.
INTRODUCTION
Unerupted teeth are those which, when the time for eruption arrives, remain partially or totally inside the dental arch, i.e. they are intraosseous4-5. Impaction of third molars occurs due to insufficient space in the retromolar region, the amount of space being determined by the facial growth, size of teeth and their positioning in the dental arch6. The eruption of the third molars normally takes place after 18 years of age7-8.
The most common complications that occur as a result of impaction of the third molars are resorption of the second molar, periodontal problems4-9, internal resorption of the third molars and, more rarely, odontogenic cysts and tumors4. Accordingly, the recommendation to extract the third molars should be evaluated on an individual basis, taking into account the possibility of future complications10, and they may be carried out prophylactically8. Other more frequent indications are caries in the third molars and indications for orthodontic purpose4. Some situations contraindicate third molar extraction, such as asymptomatic teeth in elderly patients, very close to adjacent structures that may be damaged, when these serve as support for orthodontic prostheses or treatments5 and if the extraction could cause harm to the patient's physical or systemic condition4.
Supernumerary teeth, or hyperdontia, are characterized by an excess of teeth in the maxilla or mandible, and may be found in both the deciduous and permanent dentitions11-13. It may occur singly or in multiple form, unilaterally or bilaterally12. The most accepted theory for the appearance of supernumerary teeth is that alterations occur in the dental lamina14-15. These teeth are generally detected by means of radiographic examination15 and the main recommendations for extraction are: orthodontic treatment, fitting of implants, active alignment and associated pathologies4.
Supernumerary teeth may be classified according to morphology: conical; tuberculate or supplemental3. They are classified according to their position: normal, horizontal, inclined or inverted11. Despite the fact that these elements are usually asymptomatic, it is a factor that leads to a change in normal occlusion pattern12. There could also be associated clinical problems such as dentigerous cysts, root resorption, delayed eruption of other teeth14, as well as possibly leading to developmental problems such as cleft lip and palate13.
Therefore, bearing in mind the importance and the implications of these conditions, the present study soughtto analyze the prevalence of unerupted third molars and supernumerary teeth in patients in Maringá and region, attending the dental clinic at the Ingá School of Dentistry.
METHODS
This study was approved by the Ethics in Research Involving Human Beings Committee at the Ingá School of Dentistry (opinion no. 198/09), and was conducted in compliance with all the requirements and standards of National Health Council Resolution 196 of 13th June 1996.
In a retrospective study carried out between March and August 2010, 411 panoramic x-rays were evaluated of patients who attended the dental clinic at the Ingá School of Dentistry in 2009. Patient records were only evaluated if they included a panoramic x-ray and the patient was over the age of 18. The collection was carried out by a single examiner and the presence of maxillary and mandibular unerupted third molars and supernumerary teeth was evaluated.
The panoramic x-rays were selected in accordance with the region to be evaluated being clear and there being favorable lighting conditions, with the use of a black paper mask and a negatoscope, as well as an evaluation card with patient data. The Pell & Gregory1 and Winter2 classifications were used for third molars and the classification by Garvey et al.3 was used to classify the supernumerary teeth, as follows: a) Winter Classification2: compares the long axis of the third molar to the long axis of the second molar: vertical - when parallel; mesio-angular - when the long axis of the third molar is in the mid position in relation to the long axis of the second molar; disto-angular - when the long axis of the third molar is in a distal position in relation to the long axis of the second molar; horizontal - when the long axis of the third molar is perpendicular to the long axis of the second molar; b) Pell & Gregory Classification1: compares the mandibular third molar with the anterior edge of the mandibular ramus: class 1 - if the mesiodistal diameter of the crown is totally in front of the anterior edge of the mandibular ramus; class 2 - if the tooth is located to the rear such that close to half of it is covered by the ramus; class 3 - if the tooth is located completely inside the mandibular ramus. It compares the third molar to the occlusal plane of the second molar: class A - occlusal surface of the third molar at the same level as or above the second molar; class B - occlusal surface of the third molar between the occlusal level and the cervical level; class C - occlusal surface of the third molar below the cervical line of the second molar; c) Classification by Garvey et al.3 for supernumerary teeth, in terms of shape: conical; tuberculate; supplemental. In terms of position (erupted or not): normal - in a vertical position with the crown in coronal position in relation to the root; horizontal - in a perpendicular position in relation to the erupted teeth; inclined - at an angled position in relation to the erupted teeth; inverted - in a vertical position with the crown in apical position in relation to the root.
Both the absolute and the relative frequencies of the study variables were calculated and the chi-squared non-parametric test was applied, being statistically significant when p was less than 5%.
RESULTS
Of the 411 radiographs evaluated, 113 individuals and 217 teeth were seen to be unerupted, the majority of individuals affected having just one unerupted tooth.
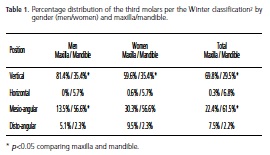
According to the Winter classification2, as demonstrated in Table 1, for both men and women (p>0.05), the vertical position for the third molars was more prevalent in the maxilla (p<0.05) and the mesioangular position in the mandible (p<0.05).
Table 2 shows a higher prevalence of position "A", i.e. when the occlusal surface of the third molar was at the same level as or above the second molar, either in the maxilla or the mandible (p>0.05), with an equal distribution between men and women (p>0.05).
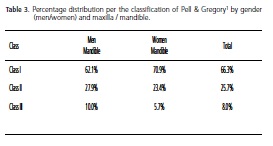
In both women and men (p>0.05), the highest prevalence found was for Pell & Gregory class I1, i.e. the mesiodistal diameter of the crown is completely forward of the anterior edge of the mandibular ramus (Table 3).
In the sample evaluated, 5 patients presented with supernumerary teeth, 3 of them men and 2 women, each individual having just 1 supernumerary tooth. It was possible to ascertain higher prevalence in the maxilla, with 4 supernumerary teeth, while only 1 supernumerary tooth was located in the mandible.
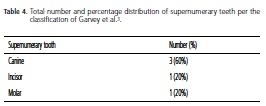
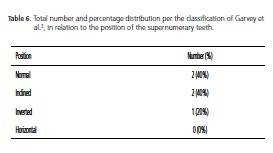
Also with regard to supernumerary teeth, 60% of those found were canine, 20% incisors and 20% molars (Table 4). As for the format, supplemental shape appeared in 80% of cases, followed by the tuberculated shape (Table 5). In respect of position, normal and inclined each appeared with 40%, as can be seen in Table 6.


DISCUSSION
The present study sought to evaluate the prevalence of unerupted third molars and supernumerary teeth in individuals attending, during 2009, the Dental Clinic of the Ingá School of Dentistry, which serves the city of Maringá and region. The sample comprised only individuals aged 18 or over, bearing in mind that from this age onwards there is greater certainty as to whether a third molar is erupted or not. According to the 411 radiographs evaluated, 113 individuals, equating to 27.5% of the total evaluated, presented with one or more impacted third molar and only 5 individuals, representing 1.2% of all patients evaluated, presented with at least one supernumerary tooth.
The low number of supernumerary teeth confirms the evidence found in the literature which also demonstrates a low frequency of supernumerary teeth16. In an epidemiological study in which 1,800 radiographs were evaluated, the authors observed the presence of 35 supernumerary teeth in 25 radiographs, corresponding to 1.4% of the total. Of the 35 supernumerary teeth, 14 were found in women and 11 in men, unlike this study, which demonstrates a higher prevalence of supernumerary teeth in men. The authors also found a higher prevalence in the premolar region, contradicting the findings of the present study, where the highest prevalence was in the premaxillary region16.
Several studies contradict the data found in this and other studies in relation to the prevalence of supernumerary teeth17-18. In a study conducted on Spanish children with supernumerary teeth, 79 patients were included and 113 supernumerary teeth were found, in both the maxilla and the mandible, with higher prevalence in males17. Another study 18 showed that, of the 240 patients evaluated, 60 (25%) presented with supernumerary teeth, a high outcome compared to the present study.
The literature shows there is a higher prevalence of supernumerary teeth in the maxilla than the mandible and in men versus women11,19 with between 90% and 98% occurring in the maxilla and more specifically, in the premaxilla19. In a study evaluating a sample of 153 individuals with supernumerary teeth, men were more affected than women and 90% of supernumerary teeth occurred in the premaxilla. As to shape, there was a prevalence of the conical form in 75% of cases and as regards position, 83.1% were normal10. Other authors have also shown a higher prevalence in the pre-maxillary region, involving incisors and canines13,20.
Several epidemiological studies have shown that the prevalence of unerupted third molars is high and is found more often than with the other teeth4-8, however canines, premolars and 1st and 2nd molars are also frequently found4. In a prospective study7, it was shown that with 2,857 third molars monitored over 8 years in individuals aged 18, 13.1% were still unerupted. However, in this study, the prevalence was found to be higher in individuals over 18 years of age.
In a study in which the authors evaluated 88 radiographs with a presence of unerupted third molars, a higher prevalence was seen of positions B and C for the maxilla and positions A and B for the mandible. The results of the present study show that the most common position of maxillary third molars was the vertical and mesio-angular for the mandible. The majority of mandibular third molars were completely forward of the anterior edge of the mandible (Class 1) and in both the maxilla and the mandible, the majority presented the occlusal surface on the same level as or above the second molar (Position A)1. This study showed that there was no significant difference between the sexes in relation to the Pell & Gregory classification1, in relation to both position and class.
The prevalence of almost 30% of individuals with unerupted teeth suggests a high need for the population in the study to seek a dental evaluation when these teeth fail to erupt, bearing in mind the complications that could be produced as a result. On the other hand, the prevalence of supernumerary teeth is low, as also demonstrated in other studies.
CONCLUSION
According to the findings of the present study, it may be concluded that around one-third of the population over 18 years of age has an unerupted third molar. The majority of unerupted third molars are to be found in the vertical position (maxilla) or mesio-angular position (mandible), Class IA. With regard to supernumerary teeth, it may be concluded that they are not common in this population and when they do appear, they occur mostly in the pre-maxillary region.
Collaborators
VB SANTOS contributed with the evaluation of the radiographs of the individuals included in the research study, and the composition of the article. AB SOUZA took part in the statistical analysis and composition of the manuscript. VM SAPATA participated in the composition of the manuscript. GO CORREA and FC MARSON contributed to the evaluation and the composition of the article. C OLIVEIRA E SILVA participated in the evaluation of the radiographs included in the study and in the composition of the manuscript. the manuscript. GO CORREA and FC MARSON contributed to the evaluation and the composition of the article. C OLIVEIRA E SILVA participated in the evaluation of the radiographs included in the study and in the composition of the manuscript.
REFERENCES
1. Pell GJ, Gregory GT. Impacted third molars: classification and modified technique for removal. Dent Digest. 1933;39:330-8. [ Links ]
2. Winter GB. Principles of exodontias as applied to the impacted third molars: a complete treatise on the operative technique with clinical diagnoses and radiographic interpretations. St. Louis: American Medical Books; 1926. [ Links ]
3. Garvey MT, Barry HJ, Blake M. Supernumerary teeth: an overview of classification, diagnosis and management. J Can Dent Assoc. 1999;65(11):612-6. [ Links ]
4. Farias JG, Santos FAP, Campos PSF, Sarmento VA, Barreto S, Rios V. Prevalências de dentes inclusos em pacientes atendidos na disciplina de cirurgia do curso de odontologia da universidade estadual de Feira de Santana. Pesq Bras Odontoped Clin Integr. 2003;3(2):15-9. [ Links ]
5. Hattab FN, Alhaija ESJA. Radiographic evaluation of mandibular third molar eruption space. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(3):285-91. doi: 10.1016/S1079-
2104(99)70029-6.
6. Grubor D, Breik O. The incidence of mandibular third molar impactions in different skeletal face types. Aust Dent J. 2008;53(4):320-4. doi: 10.1111/j.1834-7819.2008.00073.x. [ Links ]
7. Kruger E, Thomson WM, Konthasinghe P. Third molar outcomes from age 18 to 26: Findings from a populationbased New Zealand longitudinal study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(2):150-5. doi: 10.1067/moe.2001.115461. [ Links ]
8. Ay S, Agar U, Biçakçi AA, Köşger HH. Changes in mandibular third molar angle and position after unilateral mandibular first molar extraction. Am J Orthod Dentofacial Orthop. 2006;129(1):36-41. doi: 10.1016/j.ajodo.2004.10.010. [ Links ]
9. Yamaoka M, Furusawa K, Ikeda M, Hasegawa T. Root resorption of mandibular second molar teeth associated with the presence of the third molars. Aust Dent J. 1999;44(2):112-6. doi:
10.1111/j.1834-7819.1999.tb00211.x.
10. Capelli J Jr. Mandibular growth and third molar impaction in extraction cases. Angle Orthod. 1991;61(3):223-9. [ Links ]
11. Diaz A, Orozco J, Fonseca M. Multiple hyperodontia: Report of a case with 17 supernumerary teeth with non syndromic association. Med Oral Patol Oral Cir Bucal. 2009;14(5):E229-31. [ Links ]
12. Bezerra PKM, Bezerra PM, Cavalcanti AL. Dentes supranumerários: revisão da literatura e relato de caso. Rev Ci Med Biol. 2007;6(3):349-56. [ Links ]
13. Rajab LD, Hamdan MAM. Supernumerary teeth: review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12(4):244-54. doi: 10.1046/j.1365-263X.2002.00366.x. [ Links ]
14. Santos APP, Ammari MM, Moliterno LFM, Capelli JJ. First report of bilateral supernumerary teeth associated with both primary and permanent maxillary canines. J Oral Sci. 2009;51(1):145-50. doi: 10.2334/josnusd.51.145. [ Links ]
15. Klippel R, Weingartner E, Ciparandi MTO, Silva TSN, Hernandez PAG, Silva, ANJ. Dentes supranumerários dismórficos: relato de caso clínico. Rev Ci Med Biol. 2005;4(3):251-6. [ Links ]
16. Segundo AVL, Faria DLB, Silva UH, Vieira ITA. Estudo epidemiológico de dentes supranumerários diagnosticados pela radiografia panorâmica. Rev Cir Traumatol Buco-maxilo-fac. 2006;6(3):53-6. [ Links ]
17. Ferrés-Padró E, Prats-Armengol J, Ferrés-Amat E. A descriptive study of 113 unerupted supernumerary teeth in 79 pediatric patients in Barcelona. Med Oral Patol Oral Cir Bucal. 2009;14(3):E146-52. [ Links ]
18. Brook AH, Griffin RC, Smith RN, Townsend G, Kaur G, Davis GR, et al. Tooth size patterns in patients with hypodontia and supernumerary teeth. Arch Oral Biol. 2009;54(Suppl 1):S63-70. doi: 10.1016/j.archoralbio.2008.05.016. [ Links ]
19. Torres MA, Fernandes KP. Dente supranumerário e diastema mediano superior. RGO - Rev Gaúcha Odontol. 1996;44(4):220-9. [ Links ]
20. Anthonappa RP, Lee CK, Yiu CKY, King NM. Hypohyperdontia: literature review and report of seven cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(5):e24-30. doi:
10.1016/j.tripleo.2008.07.012.
 Correspondence to:
Correspondence to:
VB SANTOS
Av. Colombo, 9727, Km 130, 87070-810, Maringá, PR, Brasil
e-mail: vanessabobig@yahoo.com.br
Received on: 30/8/2011
Final version resubmitted on: 13/1/2012
Approved on: 19/3/2012
