










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.2 Porto Alegre Abr./Jun. 2013
ORIGINAL / ORIGINAL
Relationship between oral health and psychological factors in institutionalized and non-institutionalized elderly individuals
Relação entre saúde bucal e fatores psicológicos em idosos institucionalizados e não institucionalizados
Eduardo KURIHARAI; Vander José das NEVESII; Vivian Sayuri KITAYAMAIII; Marcos Sergio ENDOII; Raquel Sano Suga TERADAI; Fernanda Klein MARCONDESII
I Universidade Estadual de Maringá, Departamento de Odontologia. Av. Mandacaru, 1550, Campus Universitário, 87080-000, Maringá, PR, Brasil.
II Universidade Estadual de Campinas, Faculdade de Odontologia. Piracicaba, SP, Brasil.
III Consultório Particular. Maringá, PR, Brasil.
ABSTRACT
Objective
To compare the oral health status between institutionalized and non-institutionalized elderly individuals living in Maringá, PR, Brazil and to analyze how clinical and psychologic variables are correlated.
Methods
In this study, 86 elderly persons from Maringá were analyzed, of whom 38 were institutionalized and 48 non-institutionalized. Subjective oral health conditions based on General Health Assessment Index (GOHAI) were analyzed. Geriatric Depression Scale (GDS-15) and Perceived Stress Scale (PSS) were used to evaluate psychological conditions and stress self-perception, respectively, of all individuals. The dental status of subjects was evaluated using the decayed, missing, and filled teeth index (DMFT), considering their use of or need for removable dental prostheses. The salivary flow and salivary cortisol levels were measured.
Results
Institutionalized subjects had more symptoms of depression, lower salivary flow and a larger number of missing and decayed teeth when compared with non-institutionalized individuals, who presented a larger number of filled teeth. Use of and need for prosthesis were more prevalent in the institutionalized group. Correlation was found between salivary flow and need for prosthesis, and between salivary flow and missing teeth. No significant statistical difference was found among GOHAI, PSS and salivary cortisol levels.
Conclusion
The fact that institutionalized elderly assessed have a more precarious oral health status than that of the non-institutionalized is associated with clinical, social, and psychological aspects. Effective dental and psychological interventions are needed to improve the quality of oral health of the institutionalized elderly living in Maringá.
Indexing terms: Aged. Geriatric dentistry. Oral health.
RESUMO
Objetivo
Comparar as condições de saúde bucal entre idosos institucionalizados e não institucionalizados da cidade de Maringá e analisar como as variáveis clínicas e/ou psicológicas se correlacionam.
Métodos
Participaram desta pesquisa 86 idosos da cidade de Maringá, 38 institucionalizados e 48 não institucionalizados. Foram avaliadas as condições subjetivas de saúde bucal por meio do índice General Oral Health Assessment Index (GOHAI). A condição psicológica foi avaliada pela Escala de Depressão Geriátrica (GDS-15) e a autopercepção de situações estressantes, pela Escala de Estresse Percebido (PSS). Para avaliação clínica da saúde bucal foi analisada a condição dos dentes por meio do índice de dentes cariados, perdidos, obturados (CPO-D) e o uso e necessidade de próteses removíveis. Foram também analisados o fluxo salivar e a concentração de cortisol salivar.
Resultados
O grupo institucionalizado apresentou mais sintomas depressivos, menor fluxo salivar, maior número de dentes perdidos e cariados, e maior frequência de uso e necessidade de próteses dentárias em comparação com o não institucionalizado. Idosos não institucionalizados apresentaram maior quantidade de dentes restaurados. Foi observada correlação negativa entre fluxo salivar e necessidade de próteses e também entre fluxo salivar e dentes cariados. O índice GOHAI, PSS e níveis de cortisol salivar não diferiram entre os grupos.
Conclusão
A precária condição de saúde oral do idoso institucionalizado em relação ao não institucionalizado está associada com aspectos clínicos, sociais e psicológicos. Nesse sentido, efetivas intervenções odontológicas e psicológicas são necessárias para melhorar a qualidade da saúde oral dos idosos institucionalizados na cidade de Maringá.
Termos de indexação: Idoso. Odontologia geriátrica. Saúde bucal.
INTRODUCTION
According to the World Health Organization (WHO), the elderly are chronologically classified as individuals over the age of 65 years in developed countries, and over the age of 60 years in developing countries.
According to the latest Summary of Social Indicators released by the Brazilian Institute of Geography and Statistics (IBGE)1, Brazil has over 21 million elderly persons today, exceeding the numbers in European countries such as France, England and Germany. From 1998 to 2008, the proportion of elderly persons increased from 8.8% to 11.1%. There are forecasts that by the year 2025, Brazil will have the sixth largest elderly population in the world, in absolute numbers, with over 30 million persons over the age of 60 years2. This population aging is due to the intense and rapid fall in the birth rate and increase in life expectancy of Brazilians. From 1998 to 2008 there was an increase in the proportion of childless couples, rising from 13.3% to 16.7%, accompanying the drop in birth rate, which tell from 2.43 children per woman in 1998 to 1.89 in 2008. In 1998, life expectancy at birth was 69.66 years, and in 2008 this increased to 72.86 years1. In this context, the IBGE warned, by means of the Summary of Social Indicators, 2009, that urgent steps need to be taken in order to guarantee an infrastructure of care for the elderly of Brazil in all sectors.
In the society in which we live, the elderly have been discriminated and excluded because of being considered non productive and not being integrated with the culturally valued patterns of beauty and youth. However, it is precisely at this stage of life that care of elderly persons is determinant of their quality of life. With the appearance of diseases and increase in physical frailty, emotional disturbances may accentuate the feelings of dependence, insecurity, worries, anxieties, fears and changes in self-image3.
Within the family circle, feelings of loneliness and even depression may appear, due to the loss of occupation, independence of children, widowhood or the emptying of the home (empty-nest syndrome). On must also consider the loss of authority of elderly persons who, due to illness, poverty or emotional frailty tend to lose their space to their children and grandchildren in decision on central aspects of their lives4. Added to this, the profound transformations observed in Brazilian society of the last few decades, such as the increasing participation of women in the work market, reduction in the size of the family, and population aging have also caused important limitations on providing the basic care required by the elderly on the part of family members, and formulators of public policies5. As a result of the foregoing, and due to the unpreparedness of the family to assume the role of elderly care provider, millions of Brazilians have already left the lifestyle of living with the family, to live in institutions for the elderly on a long term basis, places traditionally known as old-age homes.
Of the total number of elderly persons in Brazil, around 100 thousand are believed to be living in old age homes at present, of whom approximately 1/3 do not have either the physical conditions or income generation that would allow them to live in an autonomous and independent manner5. As a consequence of Brazilian population aging, the contingent of institutionalized elderly persons has also grown, and due to the fact that they need special care, the homes that were previously destined for invalid elderly, now have a new mission: To care for elderly persons needing multiprofessional assistance, due to the loss of functions that make it problematic for them to live alone or with the family6.
With advancing age, there is a drop in the level of oral hygiene and increasing incidence of oral diseases in the elderly7. This at least partly results from the fact that up to the mid 1990s, caregivers and dentists had little perspective with regard to the longevity of elderly persons and were not concerned about maintenance of the teeth in the oral cavity7. However, professionals who work with the aging process, in the most diverse areas of knowledge, must provide the elderly with bio-psycho-social well being, especially those who are institutionalized, in order to potentiate their overall functions, so that they obtain greater independence and autonomy6. In this case, the dentist must have a profound interest in the promotion, preventing and recovery of these patients' oral health, a practice that must be inserted into the routine of old age home institutions as part of the multiprofessional work. This is because the oral condition directly influences individuals' quality of life, by the repercussion on the capacity of mastication, nutrition, phonetics and socialization7.
In view of the foregoing, and considering the lack of information with respect to the real oral health status of institutionalized elderly persons, the aim of this study was to compare the oral health status between institutionalized and non institutionalized elderly persons, and analyze how the clinical and/or psychological variables are correlated. It is the authors' hope that the results of this research will provide additional support for dentists so that they may use them in educational, preventive and curative programs related to the oral and general health of institutionalized and non institutionalized elderly persons.
METHODS
In this study 86 persons participated, of whom 38 were institutionalized and 48 non institutionalized. The criteria used for including patients in the study were: To be of a minimum age of 60 years; present the minimal cognitive function necessary, evaluated by the Mini Mental State Exam (MMSE); must not present Cushing and Sjögren syndromes; must not make use of corticoids or diuretics. The convenience sampling method was used for comparative effects of the two groups, considering the ease of access to the participants. The volunteers in the institutionalized group were recruited from the four main old age home institutions in Maringá (PR), Brazil, a city with 335,511 inhabitants, according to the latest IBGE estimate1. The volunteers of the non institutionalized group were recruited from the Social Service of Commerce (SESC), in the same city. Those responsible for the old age home institutions and for SESC signed the term of authorization for the development of the study.
The study was approved by the Research Ethics Committee of the Piracicaba Dental School, State University of Campinas (Protocol No. 188/2006) and the State University of Maringá - UEM (Protocol No: 105/2007). All the volunteers signed the Term of Free and Informed Consent, in accordance with the determinations of Resolution 196, of October 10, 1996, Of the National Council of Health, Ministry of Health of Brazil. Data were collected during a period of three months. Application of the questionnaires and saliva collections were carried out by 17 academic students of the dental course at UEM, all previously trained to perform these activities. Survey of the oral problems was conducted by a geriatric dentistry professor of UEM.
Three questionnaires were used for selecting the volunteers. The first of these, the "cognitive capacity MMSE", tested and validated in Brazil, was used to verify the volunteers' capacity of comprehension in order to respond to the other questionnaires. In the MMSE, the cut-off points obtained by Almeida8 were considered: ≤ 19 points for the diagnosis of dementia among the elderly without schooling, and ≤ 23 points for literate elderly persons and those with a previous schooling history of at least 1 year. In this study, only volunteers who presented scores higher than these values of the MMSE participated in the research. By means of a second questionnaire about the "state of health and use of medications", the occurrence of systemic diseases, use of corticoids, diuretics, anti-hypertensive and anti-depressive medications and smoking and drinking habits were evaluated. Individuals who made use of antihypertensive and anti-depressive medications were not excluded, because this concerned the majority of the sample, and would lead to the loss of representativeness and reality of Brazilian elderly persons, since there is high prevalence of the use of medications in the elderly9. By means of a third "socioeconomic" questionnaire, relevant information was obtained as regards age, gender, marital status, educational and income levels.
After the volunteers were selected, the psychological condition of both groups, institutionalized and non institutionalized was evaluated, by means of the short version of the geriatric depression scale, consisting of 15 items (GDS-15), translated and validated in Brazil by Almeida & Almeida10. In order to avoid allowing responses about somatic complaints, the GDS-15 questionnaire presents the possibility of replying with "yes" or "no". With scores that vary from zero to 15 points, it allows one to establish cases with and without depression, as well as stating the degree of depressive symptoms of the individuals evaluated. Almeida & Almeida11 demonstrated that the cut-off point 5/6 (non case/case) produces a high rate of sensitivity and specificity for the diagnosis of depression. According to Linhares et al.12, scores from zero to 5 indicate the absence of depression, from 6 to 10 indicate light to moderate depression and scores from 11 to 15 indicate severe episodes of depression.
The degree of perception of stressful situation of the elderly was determined by the Perceived Stress Scale (PSS), translated and validated in Brazil by Luft et al.13. The scale presents 14 items, designed to verify to what extent the respondents evaluated their lives as being unpredictable, uncontrollable and overburdened12. Each one of the 14 questions allow a score from zero to 4 according to the responses (zero when the response was "never", 1 for "almost never", 2 for "sometimes", 3 for "almost always" and 4 for "always"). The scores of the scale may vary from zero to 56 points, according to the scores of all the questions.
Unstimulated saliva collection from each volunteer was performed for 5 minutes in the three periods of the day: morning (between 7-8hs), afternoon (14-15hs) and at night (18-19hs), once a week, for four weeks. In the first thirty seconds, the volunteers swallowed the saliva, and after that deposited the saliva produced in a 50 ml plastic receptacle (Salivette®, Sarstedt, Rommelsdorf, Germany), previously weighed on an analytical scale. By subtracting the weight of the Salivette® from the total weight obtained after the collection, the weight of saliva in grams was obtained. Determination of the saliva volume was done directly by the weight obtained in grams, considering the saliva density of approximately 1 g/ml14. Lastly, the salivary flow was determined by dividing the volume of saliva in each Salivette® by the collection time of 5 minutes. Afterwards the saliva was centrifuged (2.500 rpm for 5 minutes) and the samples were kept at -20°C for salivary cortisol analysis, the concentrations of which were determined by a commercially available immuno-enzymatic assay kit (Salimetrics®, State College, Pennsylvania, USA), with a sensitivity of 0.003 μg/dL and intra- and inter-assay coefficients of 3.50% and 5.08%, respectively. The saliva collection of the first week was discarded, so that all the analyses involving saliva were made only in the last three weeks. This was necessary, because in a pilot study we observed a higher level of cortisol and low salivary flow in the first collection which is made in the elderly, probably because it was the volunteer's first experience of this type of procedure.
For subjective evaluation of the elderly persons' oral conditions, the translated and validated Brazilian version of the General Oral Health Assessment Index (GOHAI) was used, which presented a Cronbach α coefficient of 0.65, according to Silva & Fernandes15. Composed of 12 questions, this index covers three domains: Physical/ functional (comprising diet, speech and swallowing); psychosocial/psychological (comprising concern about or care of oral health, dissatisfaction with appearance, selfconsciousness relative to dental health, and privation of social life due to oral problems; pain/discomfort (comprising use of medications due to oral problems)16. There are three possible answers to each question in this index and each question is awarded scores varying from 1 to 3 (1 = when the response is "always"; 2 = when the response is "sometimes" and 3 = when the response is "never"), resulting in a final score that may vary from 12 to 36. In this index, the higher the score acquired by the individual, the better is his/her self-evaluation of his/her oral health.
For evaluating the oral health condition, the decayed, missing, filled teeth index (DMF-T index) was used, which allowed one to evaluate and compare the history of dental caries between the groups of elderly persons in this study. This index presents the possibility of a score between zero and 32 points, with the minimum score (zero) corresponding to individuals who have their 32 teeth without any caries experience, and the maximum score (32) corresponding to individuals who have lost all their teeth or who had some teeth, which in the vest condition, were restored; and in the worst condition, indicated for extraction. The use of and need for removable dental prosthesis (complete maxillary and/or mandibular, and partial maxillary and/or mandibular) was also analyzed by clinical evaluation. Considering that in one and the same individual cannot have more than two removable dentures in the mouth, this study determined values that ranged from zero to 2 for each individual, both in the evaluation of use and of the need for dentures, in the following manner: zero for those who did not wear dentures, or who did not need them; 1 for those who wore dentures, or who did need one; 2 for those who wore them, or who needed two dentures. The mean of the values (between zero and 2) obtained in each of the institutionalized and non institutionalized groups was used for statistical comparison.
The data were submitted to statistical analysis using the software program SAS (The SAS system, release 9.1.3., SP-4. SAS Institute Inc. Cary: NC, 2002), by means of which uni and bi-dimensional contingency tables were constructed, and analysis of variance performed with mixed models and correlations studies. In the unidimensional tables the Chi-square test was applied to test the hypothesis of absence of difference in the proportions. In the bi-dimensional tables the Chi-square and Chi-square and likelihood ratio statistical tests were applied to test the absence of linear association between lines and columns; the Mantel and Haenszel Chi-square test was applied to test the hypothesis of absence of linear association between the lines and columns of the tables, and the Cochran-Mantel- Haenszel test was used to test the hypothesis of absence of difference between the means of scores of the lines of the table, thus comparing the groups of institutionalized and non institutionalized persons, to whom the Wilcoxon test was also applied.
For analysis of the cortisol and salivary flow measures, the analysis of variance technique was used with mixed models based on the random nature of the volunteers and fixed members of the groups. In this analysis, the structure of diagonal covariance and the Restricted Maximun Likelihood (REML) method of estimation were adopted.
In the correlation studies, in order to test the existence of, and quantify the association between variables, partial correlations were calculated to eliminate the effects of group. The Pearson correlation coefficient was used according to the nature of the variables under study.
In all the statistical tests, values of p<0.05 were considered statistically significant.
RESULTS
By application of the Mini Mental test, it was possible to select volunteers capable of understanding in order to respond to the other questionnaires used in this study, as only those who presented scores of over 19 or 23 were selected. The questionnaire on the health status and use of medications allowed the selection of volunteers, who did not present the Sjögren and/or Cushing syndrome, and who did not make use of diuretic or corticoid medications, to compose the sample of this study. Thus, 38 institutionalized and 48 non institutionalized elderly persons took part in this study.
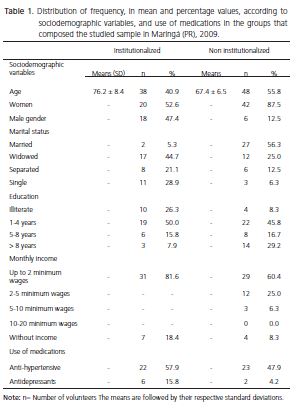
The number of illiterate volunteers and those with a history of schooling in both groups is presented in Table 1, the purpose of which is only to characterize the studied sample.
The institutionalized group presented a higher mean age, higher frequency of widowed and single persons, higher percentage of illiterate persons and those without monthly income, in comparison with the non institutionalized group (Table 1). Whereas, in the non institutionalized group there was a higher mean number of married persons. In both studied groups, there was higher frequency of women and persons with a monthly income of up to 2 minimum wages.
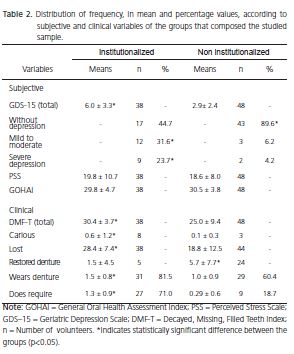
The data obtained from the Geriatric Depression Scale (GDS-15) are presented in Table 2. In the institutionalized group, the frequency of mild to moderate depression (6-9 points) as well as severe depression (10- 15 points) was higher in comparison with that in the non institutionalized group (p<0.0001; Table 2).
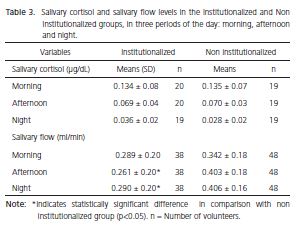
There was no statistically significant difference between the institutionalized and non institutionalized groups in the survey of stress evaluated by the Perceived Stress Scale (PSS) (p>0.05; Table 2) and there was also no statistically significant difference in the salivary cortisol levels between the groups in the three periods of the day (p>0.05; Table 3).
The GOHAI index, which evaluates self-perception of oral health, showed that there was no statistically significant difference between the groups (p>0.05; Table 2). On the other hand, the DMF-T index showed higher values in the institutionalized in comparison with the non institutionalized group (p<0.0001; Table 2). The clinical data found by the DMF-T index showed that the institutionalized in comparison with the non institutionalized group, presented a high number of missing (p<0.0001) and carious (p=0.0327) teeth (Table 2); however, the non institutionalized group presented the higher number of restored teeth in comparison with the institutionalized group (p=0.0006; Table 2).
The clinical data with respect to dental prostheses are also presented in Table 2 and the results showed that in comparison with the non institutionalized group, the institutionalized group was the one in which most dentures were worn (p=0.0116) and were most needed (p<0.0001).
Whereas, salivary flow in the afternoon (p<0.0001) and night (p<0.0001) periods showed lower values in the institutionalized in comparison with the non institutionalized group (Table 3), without difference in salivary cortisol (p>0.05).
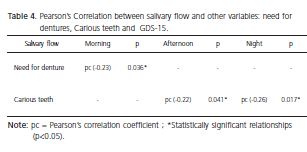
Table 4 presents the Pearson correlations (pc) observed in this study. There was negative correlation of salivary flow in the morning period with the need for dentures (p=0.036; pc= -0.23); negative correlation of salivary flow in the afternoon period with carious teeth (p=0.041; pc= -0.22) and there was negative correlation of salivary flow in the night period, also with carious teeth (p=0.017; pc= -0.26).
DISCUSSION
Over the course of history, not only in the municipality of Maringá, but also throughout the country, the prevention and treatment of dental problems has been directed towards children and pregnant women, and the elderly population has been marginalized in collective oral health programs, particularly those who are institutionalized, and who frequently present precarious conditions of life in comparison with the elderly population in general2. Nevertheless, this is a condition that needs to be changed, and special attention must be given to the elderly population, due to the recent increase in life expectancy in Brazil, and consequently, to the increasing demands and needs of the contingent of elderly Brazilians, in the area of health. These factors, in addition to the significant changes that have occurred in the pattern and incidence of oral diseases, demand the implementation of new public policies to provide the oral health services with guidelines with respect to the elderly population17. Thus, identification of the causes of oral problems in institutionalized elderly persons is of great value, from the aspect of guiding these public policies and extending the process of retrieving this population group from the apparent context of abandonment in which they find themselves.
The data presented in this study show important alterations in the oral and mental health of the institutionalized in comparison with non institutionalized elderly persons in Maringá (PR), Brazil, and suggest the need for greater attention from the dental prevention and treatment services and psychotherapy services, in the long term residence institutions in the municipality.
At present, the elderly in Brazil suffer strong emotional impacts due to the lack of social structure and health programs that allow them to continue as productive members of society. This lack of preparation of Brazilian society to deal with the problems of elderly persons and adequately integrate them into social life, condemns individuals to shelter provided by the family or old age home institutions; a condition that frequently generates chronic stress or feelings of isolation, dissatisfaction, diminished self-esteem and anguish in the elderly; emotional alterations, which in turn, have to be considered associated with the alterations in their oral health18. It was due to the fact that health and disease are largely influenced by the social space in which man lives, and also because there are few scientific studies showing the relationship between emotional and oral health factors that this study was designed. From the data obtained, no significant difference between the institutionalized and non institutionalized groups was observed according to the Perceived Stress Scale and salivary cortisol levels; and there was no relationship between stress and oral alterations, indicating that social life, whether it is within the old age home institutions of Maringa, or outside of them, apparently is not a stress generating factor to a sufficient extent to influence the salivary cortisol levels in the elderly of both groups, whereas, the dental condition and salivary flow did show significant differences between the groups. Nevertheless, it must be made clear that many variables could not be controlled in this study, such as the sociodemographic type, which in some way may have influenced analysis of the salivary cortisol levels and/or self-perception of stress, evaluated by the Perceived Stress Scale.
On the other hand, the Geriatric Depression Scale in the present study pointed out greater occurrence of depressive symptoms in the institutionalized volunteers in comparison with non institutionalized persons. This is particularly important, considering that the incidence of depression among the institutionalized elderly has been estimated to be four times higher than it is among non institutionalized elderly persons19. In a recent research conducted in Brazil, Plati et al.20 also observed high frequency of depressive symptoms among institutionalized when compared with non institutionalized elderly persons. Kressin et al.21 have demonstrated that depressive symptoms are important risk factors that compromise the quality of oral health, particularly in the elderly, suggesting the importance of the dentist's participation in preserving oral health by prevention, identification and indication of depressed elderly persons for psychotherapeutic treatment, in parallel to dental treatment. In this sense it is possible to infer that the worse dental condition and low salivary flow in the institutionalized elderly of this study, may be coadjuvant to the depressive symptoms in this group.
Depressive symptoms may also influence the salivary flow levels by the increase in anticholinergic activity of the depressive process, capable of causing a decreasing saliva production22. In the case of an elderly person being patient with diagnosed depression, and under treatment with antidepressant medication, the condition of hyposalivation may be even more accentuated, because the majority of antidepressants amplify xerostomia by blocking parasympathetic stimulation of the salivary glands23.
Hugo et al.24 observed that diminished salivary flow may also be responsible for diminishing the elastic properties of oral soft tissues, making the oral mucosa for fragile and susceptible to ulcerations and traumatisms by dentures2, in addition to increasing susceptibility to caries, promoting demineralization of the teeth and predisposing the elderly to fungal infections. In the present study, the results revealed a negative correlation, shown by the Pearson coefficient, between carious teeth and salivary flow, indicating that the lower the salivary flow, the greater the presence of carious teeth. This correlation is of great value where the institutionalized elderly are concerned, since this is the group that most presented depressive symptoms, and consequently the one with most propensity to neglecting oral hygiene.
In addition to the lack of interest in oral hygiene due to the depressive process, this group may have a preference for the ingestion of carbohydrates, due to a reduction in serotonin in the central nervous system, which also promotes a preference for sweet foods23, predisposing the elderly to the development of dental caries. In addition to the lower salivary flow and presence of a higher number of dental caries, it was also observed that the institutionalized group presented the higher number of missing teeth, reflecting an apparent history of neglecting oral health. This condition may promote difficulty with chewing and stimulate elderly persons' preference for chewing soft foods, rich in carbohydrates, which may possibly contribute to reducing stimulation of the salivary glands25 and to more rapidly deteriorating the oral health of institutionalized elderly persons. As a result of the large number of carious teeth, and probably due to the sociodemographic conditions themselves of the institutionalized elderly, they were also the ones who presented the lowest mean number of restored teeth in comparison with the non institutionalized elderly.
The DMF-T index was significantly higher in the institutionalized in comparison with the non institutionalized group. This result may be partly explained by the fact that the institutionalized group was, on an average, 10 years older than the non institutionalized group. As regards this condition, our findings are in agreement with those of the latest National Epidemiological Survery26, which found a mean value of the DMF-T of 27.79 for the age-range from 65 to 74 years of age in Brazil. Furthermore, Caldas Junior et al.27 found a significantly higher DMF-T index in institutionalized than in non institutionalized elderly persons.
In the present study it was observed that more institutionalized elderly persons wore dentures, and also that they presented greater need of them, in comparison with the non institutionalized elderly. This condition may be justified by the lack of dental care in the studied elderly residents of old age homes, together with the lack of information on the part of caregivers who did not identify problems in the prosthetic parts. There was a negative correlation between salivary flow and need for dental prostheses, indicting that the greater the need for these, the lower the salivary flow of the elderly person. The study of Matsuda et al.25, showed that prosthetic treatment significantly increased the maximum force of dental occlusion and salivary flow, suggesting that the absence of prosthetic treatment leads to low force of occlusion and low salivary flow in the elderly. When studying elderly Israelis, Wolff et al.28 also related that the salivary flow increased significantly two days after insertion of complete dentures, and diminished after 3 week, however, remained significantly above the initial values observed before the use of dentures. Thus, the association between the need for dental prostheses, and low salivary flow observed in the present study may be explained by alterations in the force of dental occlusion in elderly persons who have lost their teeth. Although the force of occlusion was not evaluated in this study, one could suppose that a diminished maximum force of occlusion among institutionalized elderly persons could be one of the associated factors that could reduce salivation in this group, as a result of the need for new dentures. Moreover, it has been suggested that chronic stimulation of mechanoreceptors located under the denture, could increase salivary flow29 and that the difficulty in chewing harder foods due to a reduction in maximum force of occlusion, because of lack of dentures, may diminish stimulation of the salivary glands in elderly persons, irrespective of other variables, such as age-related diseases or use of medications25,30. Masticatory stimulus on salivary glands exerted by dentures may improve not only stimulated salivary flow, but that of unstimulated flow as well, which contributes greatly to total salivary flow during the daytime salivation cycle25. Lastly, the absence of dental prostheses, associated with the depressive and aging processes may generate negative effects on salivary gland stimulation and contribute to the more rapid deterioration of oral and general health of institutionalized elderly persons.
The GOHAI index was used in this study, because it provides self-evaluation of the individual's oral health. The manner in which individuals perceive their oral health is an indispensable factor determining whether they seek dental care or neglect it. In the present study, the GOHAI index in the institutionalized group did not differ from that of the non institutionalized group. This result apparently represents a contrast between the clinical conditions observed by the dentist and the self-perception of oral heal in the group of institutionalized elderly persons, as it was expected that the institutionalized elderly would present precarious perception of their oral health in the face of the clinical condition demonstrated by the DMF-T index, and by evaluation of the use of and need for dentures. In the present study, the apparent contradiction between the clinical conditions evidenced, and the data obtained in GOHAI, may be related to the fact that although the GOHAI index is an important indicator of health because it expresses the individual's cultural values as regards his/ her health, it also reveals that the patient analysis his/her oral health using different criteria from those adopted by the dentist14.
Finally, it is important to recognize the limitations of this study. The population analyzed was chosen by convenience, and consequently, the results of this study may be specific for the city of Maringá. The generalization of the results obtained in this study require additional analysis in similar populations in other Brazilian cities. Moreover, the correlations of the variables obtained by the Pearson coefficients, and observed in certain periods of the day, without having occurred in other periods, are complex interpretations and require additional studies in order to be effectively explained.
CONCLUSION
In this study, the institutionalized group was characterized by the higher level of occurrence of depression and low salivary flow, which is associated with the worse conditions of the DMF-T index and greater need for the use of dentures. These conditions lead to low masticatory effectiveness, and appear to contribute to the more unfavorable oral health condition observed in institutionalized in comparison to non institutionalized elderly persons. Sociodemographic factors such as marital status, income and age, in addition to individual history may have contributed to this condition.
The results of this study allow evidence to be shown of the lack of information with regard to oral health in old age home institutions in Maringá, and the little participation by the dentist in the multidisciplinary teams that work in these institutions. Furthermore, these results allow us to conclude that there is an important degree of negligence by public power with regard to dental treatment in this special population, which after years of work, finds itself without support at a time of life when they most need care.
Although this study was conducted in the city of Maringá, in a sample restricted to volunteers, the data here obtained, probably reflects the reality of various other cities. In this context, considering the rapid Brazilian population aging, the data obtained that there is urgent need for effective action by the professional dentist, in conjunction with psychologists and psychiatrists, within the old age home institutions. If this does not occur, the incidence of the precarious oral conditions and depressive symptoms observed in this study may become even more serious in the short term, due to the vicious cycles that occur (dental problem problems promoting emotional and psychological problems and vice-versa). With the purpose of minimizing this problem, partnerships between universities and old age home institutions may be established, including the participation of dental students in the practice of dentistry within these institutions The would extend the education of geriatric dentists and could improve the quality of oral health of institutionalized elderly persons.
Acknowledgements
The authors thank the volunteers and directors of the old age home institutions and SESC for their participation in this study; and thank Patricia Oliveira de Lima e Gabriela Lopretti Guarda for help with the salivary cortisol dosing; and thank Marcelo Corrêa Alves for carrying out the statistical analysis; and thank Margery Galbraith for editing the English in the manuscript.
Collaborators
E KURIHARA contributed to all the work processes, contact with the institutions, calibration of the students during data collections, supervision of collections at SESC, laboratory work of weighing, centrifugation, transfer and storage of saliva. He participated actively in the processing and analysis of the cortisol samples, in addition to interpretation of the statistical data and writing the article. VJ NEVES was responsible for storage, laboratory analyses and processing of the salivary cortisol samples; contributed to interpretation of the statistical data and, writing the article. VS KITAYAMA was responsible for initial contact with the institutions, coordination and supervision of collections at the Old Age Home São Vicente de Paulo. She developed the laboratory work of weighing, centrifugation, transfer and storage of saliva and tabulated the data from the questionnaires and cooperated with writing the article. MS ENDO was responsible for forwarding the project to the Ethics Committee, supervision of the collections at the Old Age Homes Wajunkay and Luzamor. He developed the laboratory work of weighing, centrifugation, transfer and storage of saliva and cooperated with writing the article. RSS TERADA supervised the collections at the Old Age Home Lar dos Velhinhos, cooperated with interpretation of the statistical data and writing the article. FK provided guidance and defined the questionnaires to be applied, in addition to determining the methodology for salivary cortisol quantification. She cooperated with writing the article.
REFERENCES
1. Instituto Brasileiro de Geografia e Estatística. Ministério do Planejamento, Orçamento e Gestão. Censo Demográfico 2009 [Texto em sítio da internet]. [citado 2009 Jan 26 ]. Disponível em: <http://www.ibge.gov.br/cidadesat/topwindow.htm?1> [ Links ].
2. Silva SO, Trentin MS, Linden MSS, Carli JP, Neto NS, Luft LR. Saúde bucal do idoso institucionalizado em dois asilos de Passo Fundo - RS. RGO - Rev Gaúcha Odontol. 2008;56(3):303-8.
3. Cattani RB, Girardon-Perlini NMO. Cuidar do idoso doente no domicílio na voz de cuidadores familiares. Rev Eletr Enf. 2004;6(2):254-71.
4. Pereira A, Freitas C, Mendonça C, Marçal F, Souza J, Noronha JP, et al. Envelhecimento, estresse e sociedade: uma visão psiconeuroendocrinológica. Ciências & Cognição. 2004;1:34- 53.
5. Pasinato MTM, Kornis GEM. Cuidados de longa duração para idosos: um novo risco para os sistemas de seguridade social [texto na Internet]. In: Instituto Brasileiro de Pesquisa Econômica Aplicada [homepage na Internet]. Rio de Janeiro: Instituto Brasileiro de Pesquisa Econômica Aplicada; 2009 [citado 2009 Jan 26]. Disponível em: <http://www.ipea.gov.br/003/00301009.jsp?ttCD_CHAVE=8581>.
6. Pereira LSM, Britto RR, Pertence AEM, Cavalcante EC, Guerra VA. Programa Melhoria da Qualidade de Vida dos Idosos Institucionalizados. In: 8° Encontro de Extensão da Universidade Federal de Minas Gerais; 2005; Belo Horizonte. Anais. Belo Horizonte: Universidade Federal de Minas Gerais; 2005.
7. Mello ALSF, Padilha DMP. Instituições geriátricas e negligência odontológica. Rev Fac Odontol Porto Alegre. 2000;41(1):44-8.
8. Almeida OP. Mini exame do estado mental e o diagnóstico de demência no Brasil. Arq Neuropsiquiatr. 1998;56(3-B):605-12. doi: 10.1590/S0004-282X1998000400014.
9. Flores LM, Mengue SS. Uso de medicamentos por idosos em região do sul do Brasil. Rev Saúde Pública. 2005;39(6):924-9. doi: 10.1590/S0034-89102005000600009.
10. Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry. 1999;14(10):858-65. doi: 10.1002/ (SICI)1099-1166(199910)14:10<858::AID-GPS35>3.0.CO;2-8.
11. Almeida OP, Almeida SA. Confiabilidade da versão brasileira da Escala de Depressão em Geriatria (GDS) versão reduzida. Arq Neuropsiquiatr. 1999;57(2-B):421-6. doi: 10.1590/S0004- 282X1999000300013.
12. Linhares CRC, Coelho VLD, Guimarães RM, Campos APM, Carvalho NT. Perfil da clientela de um ambulatório de geriatria do Distrito Federal. Psicol Reflex Crít. 2003;16(2):319-26.
13. Luft CD, Sanches SO, Mazo GZ, Andrade A. Versão brasileira da Escala de Estresse Percebido: tradução e validação para idosos. Rev Saúde Pública. 2007;41(4):606-15. doi: 10.1590/S0034- 89102007000400015.
14. Flink H, Tegelberg A, Lagerlo F. Influence of the time of measurement of unstimulated human whole saliva on the diagnosis of hyposalivation. Arch Oral Biol. 2005;50(6):553-9. doi: 10.1016/j.archoralbio.2004.10.015.
15. Silva SRC, Fernandes RAC. Autopercepção das condições de saúde bucal por idosos. Rev Saúde Pública. 2001;35(4):349-55.
16. Silva DD, Sousa ML R, Wada RS. Autopercepção e condições de saúde bucal em uma população de idosos. Cad Saúde Pública. 2005;21(4):1251-9.
17. Benedetti TRB, Mello ALSF, Gonçalves LHT. Idosos de Florianópolis: autopercepção das condições de saúde bucal e utilização de serviços odontológicos. Ciênc Saúde Coletiva. 2007;12(6):1683- 90. doi: 10.1590/S1413-81232007000600029.
18. Akhter R, Hassan NM, Aida J, Zaman KU, Morita M. Risk indicators for tooth loss due to caries and periodontal disease in recipients of free dental treatment in an adult population in Bangladesh. Oral Health Prev Dent. 2008;6(3):199-207.
19. Bergdahl M, Bergdahl J. Low unstimulated salivary flow and subjective oral dryness: association with medication, anxiety, depression, and stress. J Dent Res. 2000;79(9):1652-8. doi: 10.1177/00220345000790090301.
20. Plati MC, Covre P, Lukasova K, Macedo EC. Depressive symptoms and cognitive performance of the elderly: relationship between institutionalization and activity programs. Rev Bras Psiquiatr. 2006;28(2):118-21. doi: 10.1590/S1516-44462006000200008.
21. Kressin NR, Reisine S, Spiro A 3rd, Jones JA. Is negative affectivity associated with oral quality of life? Community Dent Oral Epidemiol. 2001;29(6):412-23. doi: 0.1034/j.1600- 0528.2001.290602.x.
22. Friedlander AH, Norman DC. Late-life depression: Psychopathology, medical interventions, and dental implications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(4):404-12. doi: 10.1067/moe.2002.122434.0528.200 1.290602.x.
23. Friedlander AH, Friedlander IK, Gallas M, Velasco E. Late life depression: its oral heath significance. Int Dent J. 2003;53(1):41- 50.
24. Hugo FN, Hilgert JB, Corso S, Padilha DM, Bozzetti MC, Bandeira DR, et al. Association of chronic stress, depression symptoms and cortisol with low saliva flow in a sample of south-Brazilians aged 50 years and older. Gerodontology. 2008;25(1):18-25. doi: 10.1111/j.1741-2358.2007.00188.x.
25. Matsuda K, Ikebe K, Ogawa T, Kagawa R, Maeda Y. Increase of salivary flow rate along with improved occlusal force after the replacement of complete dentures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(2):211-5. doi: 10.1016/j. tripleo.2009.03.020.
26. Brasil. Ministério da Saúde. Secretaria de Políticas da Saúde. Departamento de Atenção Básica. Área Técnica de Saúde Bucal. Projeto SB 2000: condições de saúde bucal da população brasileira no ano 2000. Manual do Examinador. Brasília: Ministério da Saúde; 2001 [2009 Jan 26]. Disponível: < http://bvsms.saude.gov.br/bvs/publicacoes/condSB_man_exam.pdf>.
27. Caldas Junior AF, Figueiredo ACL, Soriano EP, Sousa EHA, Melo JBG, Vilela AS. Prevalência de cárie e edentulismo em idosos de Recife-Pernambuco-Brasil. Rev Bras Cienc Saúde. 2002;6(2):113-22.
28. Wolff A, Ofer S, Raviv M, Helft M, Cardash HS. The flow rate of whole and submandibular/sublingual gland saliva in patients receiving replacement complete dentures. J Oral Rehabil. 2004;31(4):340-3. doi: 10.1046/j.1365-2842.2003.01247.x.
29. Streckfus CF, Brown LJ ,Ship JA, Brunelle J. Stimulated parotid gland flow rates in healthy, elderly dentulous and edentulous individuals. J Prosthet Dent. 1993;70(6):496-9. doi: 10.1016/0022-3913(93)90261-L.
30. Ikebe K, Matsuda K, Morii K, Hazeyama T ,Kagawa R, Ogawa T, et al. Relationship between bite force and salivary flow in older adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(4):510-5. doi: 10.1016/j.tripleo.2006.12.006.
 Endereço para correspondência:
Endereço para correspondência:
E KURIHARA
e-mail: eduardokurihara@gmail.com
Recebido: 19/7/2010
Final version resubmitted on: 20/11/2010
Aceito: 15/3/2011
