










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.2 Porto Alegre Abr./Jun. 2013
CLÍNICO / CLINICAL
Endodontic management of dilacerated and bayonet shaped roots
Tratamento endodôntico de raízes dilaceradas e em forma de baioneta
Abhishek PAROLIAI; Manak KHOSLAII; Isabel Cristina Celerino de Moraes PORTOIII; Kundabala MALAIII
I Faculty of Dentistry, International Medical University. Jalan Jalil Perkasa 19 Taman Esplanade, 57000, Kuala Lumpur, Wilayah Persekutuan, Malaysia.
II Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences. Mangalore, India.
III Department of Restorative Dentistry, Cesmac University Center and Federal University of Alagoas. Maceió, AL, Brazil.
ABSTRACT
Successful root canal therapy requires a thorough knowledge of root anatomy and root canal morphology which may be quiet variable. The significance of internal root canal morphology has been emphasized by studies demonstrating that variations in canal morphology may affect the endodontic outcome. Consequently, in treating each tooth the clinician must assume that complex anatomy occurs often enough to be considered normal. Root dilaceration is one of the variations that may complicate the endodontic therapy. It is important for a clinician to have complete knowledge of internal anatomy relationships, careful interpretation of radiographs; proper access preparation and a detailed exploration of the interior of the tooth to achieve a successful treatment outcome. This paper reports successful endodontic therapy of severe dilaceration of the root of mandibular first molar and bayonet shaped root of maxillary first premolar and highlights the clinical considerations to be followed during the endodontic procedures to get the successful outcome.
Indexing terms: Dental pulp cavity. Root canal therapy. Tooth root.
RESUMO
Um tratamento de canal bem sucedido requer conhecimento profundo da anatomia da raiz dentária e morfologia do canal radicular, que pode ser variável. A importância da morfologia interna do canal radicular tem sido enfatizada por estudos que demonstram que as variações na morfologia do canal podem afetar o resultado do tratamento endodôntico. Consequentemente, no tratamento de cada dente, o clínico deve assumir que uma anatomia complexa ocorre com frequência suficiente para ser considerada normal. A dilaceração da raiz dentária é uma das variações que podem complicar o tratamento endodôntico. É importante para o clínico ter conhecimento completo das relações da anatomia interna, fazer uma interpretação cuidadosa de radiografias; preparar adequadamente o acesso e realizar uma exploração detalhada do interior do dente para conseguir um resultado de tratamento bem sucedido. Este artigo relata casos de terapia endodôntica bem sucedida de dilaceração severa da raiz do primeiro molar inferior e de raiz em forma de baioneta de um primeiro pré-molar superior e destaca as considerações clínicas a serem seguidas durante os procedimentos endodônticos para se obter êxito no tratamento.
Termos de indexação: Cavidade pulpar. Tratamento do canal radicular. Raiz dentária.
INTRODUCTION
The term dilacerations refers to an abrupt change in the axial inclination or curve in the crown or root of a tooth. It was first used by Tomes in 18481and refers to an angulation that may occur anywhere along the length of the tooth, that is, its crown, amelocemental junction, along the root, or by only involving the apex of the root1-2. The exact etiology of dilacerations is still controversial but the most accepted cause is mechanical trauma to the primary predecessor tooth3-6. However, this pathogenesis has been questioned7-8. The other possible contributing factors that have been proposed include the ectopic development of the tooth germ, presence of scar/ infection/ cyst/ tumour, developmental anomaly of tooth germ, lack of space, syndrome and hereditary factors9. The prevalence of dilacerations ranges from 0.32% to 7% but only 0.45% in mandibular first molar, mandibular third molars are affected most often, while the maxillary arch is affected more than the mandibular arch. Furthermore, permanent teeth are affected more frequently than primary teeth and posterior teeth more than anterior teeth with no gender predilection10-13. Dilaceration may occur bilaterally in some patients14. The recognition and diagnosis of a dilacerations are essential for any tooth that requires root canal therapy, as failure to diagnose root dilacerations contributes to higher rate of unfavourable outcome of endodontic treatment13. Although dilacerations of a crown can be observed visually in the oral cavity, radiographic examination is required to diagnose a dilacerated root. The direction of root dilacerations can be in single plane or two planes. If the root bends mesially or distally, the dilacerations can be clearly apparent on a periapical radiograph while in buccal / palatal (lingual) direction it gives bull's eye appearance. When the root dilaceration is in labial direction, it is called a scorpion tooth. If a tooth is doubly affected, it is called a bayonet dilaceration15. According to severity; dilaceration can be mild, moderate, or severe. This paper reports successful endodontic management of mandibular first molar with severe dilacerations of root at the apex and bayonet dilaceration in maxillary premolar.
CASE REPORT
Case 1
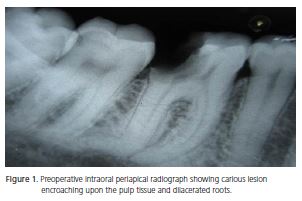
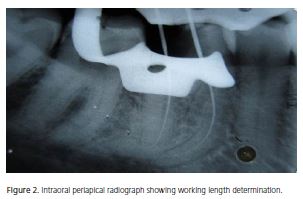
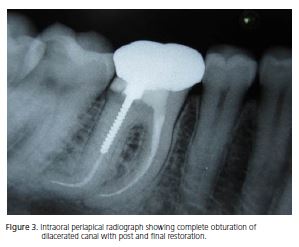
A 46 year old female patient reported to the clinic, with a chief complaint of pain on chewing in the lower right back tooth since last two weeks. Medical and family histories were noncontributory. Intraoral examination revealed a deep carious lesion with respect to the mandibular right first molar. On pulp status evaluation, the tooth showed no response with heat, cold and electric pulp tests (Parkell Electronics Division, Farmingdale, NY). The tooth was sensitive to percussion suggestive of symptomatic apical periodontitis. Intraoral periapical radiograph (IOPA) was advised and it revealed the presence of the coronal radiolucency involving the pulp, suggestive of caries perforating the pulp chamber with widening of periodontal ligament space confirming the diagnosis of symptomatic apical periodontitis. After careful reading of preoperative radiograph, presence of dilacerations was seen in distal root and severe curvature in mesial root of mandibular right first molar (Figure 1). Treatment plan was then formulated. Root canal therapy was advised for the mandibular right first molar (tooth 46). The tooth was anaesthetized with lignocaine 2% with epinephrine 1:100 000 and a conventional endodontic access opening was made using round carbide (ISO 014) and Endo-Z FG burs (Cavity Access Z Set, Dentsply Maillefer, Ballaigues, Switzerland) under rubber-dam isolation. Two canals, mesial and distal were located. Then to get the straight line access to the apical foramen the conventional triangular access was extended more mesially. Canal patency was established using # 10 K file. Working lengths were determined with a #15 K file by using the technique of Ingle and Bakland (Figure 2)16. The working lengths were kept 1 mm short of radiographic apex. It was decided to use flexible NiTi instruments. All rotary endodontic files were used using Tri Auto ZX, a cordless endodontic treatment handpiece (J. Morita USA, Inc.). For each file the individual torque limit and rotational speed (280 +/- 50 rpm) already programmed in the endodontic motor were used. RaCe endodontic instruments (FKG Dentaire, Swiss dental Products) were used in a crown down manner according to the manufacturer's instructions using a gentle in-andout motion to shape the root canals. Instruments were withdrawn when resistance was felt and changed for the next instrument. A 0.10 taper size 40 instrument was used to one third of the working length followed by 0.08 taper size 35 instrument to one third to one half of the working length (coronal third of the root canal). Subsequently 0.06 taper size 30 instrument was used to one half to two thirds and 0.04 taper size 25 instrument to two thirds of the working length (middle third). Further apical preparation of both root canal was done using Xtreme Race rotary instruments (FKG Dentaire, Swiss dental Products) in a sequence of 15/.02 > 20/.02 > 25/.02 to the full working lengths with periodic recapitulation of # 15 K flex file (Dentsply Maillefer, Ballaigues, Switzerland). The canals were thoroughly irrigated with 2.5% sodium hypochlorite, 17% aqueous solution of EDTA, 0.2%weight/volume chlorhexidine gluconate (Vishal Dentocare PVT, LTD, India) and saline as a final irrigant using 26 gauge needles. The canals were dried using sterile paper points (Dentsply Maillefer, Ballaigues, Switzerland). Calcium hydroxide powder (Raman Research, Kolkata, India) was mixed with propylene glycol, made into a paste, and placed in the root canals as the interim filling by using a lentulospiral (Dentsply Maillefer, Ballaigues, Switzerland). The access cavity was temporarily sealed with Cavit (3M ESPE, St Paul, MN, USA). The patient returned after one week, and the canals were then irrigated with 17% aqueous solution of EDTA and saline as a final irrigant to remove the remnants of the calcium hydroxide. The canal were dried using paper points (Dentsply Maillefer, Ballaigues, Switzerland) and obturated with previously selected guttapercha cones (Dentsply Maillefer, Ballaigues, Switzerland) and AH Plus sealer (Dentsply, DeTrey, GmbH, Konstanz, Germany) with the lateral and vertical compaction technique. Coronal cavity was temporarily restored using Cavit (3M ESPE, St Paul, MN, USA). In the next appointment post space preparation was done for the distal canal, and a prefabricated metal post (Produits Dentaires S.A., Switzerland) was cemented. The core build up was done using composite resin (3M ESPE, St, Paul, MN, USA). The final restoration was delivered in the form of porcelain fused to metal crown (Figure 3). One year follow up radiograph revealed successful healing.
Case 2
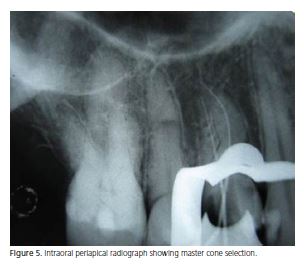
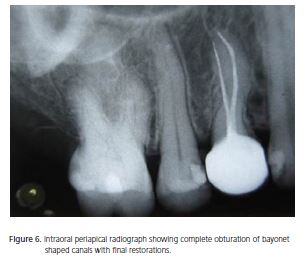
A 38 year old female reported to the department, with a chief complaint of decay in the upper right back tooth. The patient gave a history of severe pain since the last two days on drinking hot liquids. Medical and family histories were noncontributory. On intraoral examination, a deep carious lesion was seen in maxillary right first premolar (tooth 14). Pulp status was evaluated using heat test, cold and electric pulp tests (Parkell Electronics Division, Farmingdale, NY, USA). The tooth showed an exaggerated response to heat testing with lingering pain suggestive of symptomatic irreversible pulpitis. An intraoral periapical (IOPA) radiograph was advised for the tooth, which revealed the presence of a coronal radiolucency involving the pulp chamber, suggestive of caries encroaching upon the pulp tissue confirming the diagnosis of irreversible pulpitis. The roots were double curved (Bayonet or 'S' shaped) (Figure 4). Faulty restorations were seen on the proximal aspect of maxillary right canine (tooth 13) and second premolar (tooth 15), not involving the pulp chamber. Treatment plan was then formulated. Maxillary right first premolar was advised for endodontic therapy and maxillary right canine and second premolar were advised for re-restorations. The tooth was anaesthetized with lignocaine 2% with epinephrine 1:100 000 and a conventional endodontic access opening was made using round carbide (ISO 014) and Endo-Z FG burs (Cavity Access Z Set, Dentsply Maillefer, Ballaigues, Switzerland) under rubber-dam isolation. Canal patency was established using # 10 K file. Working lengths were determined by using the technique of Ingle and Bakland16, using #15 stainless steel K-files and the working lengths were kept 1 mm short of radiographic apex. Shaping and cleaning of the root canals were done using Xtreme Race rotary instruments (FKG Dentaire, Swiss dental Products) similarly as done in the case report 1. Coronal enlargement was done for both the canals using Pre-Race rotary instruments (FKG Dentaire, Swiss dental Products), which reduced the angle of curvature to the first curve, and enabled easier approach to the second curve. The canals were irrigated with 2.5% sodium hypochlorite, 17% aqueous solution of EDTA, 0.2% weight/volume chlorhexidine gluconate (Vishal Dentocare PVT, LTD India) and saline as a final irrigant using 26 gauge needles. The canals were dried using sterile paper points (Dentsply Maillefer, Ballaigues, Switzerland). Calcium hydroxide powder (Raman Research, Kolkata, India) was mixed with propylene glycol, made into a paste, and placed in the root canals as the interim filling by using a lentulospiral (Dentsply Maillefer, Ballaigues, Switzerland). The access cavity was temporarily sealed with Cavit (3M ESPE, St Paul, MN, USA). The patient returned after one week, and the canals were then irrigated with 17% aqueous solution of EDTA and saline as a final irrigant to remove the remnants of the calcium hydroxide. The canals were dried using sterile paper points (Dentsply Maillefer, Ballaigues, Switzerland), master cones were selected (Figure 5) and obturated with guttapercha cones (Dentsply Maillefer, Ballaigues, Switzerland) and AH Plus sealer (Dentsply, DeTrey, GmbH, Konstanz, Germany) using lateral and vertical compaction technique. The access cavity was cleaned with damped cotton pellet and then restored with composite resin (3M ESPE, St, Paul, MN, USA). Post-endodontic restoration was delivered in the form of porcelain fused to metal crown (Figure 6).
DISCUSSION The main goal of endodontic therapy is thorough chemomechanical debridement of the entire root canal system followed by a three-dimensional obturation with an inert filling material and a final coronal restoration, thereby preventing access to microorganisms. To achieve this goal it is necessary for the clinician to have thorough knowledge of root canal morphology and its variations. Root dilaceration is one of the variations that may complicate the endodontic therapy hence diagnosing it before endodontic treatment is an important objective for the successful outcome17. The criteria for recognizing root dilaceration vary in the literature. According to some authors a tooth is considered to have a dilacerations, if there is a 90-degree angle or greater along the axis of the tooth or root10-13, whereas others defined dilaceration as a deviation from the normal axis of the tooth of 20 degrees or more in the apical part of the root12. A frequent error that may occur during endodontic procedure in dilacerated root is the failure to maintain root canal curvature, resulting in ledge formation, apical transportation, zipping, perforation, and instrument breakage18. To avoid these mishaps, the basic principles of endodontic therapy must be followed, that is good preoperative radiograph, straight line access to apical foramen, pre-curving the endodontic hand instrument, file recapitulation, thorough irrigation and use of flexible Ni- Ti instruments9,19. Hence in the present cases all these principles were followed. Access cavities were modified to reach the apical foramen; enough tooth structure was removed to get the straight line access to apical foramen, giving the access cavity a cloverleaf appearance. This modified outline form of access cavity is known as shamrock preparation which allows the endodontic instrument unrestrained in the severely curved canals16. In dilacerated teeth it is often difficult to explore and negotiate the canal to its apical foramen; hence the use of scout file is recommended in these kind of cases19. In the present cases # 10k file was inserted in watch-winding motion to confirm the canal patency. After exploring the canal, crowndown sequence of instrumentation was followed, as early coronal flaring leads to greater tactile awareness of the apical constriction, reduce coronal binding of instruments, less risk of inoculation of endodontic pathogens into the periradicular tissues, enhance penetration of irrigant into the root canal system, less likelihood for a change in the working length measurement during preparation and more effective performance of electronic apex locators20. In the present cases NiTi Xtreme RaCe instruments (FKG Dentaire, Swiss Dental Product) were used. Reamer with Alternating Cutting Edges (RaCe) is NiTi endodontic rotary instruments having noncutting safety tip, non-threading blade with triangular section. RaCe instruments are supplied as easy RaCe and Xtreme RaCe. Easy RaCe is used in slight or moderately curved canals while Xtreme in severely curved root canals. Studies have shown that ccombination of triangular section, alternating cutting edges and flexibility of RaCe ensures efficient evacuation of chips and cutting debris, allows better penetration, effective cutting and maintains the original canal curvature21-23. Use of Tri Auto ZX automatic endodontic treatment handpiece is also very useful due to its three main functions: automatic start and stop, automatic torque reverse (automatically stops and reverses the rotation of the nickel titanium file when too much pressure is applied) and automatic apical reverse (automatically stops and reverses the rotation of the file when the file tip reaches a distance from the apex present by the clinician. In the present cases multiple visits approach was followed with the use of inter-appointment intracanal medicament using calcium hydroxide to ensure complete elimination of microorganisms. Calcium hydroxide was used with propylene glycol; a vehicle that allows calcium and hydroxyl ions to release slowly, enables them to remain in the periapical region for considerable time and thereby exerts a beneficial action24. Thereafter, root canals were obturated using lateral compaction technique. Flexible NiTi spreaders were used because they penetrate to greater depths and distribute forces more evenly than stainless spreader in severely curved canals16. Dilacerated teeth are uncommon but the presence of severe root dilacerations increases the risk of mishaps during the endodontic procedure. Hence thorough examination and sound treatment planning are strongly advocated. Clinicians should be aware of all the basic principles, modification and latest technology of endodontic therapy to manage these kinds of cases. 
A PAROLIA and M KHOSLA performed the endodontic therapy for these teeth, also contributed significantly in the preparation of the manuscript and its review. ICCM PORTO and K MALA supervised the implementation and systematic interpretation of the manuscript. They significantly contributed in the review of this manuscript. All authors have read and approved the final manuscript.
REFERENCES
1. Tomes J. A course of lectures on dental physiology and surgery. London: Gryphon Editions, Ltd.; 1846. [ Links ]
2. Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 4th ed. Philadelphia: WB Saunders; 1983.
3. Maragakis MG. Crown dilaceration of permanent incisors following trauma to their primary predecessors. J Clin Pediatr Dent. 1995;20(1):49-52.
4. Kearns HP. Dilacerated incisors and congenitally displaced incisors: three case reports. Dental Update. 1998;25(8):339-42.
5. Matsuoka T, Sobue S, Ooshima T. Crown dilaceration of a first premolar caused by extraction of its deciduous predecessor: a case report. Endod Dent Traumatol. 2000;16(2):91-4.
6. Prabhakar AR, Reddy VV, Bassappa N. Duplication and dilaceration of a crown with hypercementosis of the root following trauma: a case report. Quintessence Int. 1998;29(10):655-7.
7. Chadwick SM, Millet D. Dilaceration of a permanent mandibular incisor. A case report. Br J Orthod. 1995;22(3):279-81.
8. Stewart DJ. Dilacerated unerupted maxillary central incisors. Br Dent J. 1978;145(8):229-33.
9. Jafarzadeh H, Abott PV. Dilaceration: review of an endodontic challenge. J Endod. 2007;33(9):1025-30. doi: 10.1016/j. joen.2007.04.013.
10. Malcic A, Jukic´ S, Brzovic´ V, Miletic´ I, Pelivan I, Anic´ I. Prevalence of root dilaceration in adult dental patients in Croatia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(1):104-9. doi: 10.1016/j.tripleo.2005.08.021.
11. Udoye CI, Jafarzadeh H. Dilaceration among Nigerians: prevalence, distribution, and its relationship with trauma. Dent Traumatol.2009;25(4):439-41. doi: 10.1111/j.1600- 9657.2009.00796.x.
12. Chohayeb AA. Dilaceration of permanent upper lateral incisor frequency, direction, and endodontic treatment implications. Oral Surg Oral Med Oral Pathol. 1983;55(5):519-20. doi: 10.1016/0030-4220(83)90239-6.
13. Hamasha AA, Al-Khateeb T, Darwazeh A. Prevalence of dilaceration in Jordanian adults. IntEndod J. 2002;35(11):910-2. doi: 10.1046/j.1365-2591.2002.00593.x.
14. Lin L, Dowden WE, Langeland K. Bilateral dilaceration. J Endod.1982;8(2):85-7. doi: 10.1016/S0099-2399(82)80264-1.
15. Valladares Neto J, de Pinho Costa S, Estrela C. Orthodonticsurgical- endodontic management of unerupted maxillary central incisor with distoangular root dilaceration. J Endod. 2010;36(4):755-9. doi: 10.1016/j.joen.2009.12.032.
16. Ingle JI, Bakland LK. Endodontics. 5th ed. London: BC Decker Inc; 2002.
17. Cohen S, Burns RC. Pathways of pulp. 8th ed. St Louis: Mosby; 2002.
18. Walton RE, Torabinejad M. Principles and practice of endodontics. 2nd ed. Philadelphia: WB Saunders; 1996.
19. Dastmalchi N, Kazemi Z, Hashemi S, Peters OA, Jafarzadeh H. Definition and endodontic treatment of dilacerated canals: a survey of Diplomates of the American Board of Endodontics. J Contemp Dent Pract. 2011;12(1):8-13.
20. Saunders EM. Hand instrumentation in root canal preparation. Endodontic Topics. 2005;10(1):163-7. doi: 10.1111/j.1601- 1546.2005.00127.x.
21. Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2006;39(3):203-12. doi: 10.1111/j.1365-2591.2006.01075.x.
22. Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009;35(6):883-6. doi: 10.1016/j.joen.2009.03.007.
23. Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2004;37(4):239-48. doi: 10.1111/j.0143-2885.2004.00783.x.
24. Simon ST, Bhat KS, Francis R. Effect of four vehicles on the pH of calcium hydroxide and the release of calcium ion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.1995;80(4):459-64. doi: 0.1016/S1079-2104(05)80371-3.
 Endereço para correspondência:
Endereço para correspondência:
A PAROLIA
e-mail: abhishek_parolia@imu.edu.my
Received on: 4/4/2012
Final version resubmitted on: 9/8/2012
Approved on: 26/9/2012
